
Abstract
Background:
Deep location and neurovascular structures make access to lesions of the petrous apex a significant challenge. A novel approach for these tumors is the contralateral transmaxillary approach.
Clinical Presentation:
A 31-year-old male was evaluated for left abducens nerve palsy. Magnetic resonance imaging (MRI) and computed tomography revealed an enhancing, lytic lesion of the petrous apex with extension to the cavernous sinus and petroclival junction. The patient underwent a combined endoscopic contralateral transmaxillary and endoscopic endonasal transclival approach for resection of the lesion. No new or worsening neurologic deficits were noted following the procedure. Pathology revealed low-grade chondrosarcoma (grade I). Postoperative MRI revealed gross total resection of the lesion. Patient underwent adjuvant radiation therapy at the discretion of radiation oncology.
Conclusion:
The contralateral transmaxillary approach to the petrous apex allows for resection of lesions of the petrous apex with the ability to extend the dissection laterally. Excellent results achieved by institutions with advanced extended endoscopic endonasal experience can be reproduced in institutions with less experience. Further characterization of the risks and benefits of this approach is needed.
Keywords
Background
Surgical management of petrous apex lesions is challenging due to proximity of critical neurovascular structures, particularly the petrous internal carotid artery (ICA). 1 Transcranial approaches are effective and are still required with far lateral extension.2-5 Complications of open approaches include cranial nerve III-IX palsy, jugular foramen syndrome, infarcts, cerebrospinal fluid leak (CSF) leak, hydrocephalus, wound infection, pneumonia, and pulmonary embolism.2-5
Endoscopic endonasal approaches (EEAs) provide a less invasive alternative and obviate the need for durotomy and brain retraction which cause stroke, encephalomalacia, and seizures. 6 Endoscopic endonasal access to the lateral petrous apex is challenging due to anatomic limitations of working lateral and inferior to the petrous ICA, leading to worse outcomes and higher rates of recurrence. 7 The endoscopic contralateral transmaxillary (CTM) approach was developed to overcome this limitation. 8 In this report, we describe a patient with a petrous apex chondrosarcoma treated with the endoscopic CTM approach.
Clinical Presentation
A 31-year-old male presented with diplopia on left lateral gaze. On examination, he was found to have an isolated, incomplete left abducens palsy. He underwent computed tomography, which revealed an erosive left petrous apex lesion. Magnetic resonance imaging (MRI) with gadolinium revealed a contrast-enhancing left petrous apex lesion with extension to the petroclival fissure and cavernous sinus (Figure 1).
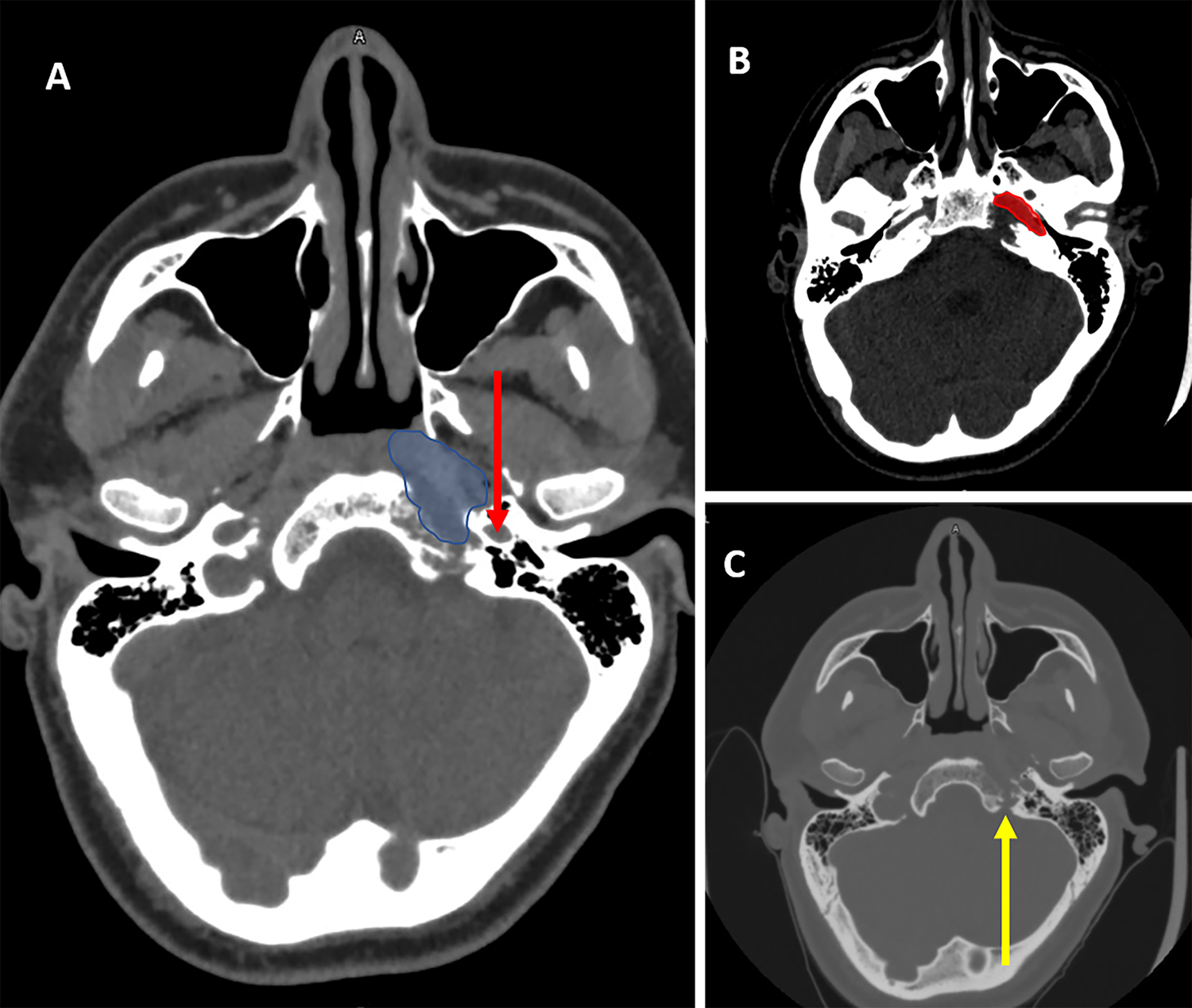
Preoperative imaging of erosive lesion of the petrous apex. A, Erosive lesion of petrous apex outlined in blue. Red arrow points to carotid canal. B, Extension inferior posterior and medial to the petrous internal carotid artery (ICA). Red region highlights lacerum segment of the ICA. C, Lower limit of dissection near hypoglossal canal bone uninvolved. Yellow arrow points to hypoglossal canal.
The patient underwent a CTM approach to the left petrous apex. The surgical procedure was uncomplicated, with no worsening of his abducens palsy. Postoperative gadolinium-enhanced MRI revealed gross total tumor resection. He had expected postoperative right infraorbital nerve hypoesthesia and stable diplopia but no oroantral fistula or epistaxis. The patient was transferred from the intensive care unit on POD 1 and discharged on POD 3. The only complications in the postoperative period were cacosmia, postnasal drainage, and Staphylococcus sinusitis which were treated with debridements and doxycycline around postoperative day (POD) 21 and POD 63. Postoperative gadolinium-enhanced MRI revealed gross total tumor resection.
Final pathology diagnosed a low-grade chondrosarcoma (grade I). Immunohistochemical stains were positive for S100 and negative for epithelial markers and Brachyury. There were no EWSR1 and NR4A3 gene rearrangements. The patient received adjuvant intensity-modulated radiation therapy, 70 Gy in 35 fractions over 51 days. By 9 weeks, he reported near-total resolution of diplopia (experienced only with extreme lateral gaze). By 12 weeks, he reported return of sensation in the distribution of the infraorbital nerve. Posttreatment positron emission tomography was obtained approximately 15 weeks following surgery and revealed no residual tumor, only enhancement of the nasoseptal flap (Figure 2).
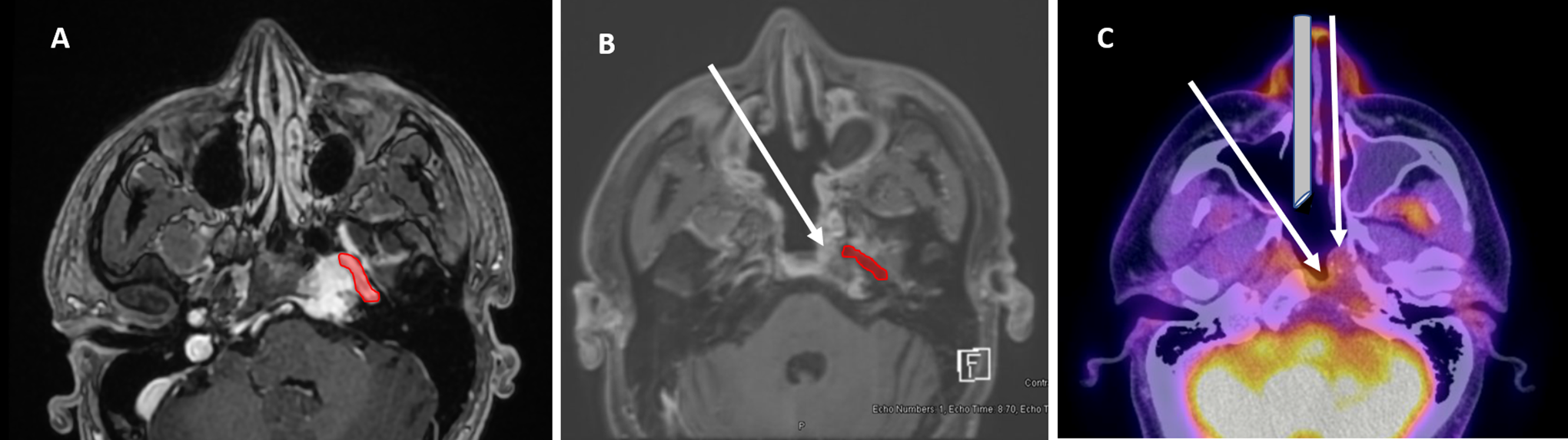
Pre- and posttreatment magnetic resonance imaging (MRI) and posttreatment positron emission tomography–computed tomography (PET-CT). A, Axial pretreatment, enhanced MRI. Petrous internal carotid artery (ICA) in red. B, Axial posttreatment, enhanced MRI. Petrous ICA in red. The arrow depicts reverse L-shaped nasoseptal flap. C, Axial, posttreatment PET-CT. Single arrows show the operative approach to the petrous apex afforded with the contralateral transmaxillary corridor compared to the transnasal corridor.
Operative Technical Note
Through a right sublabial incision, a Caldwell-Luc antrostomy was performed using a 4.0 coarse diamond drill. An inside-out medial maxillectomy was performed using a Kerrison rongeur by opening the natural os through the nasal fontanelle. Attention was then turned to the right naris. The posterior two-thirds of the inferior turbinate was resected via the CTM approach.
A standard endonasal transsphenoidal approach to the sella with resection of the right middle turbinate was performed in binarial fashion. Neuronavigation confirmed the locations of the left lateral opticocarotid recess, the paraclival ICAs, and the left Vidian canal. The dorsum sella, intercavernous sinuses, and the entire left parasellar ICA were exposed. Next, a transclival approach was performed. The left Vidian canal was identified and the Vidian nerve was followed toward the second genu between the paraclival and lacerum segment of the ICA. The tumor was encountered during this dissection around the carotid. As the floor of the sphenoid and lower clivus were dissected at the inferior tumor margin, the hypoglossal nerve was stimulated. Navigation was used to determine the location of the hypoglossal canal and preserve the nerve (see Figure 3, A1 and A2).
The tumor removal proceeded with ease in piecemeal fashion using suction and curettage through the CTM window and the contralateral naris. The angled endoscope was used both through the CTM window and the contralateral naris, with the advantage of the latter being to limit collisions between the surgeon and the endoscopist (see Figure 2C). The tumor tracked toward Dorello’s canal at the level of the sixth cranial nerve. A pinhole size durotomy was noted at this site. There was no injury to the sixth cranial nerve indicated by neuromonitoring during the dissection. Angled endoscopes through the CTM approach demonstrated no residual tumor in the petrous apex, around the lacerum segment of the carotid, or overlying the dura (see Figure 3, B1 and B2). Finally, the durotomy and CSF were sealed with Gelfoam and thrombin covered by a vascularized nasoseptal mucoperichondrial flap positioned in the clival recess. The sublabial incision was closed in 2 layers.
Discussion
Benet et al 6 described the extended EEA to the lower third of the clivus as the “far medial” approach. The advent of treating laterally situated lesions began with Jho and Ha 9 with exploration of the cavernous sinus. Endoscopic approaches to the petrous apex were first described by Kassam et al using the traditional binarial approach and subsequent lateral drilling of the petrous apex using angled endoscopes for lateral visualization. 10
Since then, transmaxillary approaches have been described for approaches to the infraorbital fossa, pterygopalatine fossa, and the lateral cavernous sinus.11,12 The addition of a sublabial transmaxillary approach (Caldwell Luc approach) or an anteromedial maxillotomy (Denker procedure) to a uninostril or binostril endonasal endoscopic approach has been shown to improve surgical freedom.
The CTM approach was recently developed to allow for improved lateral access in endoscopic approaches to the petrous apex.8,13 Compared to ipsilateral transmaxillary and transpterygoid approaches, the CTM approach increases surgical freedom and decreases the angle of attack to the petrous apex, thus improving the surgeon’s ability to work inferior, posterior, and lateral to the lacerum segment of the ICA. Recently, Snyderman et al 14 described their results in 29 patients treated with this approach, including a subset of patients with chondromatous tumors. They report gross total resection in 16 of 22 lesions. The group experienced 3 postoperative CSF leaks among 21 patients with intraoperative CSF leaks, 1 case of idiopathic sensorineural hearing loss, and 6 cases of hypoesthesia or neuralgia of the maxillary nerve which was generally transient. Per this review, the only other reports of this approach come from a case series and 2 case reports, with 3 of the 4 publications coming from the same institution.8,15,16
In this article, we describe the use of the CTM approach to the petrous apex in a tertiary academic center with minimal prior experience in expanded endoscopic approaches to the skull base. This report adds to the sparse literature examining this complex approach and attests to the reproducibility of prior results. As this was the first case at this institution, this patient was selected due to ideal tumor characteristics for this approach including, small, extradural, and hyperintense T2 imaging indicating easily resectable tumor. Despite the well-reported advantages of this approach, it should be used judiciously because of the learning curve associated with new techniques and complex surgical anatomy. 16
Conclusion
While endoscopic treatment of petrous apex tumors remains challenging, the CTM approach allows for improved surgical freedom and better visualization when working around the petrous carotid artery. The efficacy of this technique is demonstrated by its successful application in a growing skull base center. Further investigation of this surgical approach is needed to better define appropriate patient selection and risks/benefits of the procedure which has rare indications.
Supplemental Material
Supplemental Material, sj-docx-1-ear-10.1177_0145561320982161 - Contralateral Transmaxillary Approach for Resection of Chondrosarcoma of the Petrous Apex: A Case Report
Supplemental Material, sj-docx-1-ear-10.1177_0145561320982161 for Contralateral Transmaxillary Approach for Resection of Chondrosarcoma of the Petrous Apex: A Case Report by Jesse D. Lawrence, Robert Marsh and Meghan T. Turner in Ear, Nose & Throat Journal
Supplemental Material
Supplemental Material, sj-tif-1-ear-10.1177_0145561320982161 - Contralateral Transmaxillary Approach for Resection of Chondrosarcoma of the Petrous Apex: A Case Report
Supplemental Material, sj-tif-1-ear-10.1177_0145561320982161 for Contralateral Transmaxillary Approach for Resection of Chondrosarcoma of the Petrous Apex: A Case Report by Jesse D. Lawrence, Robert Marsh and Meghan T. Turner in Ear, Nose & Throat Journal
Footnotes
Authors’ Note
All authors contributed equally to this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.