
Abstract
Background:
Increased frailty has been associated with worse outcomes in various surgical specialties. In endoscopic endonasal skull base surgery (EESBS), the relationship between frailty and outcomes has been examined to some degree.
Objective:
This scoping review aimed to consolidate the current literature, analyzing relationships between frailty and EESBS postoperative outcomes.
Methods:
A scoping review of frailty in EESBS was conducted on PubMed, Cochrane Library, Ovid Medline, Web of Science, Embase, and Google Scholar. Initial search yielded a total of 408 articles, which were reduced using the PRISMA model. Four studies published between 2020 and 2023 fit the inclusion criteria for this review.
Results:
A total of 1306 patients were captured with an average age of 54.1 years. All studies discussed modified frailty index-5 (mFI-5). Two studies utilized American Society of Anesthesiologists (ASA) classification, and 3 studies examined Charlson Comorbidity Index (CCI) as additional frailty measures. Higher mFI-5 was significantly associated with prolonged length of stay and readmission. Higher ASA was significantly associated with increased rates of Clavien-Dindo IV complications and permanent postoperative diabetes insipidus. CCI was not associated with any of the postoperative complications studied. Frailty was not strongly associated with worsened surgical complications, endocrine dysfunction, visual outcomes, and quality of life after EESBS.
Conclusion:
Frailty may serve as a useful tool in anticipating certain postoperative outcomes following EESBS. However, further research is necessary examining frailty specifically within endoscopic endonasal approaches to the skull base, rather than open or microscopic approaches. In addition, future studies need to be consistent in which frailty indices are used, and how frailty data are analyzed for effective conclusions to be made.
Keywords
Introduction
In recent decades, there has been a steady increase in the elderly population due to advances in health care and longevity. 1 It has become more relevant and important to identify predictors of clinical outcomes outside of age alone. Frailty is defined as multisystem impairment due to the depletion of physiologic reserves, which in turn results in increased vulnerability of the individual. 2 Frail patients are overall at a high risk of developing negative health-related events. 2 In the surgical literature, increased frailty is associated with poor outcomes following various operations within specialties such as neurosurgery, orthopedic surgery, gynecology, cardiothoracic surgery, and trauma surgery.2 -7 Within otolaryngology, frailty has been shown to predict patient morbidity and mortality in head and neck surgery.2,8 -11
In the past few decades, endoscopic endonasal skull base surgery (EESBS) has largely replaced more traditional open or microscopic approaches to midline, anterior skull base lesions.12,13 Given the demonstrated safe and effective clinical outcomes of EESBS, the field continues to broaden its use for various indications. However, in the elderly population, there is concern for increased complication rates after EESBS compared with those in young healthy patients.14,15 Kenning and Pinheiro-Neto utilize a case report to underscore the concern for potential increased perioperative morbidities and complications such as high flow cerebrospinal fluid (CSF) leak and subdural hematoma specifically in elderly patients undergoing EESBS. 15 Wilson et al examined tumor characteristics and postoperative outcomes specifically in elderly patients undergoing endoscopic endonasal pituitary surgery. 14 The cohort of patients who were 70 years or older were found to have a larger average tumor diameter and experienced a significantly-higher complication rate than the cohort of patients aged 60 to 69 years old. 14 With the expansion of EESBS to the elderly, it has become important to understand frailty to better serve this patient population.
The ability to predict patient outcomes after EESBS more precisely is an important area of increasing investigation. Frailty is an objective method of assessing patient comorbidities and relative risk factors prior to surgical procedures. 2 A comprehensive and holistic understanding of patient-specific risk factors in predicting EESBS outcomes facilitates a stronger patient-centered preoperative discussion, enhances patient education, and clarifies care team expectations. This scoping review provides a consolidated summary on the current literature surrounding frailty and its association with postoperative outcomes following EESBS.
Materials and Methods
Inclusion Criteria
The following databases were used in this scoping review (Figure 1): PubMed, Cochrane Library, Ovid Medline, Web of Science, Embase, and Google Scholar. The following search term was agreed on by the authors to encompass as many studies as possible relating to frailty and skull base surgery: ((Frailty) OR (modified frailty index) OR (mFI) OR (mFI-11) OR (mFI-5)) AND ((pituitary adenoma) OR (transsphenoidal) OR (pituitary surgery) OR (pituitary tumor) OR (transnasal transsphenoidal) OR (sellar mass) OR (suprasellar mass) OR (endoscopic skull base) OR (cerebrospinal fluid leak) OR (endoscopic endonasal skull base)). Studies with any methodology and from any year were included. Our initial inclusion criteria were intentionally broad to capture as many articles as possible. Any article that contained any mention of frailty and skull base or pituitary surgery were included. The initial search performed on October 26, 2023, yielded 408 publications between the years 1953 and 2023.
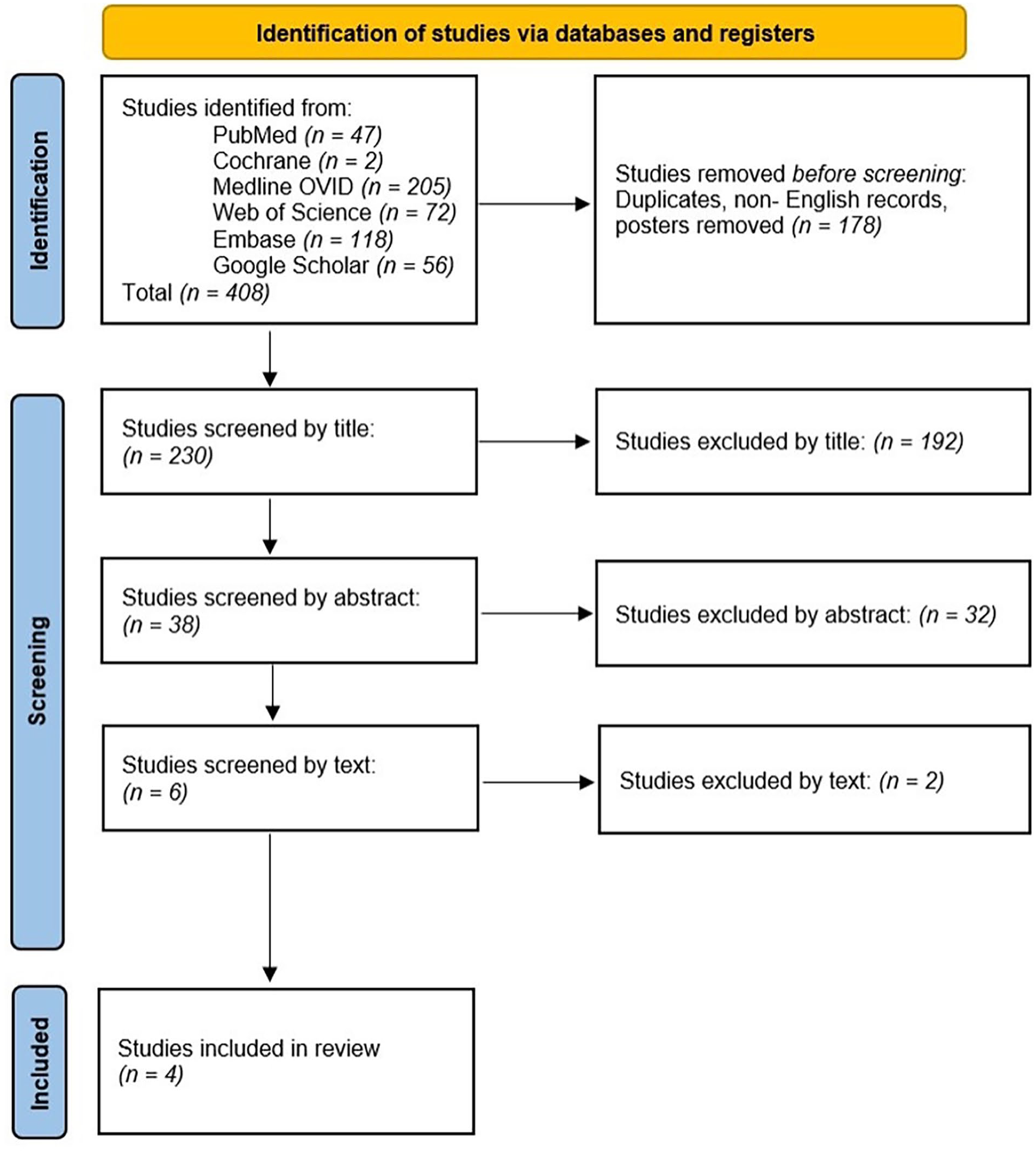
PRISMA flow model demonstrating article collection and screening process for this systematic review. 18
Exclusion Criteria
Exclusion criteria were then applied during the article screening process (Figure 1). Duplicates, abstract-only results, slideshow presentations, poster-only results, and non-English articles were excluded. Articles were also excluded if they were not peer reviewed. Given that outcomes and complications are known to substantially differ depending on the tumor pathology, tumor location, and surgical approach (endoscopic vs microscopic vs open),12,16,17 a study was excluded if it examined only non-endoscopic approaches, or if it aggregated multiple approaches (endoscopic, microscopic, and/or open) in 1 group without explicitly analyzing frailty within endoscopic-only patients.
Article Screening Process
The article screening process followed a Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) model (Figure 1). 18 After duplicates, abstract-only results, slideshow presentations, poster-only results, and non-English articles were excluded, 230 articles remained. These articles were then screened by title, yielding 38 articles. When examining the title, if it was readily obvious that the article had no relevance to frailty and skull base surgery, the study was excluded. Two authors (S.Y.C. and S.E.O.) then independently screened these 38 articles by reading each abstract. If it was exceedingly evident that the article had no relevance to frailty and specifically EESBS based on the abstract, the article was excluded. This process yielded a total of 6 eligible studies. Authors S.Y.C. and S.E.O. then independently reviewed the full-length texts of these 6 studies. Four articles were ultimately included in the present scoping review after all exclusion criteria were applied.
Data Collection
Each of the 4 articles included in this scoping review discussed frailty in the context of endoscopic endonasal anterior skull base surgery. Information including article titles, authors, date of publication, methodology, indication for surgery, number of patients, and frailty indices examined were collected. Data regarding postoperative outcomes were collected when available. Medical complications reported included myocardial infarction (MI), cerebrovascular accident (CVA), diabetes insipidus (DI), pneumonia, pulmonary embolism (PE), vision loss, hypoglycemia, cardiac arrest, vascular injury, seizure, venous thromboembolism (VTE), meningitis, sepsis, and stroke. A collective group of intensive care unit (ICU)-level Clavien-Dindo IV (CDIV) complications were also specifically reported and included cardiac arrest, MI, failure to wean off ventilation >48 hours, renal failure requiring dialysis, sepsis with end organ failure, PE, unplanned reintubation. Non-CDIV medical complications reported included hyponatremia/hypoosmolality, deep vein thrombosis (DVT), pneumonia, urinary tract infection (UTI), and renal insufficiency not requiring dialysis. Data regarding postoperative surgical complications were also recorded and included sinusitis, hematoma, tension pneumocephalus, CSF leak, and reoperation. Postoperative endocrine status, visual outcome, length of stay (LOS), readmission, and quality of life (QOL) measures were collected. When available, the associations between frailty indices and each of these postoperative outcome variables were collected as well.
Results
A total of 4 studies were eligible for inclusion in this scoping review.19 -22 All studies examined frailty and postoperative outcomes after EESBS (Table 1).19 -22 The earliest study was published in 1953, and the most recent was published in 2023.19 -22 They represented a total of 1306 patients (682 female, 624 male) with an average age of 54.1 years.19 -22 Three articles were retrospective in nature (Khalafallah et al, Kshirsagar et al, and Sukys et al) and 1 article was a prospective observational study (Castle-Kirszbaum et al).19 -22 The sample size in each of the studies ranged from 88 to 680 patients.19 -22 In 3 studies (Khalafallah et al, Castle-Kirszbaum et al, and Sukys et al), the indication for surgery in all patients was for pituitary adenomas.19 -21 Kshirsagar et al, which had the smallest sample size of 88 patients, specifically examined patients undergoing EESBS for not only pituitary adenoma, but also meningioma, craniopharyngioma, chondrosarcoma, Rathke’s cleft cyst, and vascular malformation. 22 Table 1 summarizes this content within each article.
Articles Examining Postoperative Complications and Frailty Indices Following Endoscopic Endonasal Skull Base Surgery.
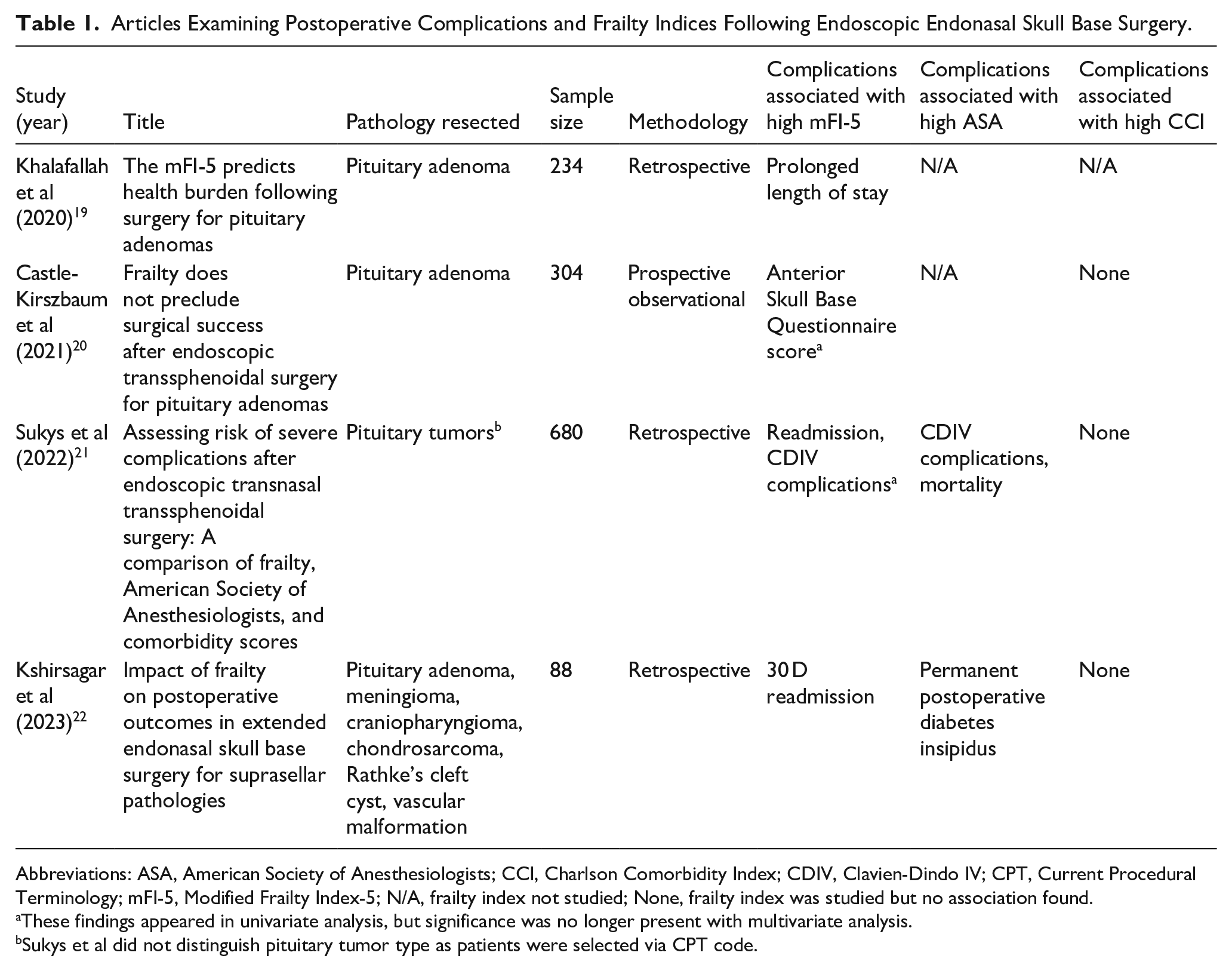
Abbreviations: ASA, American Society of Anesthesiologists; CCI, Charlson Comorbidity Index; CDIV, Clavien-Dindo IV; CPT, Current Procedural Terminology; mFI-5, Modified Frailty Index-5; N/A, frailty index not studied; None, frailty index was studied but no association found.
These findings appeared in univariate analysis, but significance was no longer present with multivariate analysis.
Sukys et al did not distinguish pituitary tumor type as patients were selected via CPT code.
Frailty Indices
Within the 4 studies in this review, validated scales that were used to quantify frailty included the Modified Frailty Index-5 (mFI-5), the Charlson Comorbidity Index (CCI), and the American Society of Anesthesiologists (ASA) classification (Table 1). The mFI-5 was the most widely used frailty index and was reported in all 4 studies in this review.19 -22 The CCI was the next most-widely-used frailty index and was additionally reported in 3 studies.20 -22 The ASA classification was used the least frequently as a frailty measure, with 2 studies reporting its use.21,22
Modified Frailty Index-5
Prior to performing statistical analyses, 3 studies converted mFI-5 into a categorical variable, and the specific ways in which the authors separated patients into categorical groups varied. Sukys et al categorized patients into 4 groups (mFI-5 score of 0, 1, 2, and 3+). 21 Castle-Kirszbaum et al dichotomized patients into 2 groups: mFI-5 ≤1 (non-frail) and mFI-5 >1 (frail). 20 Kshirsagar et al dichotomized patients into 2 groups as well but used different mFI-5 score cutoffs: mFI-5 = 0 (non-frail) or mFI-5 ≥1 (frail). 22 Khalafallah et al kept mFI-5 as a continuous variable when performing statistical analyses. 19
Charlson Comorbidity Index
Castle-Kirszbaum et al utilized CCI to define frailty by dichotomizing patients into 2 groups: CCI ≤1 (non-frail) or CCI >1 (frail). 20 Sukys et al categorized patients into 4 groups (CCI score of 0, 1, 2, and 3+). 21 Kshirsagar et al analyzed CCI as a frailty metric by keeping it a continuous numeric variable. 22
American Society of Anesthesiologists
Sukys et al analyzed ASA as a frailty marker and analyzed it as a categorical variable by dividing patients into 4 groups (ASA score of 1, 2, 3, and ≥4). 21 Kshirsagar et al analyzed ASA as a frailty metric by keeping it a continuous numeric variable. 22
Postoperative Outcomes
A wide range of postoperative complications were assessed in each article. The associations between frailty and outcome measures are described below and summarized in Tables 1 and 2.
Post-Operative Complications Associated With Increased Frailty Following Endoscopic Endonasal Skull Base Surgery.
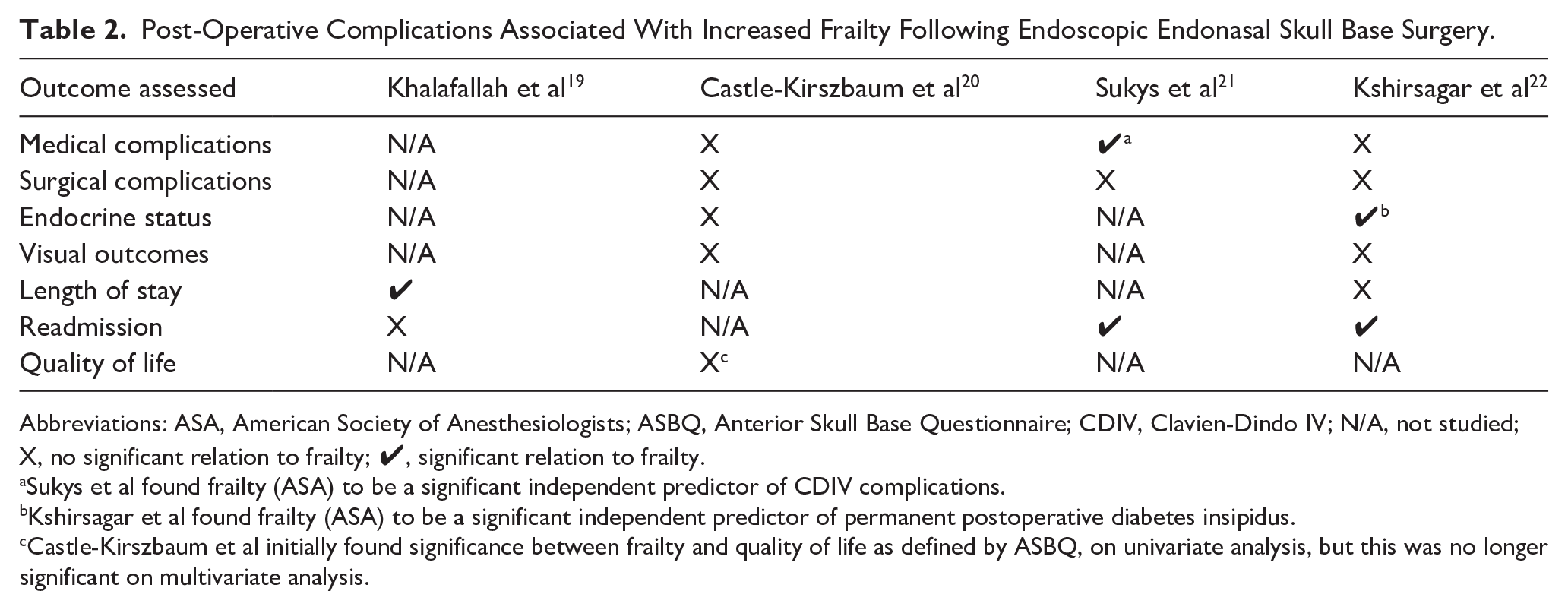
Abbreviations: ASA, American Society of Anesthesiologists; ASBQ, Anterior Skull Base Questionnaire; CDIV, Clavien-Dindo IV; N/A, not studied; X, no significant relation to frailty; ✔, significant relation to frailty.
Sukys et al found frailty (ASA) to be a significant independent predictor of CDIV complications.
Kshirsagar et al found frailty (ASA) to be a significant independent predictor of permanent postoperative diabetes insipidus.
Castle-Kirszbaum et al initially found significance between frailty and quality of life as defined by ASBQ, on univariate analysis, but this was no longer significant on multivariate analysis.
Medical Complications
Kshirsagar et al found no significant associations between postoperative medical complications (MI, CVA, pneumonia, PE, 30 day readmission, permanent DI, and vision loss) and frailty, as measured by mFI-5, CCI, and ASA. 22 Castle-Kirszbaum et al found no statistically-significant differences in medical complications (MI, hypoglycemia, cardiac arrest, vascular injury, seizure, VTE, meningitis, sepsis, stroke) between frail (mFI-5 >1) and non-frail (mFI-5 ≤1) patients. 20 Sukys et al found that mFI-5 was significantly correlated with ICU-level CDIV complications (cardiac arrest, MI, failure to wean off ventilatory >48 hours, renal failure requiring dialysis, sepsis with end organ failure, PE, unplanned reintubation) on univariate analysis (P = .01). 21 However, on their multivariable regression analysis, mFI-5 was not a significant predictor of CDIV complications. 21 CCI score was also not found to be associated with CDIV complications. 21 Sukys et al found that CDIV complications and mortality were significantly associated with frailty when defined by ASA score on their multivariable regression analysis (P < .01). 21 The same authors also found that mFI was not significantly correlated with non-CDIV medical complications (hyponatremia/hypoosmolality, DVT, pneumonia, UTI, and renal insufficiency not requiring dialysis). 21
Surgical Complications
Kshirsagar et al found no independent, significant associations between postoperative surgical complications (CSF leak, sinonasal wound infection, orbital injury, and blood loss requiring transfusion) and frailty as measured by mFI-5, CCI, and ASA. 22 Castle-Kirszbaum et al found no statistically-significant differences in surgical complications including sinusitis, hematoma, and tension pneumocephalus between frail (mFI-5 >1) and non-frail (mFI-5 ≤1) patients. 20 Sukys et al found that mFI was not significantly correlated with postoperative surgical complications including CSF leak, reoperation, superficial/deep wound infection, and hematoma on univariate analysis. 21 With the data available, Sukys et al found no significant correlation between CCI or ASA score and postoperative CSF leak and reoperation rate. 21
Endocrine Status
Kshirsagar et al found no significant relationships between higher mFI-5 or CCI and worsened endocrine status on multivariate analysis. 22 However, increasing ASA was significantly associated with permanent postoperative DI (P = .035). 22 Castle-Kirszbaum et al found that postoperatively, there were no significant differences in normalization of endocrinopathy in functioning tumors, rates of new adenohypophyseal deficiency, postoperative DI, and syndrome of inappropriate antidiuretic hormone secretion between frail (mFI-5 >1) and non-frail (mFI-5 ≤1) patients. 20
Visual Outcomes
Kshirsagar et al found no significant associations between mFI-5, CCI, and ASA and worsened postoperative vision status on multivariate analysis. 22 Castle-Kirszbaum et al examined patients who had preoperative field cuts and found that mFI-5 score was not a significant independent predictor of postoperative visual field outcomes on multivariate analysis, when age was considered. 20
Length of Stay
Kshirsagar et al found no significant relationships between higher mFI-5, CCI, and ASA and prolonged LOS (defined as ≥7 days) on multivariate analysis. 22 Khalafallah et al found that with each one-point increase in mFI-5, total LOS increased by 0.64 days among all patients (P < .001), 1.08 days in the Cushing disease cohort (P = .045), and 0.659 days in the nonfunctioning tumor cohort (P = .003), respectively. 19 The mFI-5 score was not significantly associated with total LOS for the acromegaly and prolactinoma functioning tumor subgroups. 19
Readmission
On multivariate logistic regression analysis, Kshirsagar et al found a significant association between higher mFI-5 and 30 day readmission (P = .038). 22 Khalafallah et al found that an increased mFI-5 score was not significantly associated with increased 90 day readmission in both the overall cohort and in the nonfunctioning tumor cohort. 19 Sukys et al found a significant correlation between mFI and readmission on univariate analysis (P = .04). 21
Quality of Life
Castle-Kirszbaum et al reported that QOL, as measured by the 35-item Anterior Skull Base Questionnaire (ASBQ) score, seemed to be lower in frail patients (mFI-5 >1) on univariate analysis. 20 However, on multivariate analysis, ASBQ score was actually strongly associated with the presence of Cushing’s disease, but not mFI-5 score. 20 Castle-Kirszbaum et al also utilized the 22-item Sinonasal Outcome Test (SNOT-22) as a sinonasal QOL tool, which was not found to be significantly associated with mFI-5 score. 20 When using the CCI to define frailty, Castle-Kirszbaum et al did not observe any differences in QOL between groups. 20
Discussion
We present the first review that consolidates all the current literature to date pertaining to frailty within EESBS, a topic that is still evolving and growing. Our results suggest that increasing frailty may be associated with greater postoperative CDIV complications, permanent DI, increased LOS, and readmission. In contrast, frailty does not seem to be associated with worsened postoperative surgical complications, endocrine dysfunction, visual outcomes, and QOL. This scoping review highlights major gaps in knowledge and the need for more research on this topic, to better predict which patients may be at higher risk for specific complications after endoscopic skull base surgery.
Within the existing neurosurgical literature, frailty has been significantly correlated with worse outcomes, including mortality, intracranial vascular complications, medical and surgical complications, LOS, readmission, and reoperation.12,16,17,19 Much of this existing literature has centered around open cranial surgeries and spinal procedures, as well as surgeries of the anterior cranial fossa such as pituitary surgery, without distinguishing between microscopic and endoscopic approaches.12,16,17,19,23 -37 In specifically EESBS, the cumulative findings from this review suggest that increased frailty may possibly be associated with certain postoperative outcomes such as ICU-level CDIV medical complications, postoperative permanent DI, prolonged LOS, and unplanned readmission. However, EESBS, in contrast to other approaches to the skull base such as microscopic and open cranial surgeries, may be safer and better tolerated even in patients traditionally described and defined as frail. This review found that among frailty (mFI-5, CCI, and/or ASA) and postoperative surgical complications (sinusitis, hematoma, tension pneumocephalus, CSF leak, and reoperation), vision status, and QOL (measured by either ASBQ or SNOT-22 score), there were no significant associations exhibited.20 -22 This may have been observed because in EESBS, there is no retraction on the brain compared with than in open approaches. There are also smaller incisions and bony defects to heal following EESBS than those that follow open approaches, which also leave external skin and soft tissue incisions to heal. There is also likely an inherent bias for larger tumors to be approached via an open craniotomy rather than a smaller endoscopic corridor. This bias, however, is not likely to be present between cases chosen for microscopic versus endoscopic techniques. When compared to microscopic pituitary surgery, EESBS allows better direct visualization, which may also help explain why multiple postoperative outcomes were not associated with frailty after EESBS in this review. Studies have shown that the endoscopic technique demonstrates significantly-shorter duration of surgery, minimized postoperative endocrine dysfunction, fewer overall complications, and improved normalization of visual impairment than the microscopic technique.12,13
This scoping review also highlights the fact that there is large variability in which frailty indices are included in studies. There is not yet a consensus on which frailty index is the most useful or valuable. Each index was developed with different but overlapping clinical definitions of frailty. 38 The mFI has multiple renditions, with the most recent being mFI-5. 39 The mFI-5 is a 5-point scale calculated based on the presence of multiple comorbidities, which has been identified as an equally-effective predictor of mortality and postoperative complications in geriatric populations across all subspecialties.39,40,41 The CCI consists of 19 items corresponding to various medical comorbidities. It was initially designed as a prognostic tool to predict 1 year mortality in hospitalized patients on the internal medicine service at Cornell Medical Center.42,43 Several adaptations of the CCI were developed and used in other contexts, including its use as a proxy for frailty.42,43 The ASA score classifies patient health on a scale of 1 through 6, with 1 indicating the patient is in good health and a level 6 indicating the patient is brain dead. 44 These classifications take several factors into account, including patient history and comorbidities. 44
Compared with CCI, mFI-5 and ASA are easier and simpler to calculate. CCI and mFI-5 are more objective than ASA, which may largely be determined based on a clinician’s interpretation of the patient’s health. 45 When comparing these 3 frailty indices, a study evaluating 41 369 patients from the NSQIP database found that mFI, CCI, and ASA all correlated significantly with outcomes; however, mFI-5 had the largest effect size. 46 A very similar conclusion was made in a study by Levy et al, who examined 23 104 patients undergoing prostate surgery. 47 mFI was found to better predict morbidity, and mFI and ASA were found to better predict mortality than CCI. 42 When comparing mFI and ASA only, there have been contradicting results with some studies concluding that mFI is a superior prognostic tool than ASA,48,49 while other studies have demonstrated ASA to be a better independent predictor of postoperative morbidity and mortality.50 -52 The results from our scoping review within EESBS demonstrate that mFI and ASA may be more useful in predicting postoperative outcomes than CCI. We hypothesize that CCI failed to predict outcomes in the studies included in this review perhaps because it was originally intended and designed to predict mortality in patients with medical admissions. CCI seems to be a good proxy for frailty in medical patients, but perhaps it may not be a good proxy for frailty and predicting outcomes in this specific postsurgical patient population. With EESBS being a relatively-recently-adopted approach to anterior cranial fossa pathology, and frailty becoming more widely researched as a prognosticator, a more standardized method of determining frailty in EESBS patients is necessary. We propose that future frailty studies consistently utilize and report at least mFI-5 score and ASA classification. In the clinical setting, frailty may be taken into consideration for patient risk stratification and preoperative patient counseling. For example, surgeons may assess a patient’s mFI-5 and ASA scores then discuss the possibility of elevated patient-specific risks such as ICU-level CDIV complications, permanent postoperative DI, increased LOS, and unplanned readmission, allowing for improved shared decision-making between patients and their care team.
This scoping review also underscores the need for future studies to utilize more consistent definitions, analysis, and interpretation of frailty scores. We hypothesize that perhaps some of the variability seen in the results relating to positive associations between frailty and postoperative outcomes may partially be due to the fact that each study defined and categorized frailty differently. Although all studies reported mFI-5, 3 studies converted mFI-5 into a categorical variable, and the specific ways in which the authors binned patients into categorical groups varied.20 -22 Sukys et al categorized patients into 4 groups (mFI-5 score of 0, 1, 2, and 3+). 21 Castle-Kirszbaum et al dichotomized patients into 2 groups: mFI-5 ≤1 (non-frail) and mFI-5 >1 (frail). 20 Kshirsagar et al dichotomized patients into 2 groups as well but used different mFI-5 score cutoffs: mFI-5 = 0 (non-frail) or mFI-5 ≥1 (frail). 22 Khalafallah et al kept mFI-5 as a continuous variable when performing statistical analyses. 19
In the literature of other surgical fields, large-scale studies have also demonstrated this inconsistency.30 -37,39,53 -56 There is drastic variation in authors’ analyses of frailty data, with some keeping frailty score as a continuous variable and running multivariate regression analyses,54,55 whereas others stratify patients into cohorts based on frailty scores.39,56 There is further variation in the number of groups patients are stratified into, as well as the score that is used to define each group. For example, in the neurosurgical literature, Weaver et al examined 23 516 patients who underwent posterior lumbar fusion and categorized patients in 3 groups: (1) mFI-5 = 0; (2) mFI-5 = 1; and (3) mFI-5 ≥2. 39 In the trauma surgery literature, Tracy et al categorized patients into 3 groups as well, but with different scores defining each group: (1) mFI-5 = 0 (not frail); (2) mFI-5 = 2 (moderate frailty); and (3) mFI-5 ≥4 (severe frailty). 56 Rather than arbitrarily grouping patients based on frailty score, we propose that future studies treat frailty score as a continuous variable and perform multivariate logistic regression analyses to determine the independent predictive value of frailty on various complications. This method is exemplified by Traven et al who analyzed mFI-5 score as an independent predictor of complications among 226 398 patients who underwent total knee arthroplasty. 55 In this way, it may be more statistically robust to keep frailty score as a continuous variable, given that it is numerical in nature. Continuous variables offer a more precise and detailed representation of data and often result in greater statistical power to detect effects, because they capture variation that is otherwise lost when data are consolidated into categories. Continuous variables allow for a wider range of statistical analyses, including parametric tests, whereas categorical variables are often analyzed using nonparametric tests, which are generally less statistically powerful. In addition, continuous variables can model trends, slopes, or nonlinear relationships in a way that categorical ones cannot support.
There are many limitations to this scoping review. Inherently, the focus of this review is to provide breadth rather than the depth of information on a very focused topic. Our review included a smaller number of studies, each with smaller sample sizes. A meta-analysis is generally unable to be performed in a scoping review as well, diminishing the strength and generalizability of any conclusions made in this review. We acknowledge that our research question is quite narrow, which is itself a limitation of this review, as this led to yielding only 4 studies. However, we believe this is an importantly-narrow question because EESBS is a very different surgery with different known outcomes than microscopic skull base surgery as well as open cranial surgeries. Despite the narrow question and limitations, we feel this scoping review is important as it highlights a need for future study, and we discuss suggestions on how to conduct future studies systematically, particularly in which frailty indices to report and the methods of statistical analyses to perform.
Strengths of the project include the standardized article selection with 2 independent researchers to eliminate bias. Additionally, the inclusion of all related articles from any year over multiple databases allowed for a comprehensive search, minimizing the risk for unintentionally-excluded research.
Conclusion
This scoping review suggests that increasing frailty may confer higher morbidity following EESBS, such as CDIV complications, permanent DI, increased LOS, and readmission. However, in contrast to other skull base approaches such as open and microscopic techniques, EESBS may be better tolerated even in frail patients, as frailty was not found to be significantly associated with worsened postoperative surgical complications, endocrine dysfunction, visual outcomes, and QOL. Further research on this topic is necessary, and we propose utilizing the mFI-5 and ASA indices in future studies. Frailty scores should be treated as continuous rather than categorical variables for the most consistent and robust statistical analyses. Understanding frailty and perioperative risk factors in EESBS will facilitate stronger patient-centered discussions, education, and informed consent.
Footnotes
Author Note
This paper was presented at the 2024 American Rhinologic Society Combined Otolaryngology Spring Meeting, Chicago, IL, on May 15 to 19, 2024.
Author Contributions
Ashleigh Halderman: investigation, review, and editing. Bradley F. Marple: investigation, review, and editing. Sofia E. Olsson: conceptualization, data curation, formal analysis, investigation, methodology, resources, writing of original draft, review, and editing. Matthew W. Ryan: investigation, review, and editing. Sei Y. Chung: conceptualization, data curation, formal analysis, investigation, methodology, resources, supervision, writing of original draft, review, and editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data are available upon request from the corresponding author.