
Abstract
Objective:
The primary objective of this study was to review the complication rate of percutaneous tracheostomies performed by a single surgeon in a community teaching hospital.
Methods:
This retrospective study reviewed the patients who underwent percutaneous tracheostomy with bronchoscopic guidance in a community hospital setting between 2009 and 2017. Patients older than the age of 18 requiring percutaneous tracheostomy were chosen for this retrospective study. Patients who were medically unstable, had no palpable neck landmarks, and inadequate neck extension were excluded. Indications for percutaneous tracheostomy included patients who had failed to wean from mechanical ventilation, required pulmonary toileting, or in whom airway protection was required.
Results:
Of the 600 patients who received percutaneous tracheostomy, 589 patients were included in the study. Intraoperative complication (2.6%) and postoperative complication rates (11.4%) compared similarly to literature reported rates. The most common intraoperative complications were bleeding, technical difficulties, and accidental extubation. Bleeding, tube obstruction, and infection were the most common postoperative complications. Overall burden of comorbidity, defined by Charlson Comorbidity Index, and coagulopathy were also found to be associated with higher complication rates. The decannulation rate at discharge was 46.3%.
Conclusion:
Percutaneous tracheostomy is a safe alternative to open tracheostomies in the community setting for appropriately selected patients.
Keywords
Introduction
Percutaneous tracheostomy (PT) is a widely accepted minimally invasive procedure that provides an alternative to the conventional surgical open tracheostomy (OT). 1 Percutaneous tracheostomy involves the insertion of a tracheal cannula into the lumen through a small skin incision without directly exposing the trachea and is commonly performed without the use of an operating room. The first descriptions of this procedure date back to 1626 by Sanctorius. 2 Contemporary PT was first described by Shelden et al in 1955, 3 then Toy and Weinstein in 1969, 4,5 followed by Ciaglia et al in 1985 who introduced percutaneous dilatational tracheostomy. 6 Over the years, percutaneous airway access methods and apparatus have been developed with bronchoscopic guidance, first being reported by Griggs et al in 1990, 7 which have significantly improved patient outcomes and decreased rate of complications. 8
The indications for PT are similar to those for conventional surgical OT, but the literature describes numerous advantages of PT, including shorter procedure duration, fewer complications, elimination of the risks of patient transfer, reduction of operating room scheduling conflicts, and improvement of intensive care unit (ICU) utilization. 9 -16 Studies have also identified intraoperative complications associated with PT such as death, hemorrhage, pneumothorax, and postoperative complications including bleeding, infection, and tracheostomy tube obstruction. 17 -22 However, surgical OT runs similar risks as well.
Debate between bedside PT and OT has been long-standing, and the method of tracheostomies remains as an area of controversy, especially in the community setting. Although there is strong evidence of PT and its favorable outcomes, the majority of the research comparing PT versus OT has been performed in large academic hospitals. 8,23 A meta-analysis with 14 prospective trials has shown similar results when comparing PT and OT, but all were set in university, academic settings. 23 The current evidence for PTs performed in community hospitals is minimal at best and requires further investigation.
This retrospective analysis looked to further strengthen the support for PT in the community setting. This study is based from Trillium Health Partners which is a large academically affiliated, community health center comprising of 3 hospitals to serve over 1 million residents in the Peel and West Toronto region in Ontario, Canada. The primary objective of this study was to assess the complication rates and outcomes of PT (including decannulation) with bronchoscopic guidance at a community teaching hospital. The secondary objective of this study was to identify patient characteristics that independently affect the complication and decannulation rates.
Materials and Methods
Patient Selection
This study was approved by the Trillium Health Partners Research Ethics Board (ID#825). This retrospective analysis included 600 consecutive patients who underwent PT at our community teaching hospital from November 2009 to May 2017. A single otolaryngologist performed or supervised all interventions. Patients older than the age of 18 and those who had appropriate indications for the procedure including failure to wean from mechanical ventilation, airway protection, and pulmonary toileting were eligible for the study. Those who were medically unstable, did not have any palpable neck landmarks (ie, cricoid or thyroid cartilage), and had limited neck extension were excluded from this study. Those who were not eligible for PT underwent open tracheostomies.
Tracheostomy Technique
All percutaneous tracheotomies were performed using the Ciaglia Blue Rhino single dilator kit (Cook Critical Care Inc) with bronchoscopic guidance. Patients were intubated in all cases prior to PT. Vital signs were monitored during the procedure. Intravenous sedation and neuromuscular paralytic agents were administered by the intensivist or anesthesiologist. Flexible bronchoscopy was performed by the intensivist or anesthesiologist present. A respiratory therapist was also present to bag-ventilate the patient. Along with the Ciaglia Blue Rhino kit, an OT set as well as a difficult intubation kit were also available at the bedside.
The operation was carried out in the patient’s ICU bed with the bed maximally inflated. The patient was positioned with adequate neck extension, prepped, and draped as for a standard tracheostomy procedure. After identification of appropriate surface landmarks, 1% xylocaine with 1:100 000 epinephrine was injected at the incision site and a vertical incision was made in the anterior neck. Blunt dissection was carried out down to the level of the trachea clearing most of the subcutaneous tissue. The endotracheal tube was then withdrawn partially and under bronchoscopic guidance, an introducer needle was inserted into the trachea with direct visualization. The needle is withdrawn and a guide wire was then inserted through the needle introducer catheter. Using a Seldinger technique, a 14F dilator was inserted to dilate the tracheostomy site. A blue rhino dilator was then used to further dilate the tracheostomy site. A Shiley #6 or #8 regular (sometimes extra-long proximal or extra-long distal) tracheostomy tube (the choice for the size of the tracheostomy tube is patient dependent) was inserted and sutured in place using silk sutures.
Variables
Demographic and clinical data were collected retrospectively. General patient demographics were recorded including age, gender, body mass index (BMI), admitting diagnosis, comorbidities, Charlson Comorbidity Index (CCI) scores, admission date, length of stay, and discharge destination. Preoperative laboratory data including hemoglobin (Hgb), platelets, international normalized ratio (INR), and partial thromboplastin time (PTT) values were also extracted. Indications for intubation and tracheostomy, size of tracheostomy, time between receiving the tracheostomy consultation and the procedure, peri or postoperative complication, decannulation status, and patient outcome (no complication, complication or death) were also collected. The complications were further subcategorized into bleeding, infection, accidental extubation, accidental decannulation, cuff-related incidents, desaturation, false passage, subcutaneous emphysema, pneumothorax, tube obstruction, posterior wall injury, technical difficulties, conversion to OT, other, and death.
Analysis
Descriptive statistics were performed on the demographic and other clinical variables, expressed as mean ± standard deviation or frequency. Charlson Comorbidity Index frequencies were grouped depending on mortality rates. 24 Complication rates were calculated for both perioperative and postoperative complications in patients who received PT. Perioperative and postoperative complication rates were calculated for the subcategories as well. Chi-square test and t test were used to analyze the association between complication and decannulation rates with clinical variables. Univariate and multivariate logistic regression analysis were also used to test how clinical variables affect complication and decannulation rates. Before conducting the logistic regression analyses, some variables were rescaled for meaningful interpretation of the results. Statistical significance was decided at a 5% significance level. All statistical analyses were conducted using R statistical software, version 3.3.3.
Results
This retrospective study reviewed 600 patients who underwent PT at our community teaching hospital from 2009 to 2017. Of the 600 patients reviewed, 589 patients were included in this study based on inclusion and exclusion criteria. The demographic distribution can be seen in Table 1. The study population included 350 (59.4%) male and 239 (40.9%) female patients. The mean age was 67 ± 14.9 years. Majority of patients had a BMI that classified them as overweight (BMI 25-29.9; 31%) or obese (BMI ≥30; 29.6%). Charlson Comorbidity Index scores were categorized according to the mortality rates. 24 The majority of patients had a CCI score that correlated with more than 25% mortality rate or higher (Table 1).The most common indication for tracheostomy was prolonged intubation (intubation exceeding 7 days), 25 followed by failure to extubate (inability to maintain spontaneous breathing after removing an artificial airway, requiring reintubation within 24-72 hours), 26 airway protection, and pulmonary toileting/secretions. The average length of stay in the hospital was 82.4 days, and the average length of days from admission to tracheostomy was 18.9 days. Three hundred and eighty patients either were discharged home or to long-term care, and 46.3% of those patients were decannulated at the time of discharge.
Demographic Data.
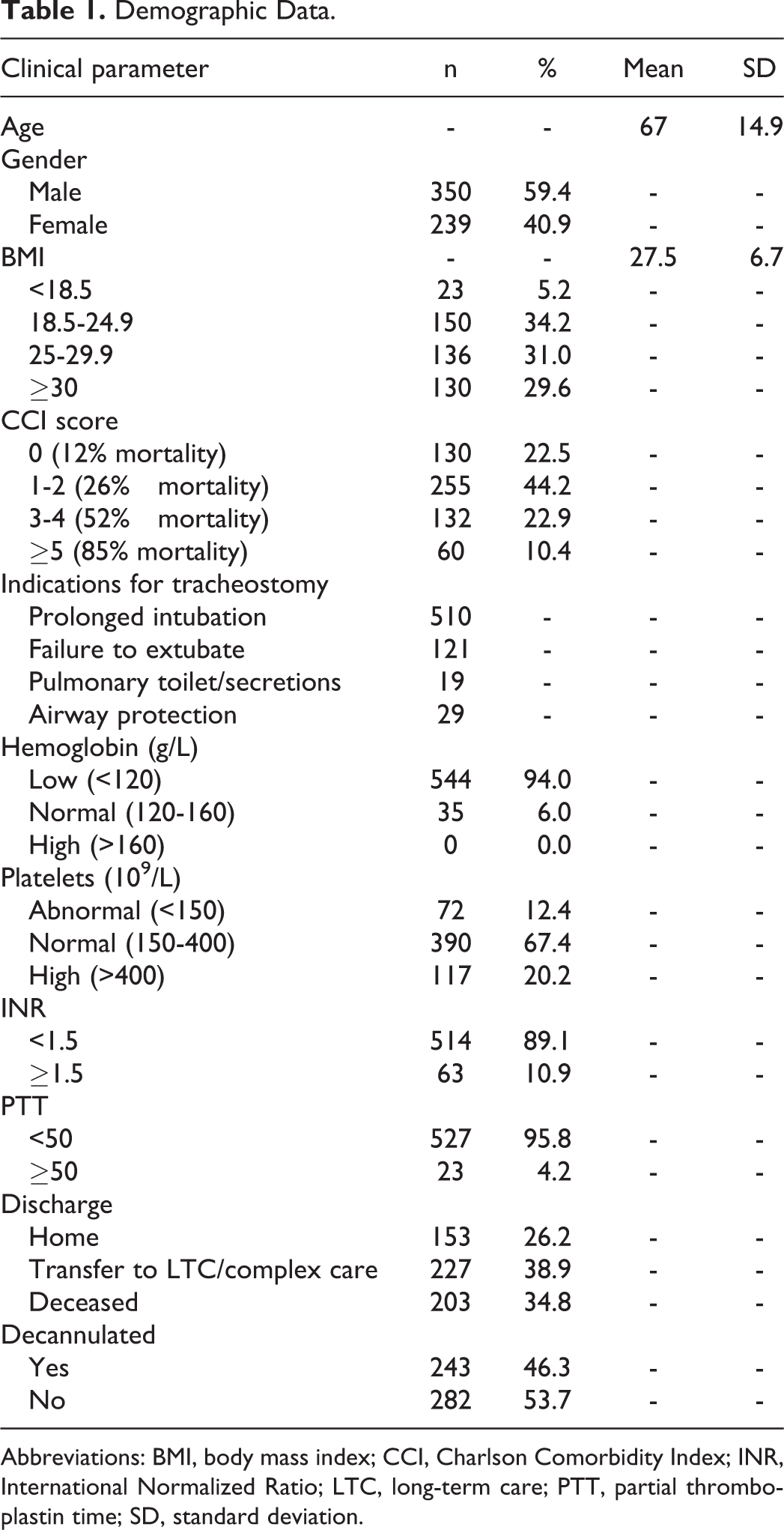
Abbreviations: BMI, body mass index; CCI, Charlson Comorbidity Index; INR, International Normalized Ratio; LTC, long-term care; PTT, partial thromboplastin time; SD, standard deviation.
Of 589 patients reviewed, a total of 80 patients had one or more complications. The perioperative complication rate was 2.6% and postoperative complication rate was 11.4% (Figure 1). The most common perioperative complications were bleeding (5; 33%), technical difficulties (4; 27%), and accidental extubation (2; 13%). The most common causes of postoperative complications were bleeding (19; 29%), tube obstruction (15; 23%), and infection (10; 15%). There were no deaths due to either perioperative or postoperative complications specific to PT; patient deaths reported were due to other causes unrelated to the tracheostomy.
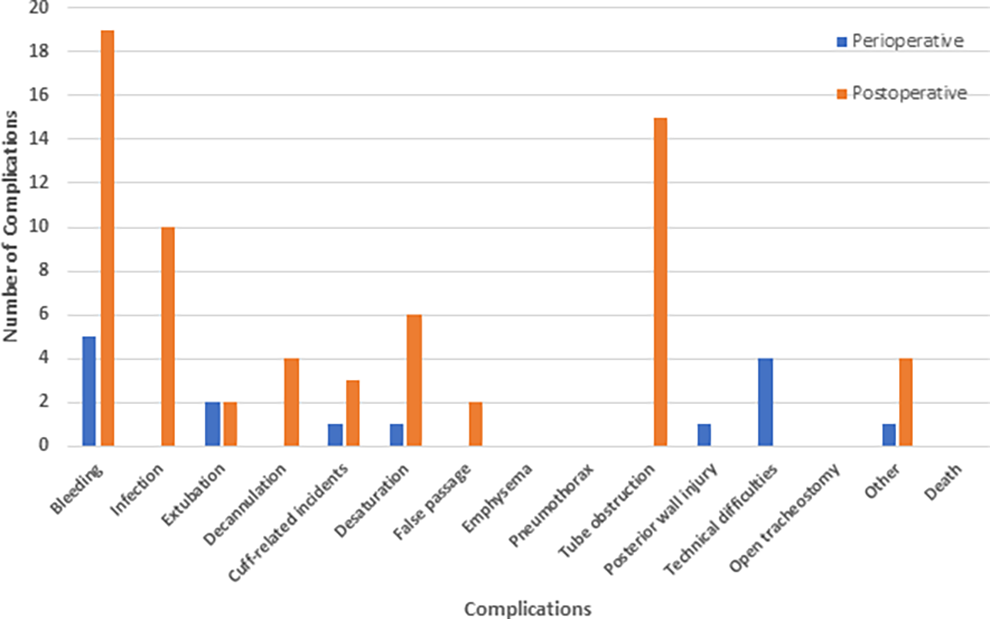
Frequency of perioperative and postoperative complications of percutaneous tracheostomy. Perioperative complication rate was 2.6%, and postoperative complication rate was 11.4%.
The association between incidence of complications and several patient characteristics was also examined (Table 2). Patients having complications were more likely to have a low platelet count compared to patients with no complications (270 vs 300; P < .05). Age, Hgb, INR, PTT, CCI score, and gender did not differ significantly between complications and noncomplications groups. However, it was observed that patients with complications are likely to be little older compared to patients with no complications (70.1 vs 66.2, P = .03). Similarly, the association between decannulation status and patient characteristics was examined (Table 3). Patients who were discharged with tracheostomy tube were more likely to have low Hgb values (91.1 vs 94.3; P = .01), be older (68.7 vs 65.3; P = .01), and have high INR values (1.26 vs 1.20; P < .01) compared to patients who were decannulated at discharge.
Association Between Complications and Clinical Parameters.a
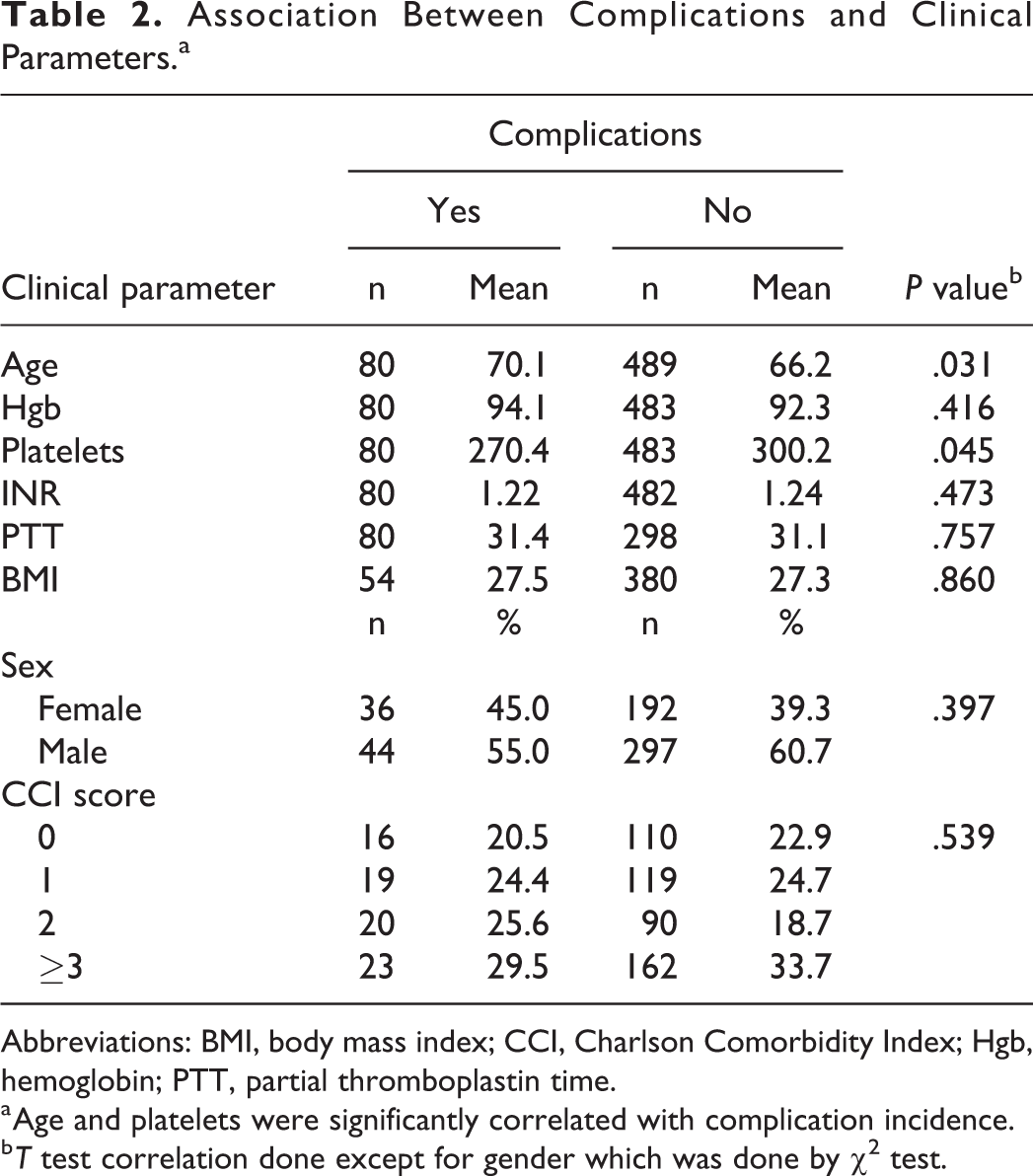
Abbreviations: BMI, body mass index; CCI, Charlson Comorbidity Index; Hgb, hemoglobin; PTT, partial thromboplastin time.
a Age and platelets were significantly correlated with complication incidence.
b T test correlation done except for gender which was done by χ2 test.
Association Between Decannulation and Clinical Parameters.a
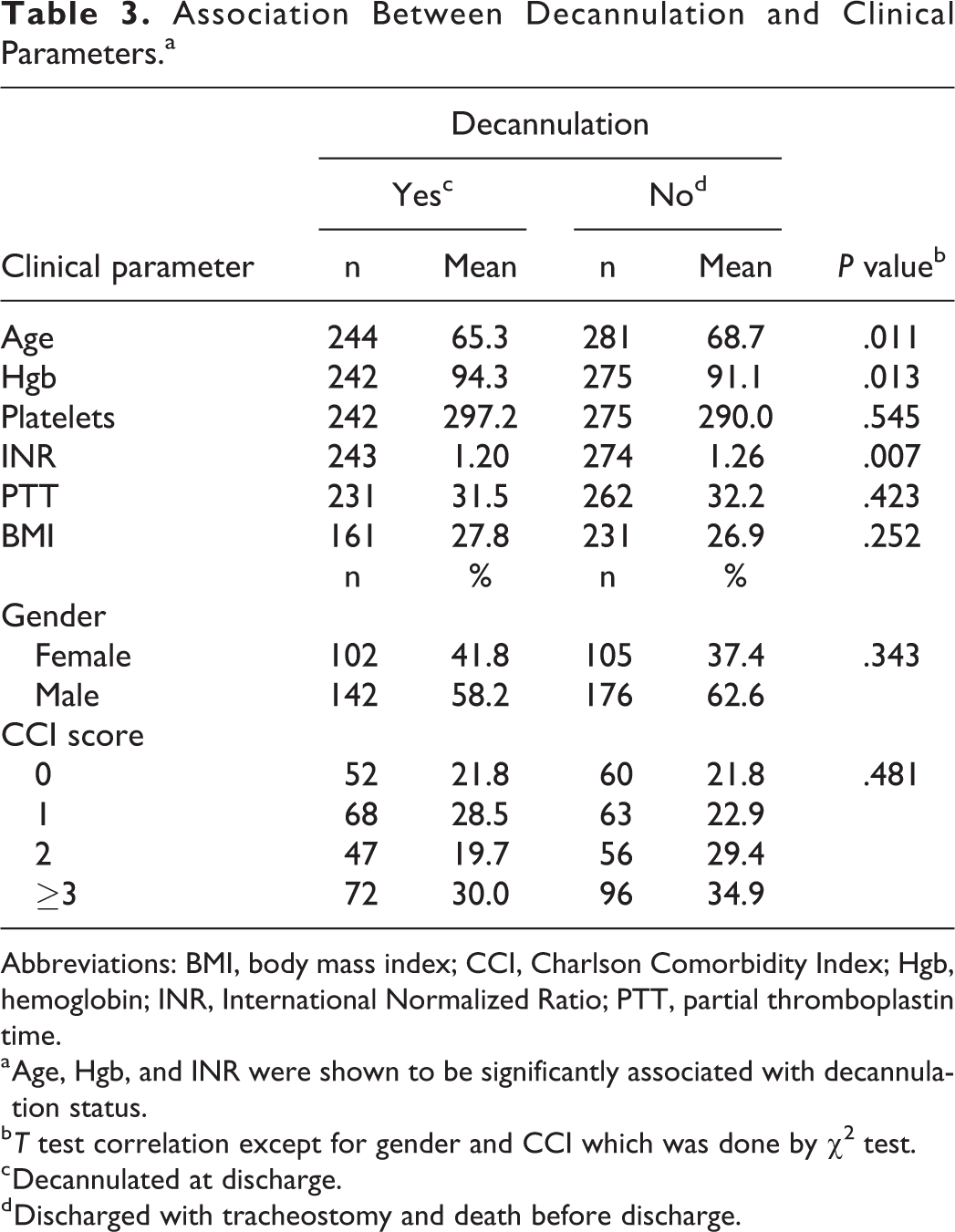
Abbreviations: BMI, body mass index; CCI, Charlson Comorbidity Index; Hgb, hemoglobin; INR, International Normalized Ratio; PTT, partial thromboplastin time.
a Age, Hgb, and INR were shown to be significantly associated with decannulation status.
b T test correlation except for gender and CCI which was done by χ2 test.
c Decannulated at discharge.
d Discharged with tracheostomy and death before discharge.
Lastly, logistic regression analysis was used to test how clinical variables affect complication incidence (Table 4) and decannulation status upon discharge (Table 5). Multivariate regression analysis was done to see the affects of age, gender, Hgb, platelets, INR, PTT, CCI score, and BMI on the measuring variables. Univariate analysis showed that age was the only significant predictor affecting complication after the tracheostomy. For each 10-year increase of age, the odds of being discharged with a tracheostomy tube increased by 20% (P < .05). However, when controlling for other factors using a multivariate analysis, age was no longer a significant contributor to complication status (P = .24).
Prognostic Factors Affecting Complications.a
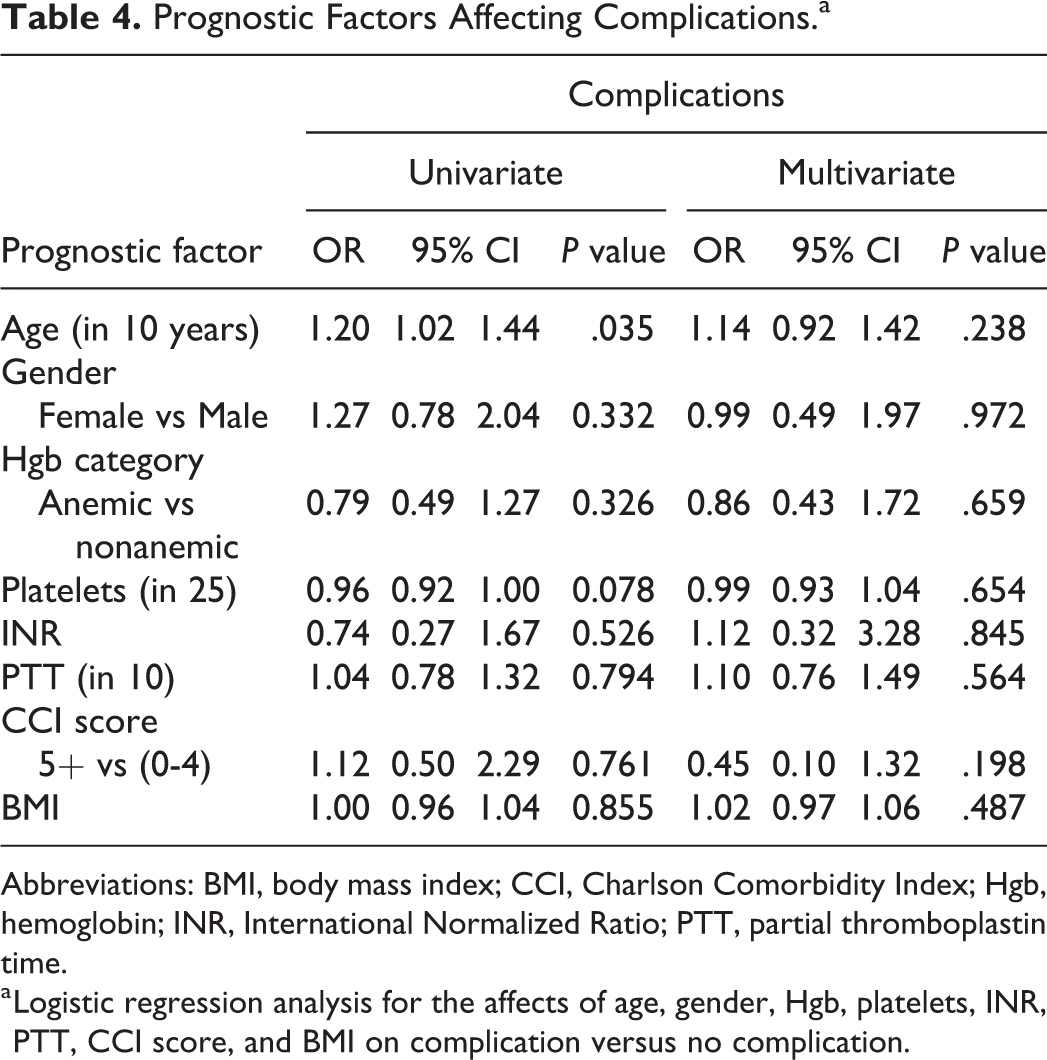
Abbreviations: BMI, body mass index; CCI, Charlson Comorbidity Index; Hgb, hemoglobin; INR, International Normalized Ratio; PTT, partial thromboplastin time.
a Logistic regression analysis for the affects of age, gender, Hgb, platelets, INR, PTT, CCI score, and BMI on complication versus no complication.
Prognostic Factors Affecting Decannulation.a
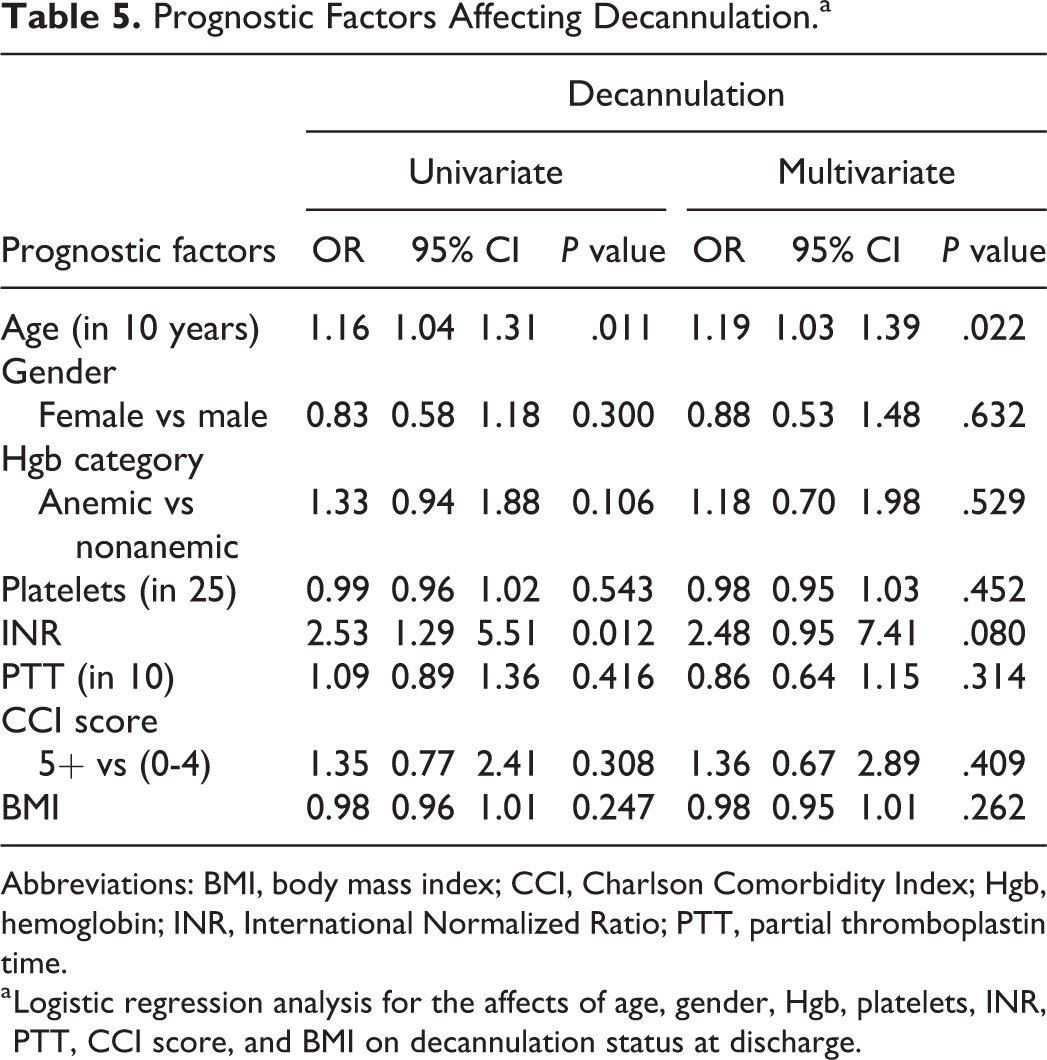
Abbreviations: BMI, body mass index; CCI, Charlson Comorbidity Index; Hgb, hemoglobin; INR, International Normalized Ratio; PTT, partial thromboplastin time.
a Logistic regression analysis for the affects of age, gender, Hgb, platelets, INR, PTT, CCI score, and BMI on decannulation status at discharge.
Univariate analysis showed that age and INR were significant predictors affecting decannulation prior to discharge. For each 10-year increase of age, the odds of discharging with tracheostomy versus decannulation at discharge increased by 16% (P = .01). The odds of discharging with tracheostomy was 2.53 times greater for each increase of INR by 0.1 (P = .01). Age was still a significant (P = .02) predictor for discharging with tracheostomy in the multivariate model after adjusting for gender, Hgb, platelets, INR, PTT, CCI score, and BMI. INR exhibited a trend toward significance (P = .08) with the odds of discharging with tracheostomy is 2.48 times greater for each increase of INR by 0.1.
Discussion
A recent meta-analysis showed no difference between PT and open tracheostomies in terms of complication rates, 27 reinforcing the notion that PT is a safe alternative to its surgical counterpart. However, research into its feasibility and efficacy within community teaching hospitals is lacking. This retrospective study reviewed the experience of PT done in a single community setting by one otolaryngologist.
Overall, the total complication rate compared similarly to the rates reported in the literature. 8 Perioperative complication rates were low at 2.6%, highlighting the safety of the procedure performed at this institution. However, this study reviews the experience of one surgeon including supervised procedures by the same surgeon. It has been shown that there is a learning curve in performing percutaneous dilatational tracheostomies, with reduced complication rates in operators who have performed at least 20 cases of PT. 28 Accordingly, surgeons with the fewest tracheostomy volumes were found to have higher complication rates. 29 Furthermore, postoperative complications occurred more frequently than perioperative complications at a rate of 11.4%. Although the rate was higher, the complications were rather minor ones, and there were no deaths due to complications of PT. Overall, PT was shown to be safe for patients at this community hospital.
It was traditionally thought that several patient characteristics including obesity, coagulopathy, and limited neck mobility were relative contraindications to the procedure. 30 Only recently has the literature identified PT to be safe within such clinical parameters. 30 -33 In fact, a retrospective analysis has shown no significant difference in bleeding between coagulopathic patients (INR ≥1.7 or platelet count ≤50k) and those without coagulopathy. 34 When comparing the complications with the clinical parameters in our study, age and platelet count had statistically significant correlation with complication occurrence. Age, Hgb, and INR were associated with decannulation status as well. Although no variables except age was associated with complications in our multivariate analysis, INR was a significant contributor to decannulation status for patients on their discharge. As bleeding was the most common perioperative and postoperative complication, it is consistent with our findings of platelets and INR being significantly associated with adverse outcomes since they are associated with primary and secondary hemostasis. Perhaps optimizing coagulation status in patients will improve both perioperative and postoperative patient outcomes. However, of the 24 patients who had either perioperative and/or postoperative bleeding, only 5 had abnormal platelet levels, INR or both. Of those 5 patients, 2 patients had platelet levels below 50 000, but were later discharged from hospital without other issues. One of the 5 patients had an INR of 2.1 and died of other complications unrelated to the tracheostomy. Considering the overall low complication rates of PT in this study—even with low platelet and high INR levels—it supports the current thought of reconsidering coagulopathy as a contraindication for PT.
There is some discrepancy on the increased risk of complications of PT with obesity 30,33 in the literature. Although some suggest a significant increase in the risk of complication after PT and surgical tracheostomies in obese patients—as much as a 4.9-fold increased risk 35,36 —others have shown no difference between obese and nonobese groups in terms of complication rates. 8 Our study consisted of 136 (31%) overweight patients (BMI 25-29.9 kg/m2), and 130 (29%) obese patients (BMI ≥30 kg/m2). However, the perioperative and postoperative complication rates remained low. Furthermore, BMI was not associated with either complication occurrence or decannulation status. Although there were missing data on BMI due to inconsistencies in patient charting, one explanation for this finding can be attributed to the experience and expertise of the surgeon. This further suggests the notion that the safety of PT in obese patients can be somewhat mitigated with sufficient technical experience. As other specialists including intensivists and anesthesiologists are equipped to perform PT, a comparison between specialties will help measure the affect of technical experience on outcome in difficult patient population.
Advanced age was also another factor that was associated with complications and decannulation status. Geriatric population is defined as age older than 65. 37 In fact, the average age of our patient population was 67 years old and 347 of our patients were older than the age of 65. In these patients, the coexistence of age-related risk factors and comorbidities may lead to a negative impact on patient outcome and complications. For example, increased age may lead to inadequate neck extension, which is a relative contraindication to the procedure since it can lead to difficulty performing the procedure. 38 Furthermore, a large portion of our patients had high CCI scores indicating an increased burden of comorbidities and mortality risk. For instance, there were a total of 192 patients with CCI scores correlating with mortality rates higher than 50%. Regardless of the high CCI scores, they were not significantly associated with either complication incidence or decannulation status. This suggests that although age exists as a nonmodifiable risk factor and comorbidities are present in older adult patients, PT can still be performed safely in the elderly population.
There were some limitations to this study. One was the fact that the surgery was done or supervised by one surgeon which restricts the generalizability of the findings. The procedures were all supervised by the same surgeon, but the level of supervision was not recorded. Thus, interrater reliability between different trainee surgeons on their effects on clinical outcome could not be assessed. There were also some missing data due to inconsistencies with patient charting over several years which is a limitation of a retrospective cohort study. BMI was an example of missing data which limited our ability to truly assess its association with outcome. A major advantage of our study was the large population size, and to our knowledge, represents the largest published case series of PT by a single surgeon. Although literature on PT in community teaching institutions is scarce and further research is required, this large sample size will hopefully represent what is experienced in the community.
Conclusion
In summary, our findings show that PT is a safe alternative to surgical tracheostomy, similar to the literature findings for academic settings. In general, the complication rates were low, with the majority of them minor ones. The low complication rates compared to high CCI scores indicate that PT in a community setting is safe even when patients have multiple medical comorbidities or risk factors (eg, coagulopathies, BMI). To the best of our knowledge, this represents the largest published series of PT performed in a community hospital setting. We plan to design a database to prospectively collect demographic and surgical information to enhance our understanding of this procedure with long-term follow-up for these patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Harry Barberian Grant, Department of Otolaryngology–Head and Neck Surgery, University of Toronto.