
Abstract
Mucormycosis of temporal bone is extremely rare. They are usually associated with host immunodeficiency, are difficult to diagnose, and many cases are fatal. We performed a literature review and found only 10 reported cases of temporal bone mucormycosis. We present a case of temporal bone mucormycosis involving the temporomandibular joint and infratemporal fossa in a 53-year-old woman with diabetes mellitus who presented with unbearable otalgia. Computed tomography and magnetic resonance imaging demonstrate inhomogeneous density mass in the parapharyngeal and retropharyngeal space accompanied with lytic bone destruction on the temporomandibular joint. After undergoing a biopsy of the left infratemporal fossa, the patient’s pathology exhibited fungal hyphae consistent with mucormycosis. To our knowledge, this is the first report of temporal bone mucormycosis with extensive involvement of temporomandibular joint and its adjacent structures, which exhibited no otologic or rhinologic signs. A definitive diagnosis is made by biopsy.
Introduction
Mucormycosis of temporal bone is extremely rare, but the prevalence has been rising due to the increase in the rate of diabetes and immunosuppressive conditions. The organism causing mucormycosis is the saprophytic fungi of the Zygomycetes class and the Mucorales order. 1 It has been ubiquitous and found in soil samples, bread molds, and other geographic areas. 1 It poses no threat to normal hosts but usually occurs in immunocompromised patients with diabetes, HIV, neutropenia, malnutrition, hematologic malignancies, and so on. 2 It usually can be introduced by respiratory tract or cutaneous and dental lesions after trauma. 3
Mucormycosis of temporal bone is often a rapidly fatal infection. The pathological feature of mucormycosis is the invasion of a blood vessel, resulting in hemorrhage, thrombosis, infarction, and necrosis of tissue. 4 The representative physical finding is a notorious black eschar plaque due to the centrifugally disseminating necrosis. 5 The clinical features of temporal bone involvement include otalgia, facial pain, headache, and facial paralysis. Mucormycosis of temporal bone has been sparsely reported in the otologic literature. A review of the literature showed only 10 cases of temporal bone mucormycosis has been reported. 4,6 -14 But extensive involvement of the temporomandibular joint and infratemporal fossa with this fungus is uncommon. In this study, we describe a case of mucormycosis of temporal bone involving the temporomandibular joint and infratemporal fossa, which may be the first case report till now. Accurate diagnosis and appropriate treatment are extremely important for the patients’ prognosis.
Case Report
A 53-year-old Chinese woman with End stage renal disease secondary to diabetic nephropathy sought treatment after experiencing left otalgia for 2 months. Her medical history was significant for bilateral chronic otitis media for 40 years and insulin-dependent diabetes mellitus for 20 years, hypertension, and heart disease. She complained of an aural discharge and otalgia. The oto-microscopic examination demonstrated edematous ear canal skin with purulent drainage. There was a central tympanic membrane perforation with thickened middle ear mucosa. Tuning fork tests show a left conductive hearing loss. A diagnosis suggestive of the acute attack of otitis media was made, and she began a course of oral ciprofloxacin and ciprofloxacin eardrops for 2 weeks.
Two weeks later, the symptom of aural discharge was disappeared, but her ear pain was persisted. On examination, there was no clinical evidence of a postauricular abscess. The oto-microscopic examination demonstrated edematous ear canal skin without purulent drainage. Her left tympanic membrane was perforated without evidence of effusion. She was discharged to home on a 2-month regimen of antibiotic therapy and pain control. She was followed as an outpatient on a regular basis, and her pain improved dramatically.
After 2 months of outpatient therapy, she sought treatment for worsening pain radiating behind her ear associated with left painful occlusion. She visited our hospital and underwent magnetic resonance imaging (MRI) and computed tomography (CT) serially. T1-weighted MR images showing isointense signals opacity with extension into the temporomandibular join and infratemporal fossa (Figure 1A). T2-weighted MR images revealed moderate and slightly high signal opacity of external canal that extended into the temporomandibular joint, infratemporal fossa, parapharyngeal space, and retropharyngeal space (Figure 1B). Computed tomography showed opacity of the left temporomandibular joint that extended into the nasopharynx, parapharyngeal space, and retropharyngeal space with erosion of the temporomandibular joint (Figure 2).
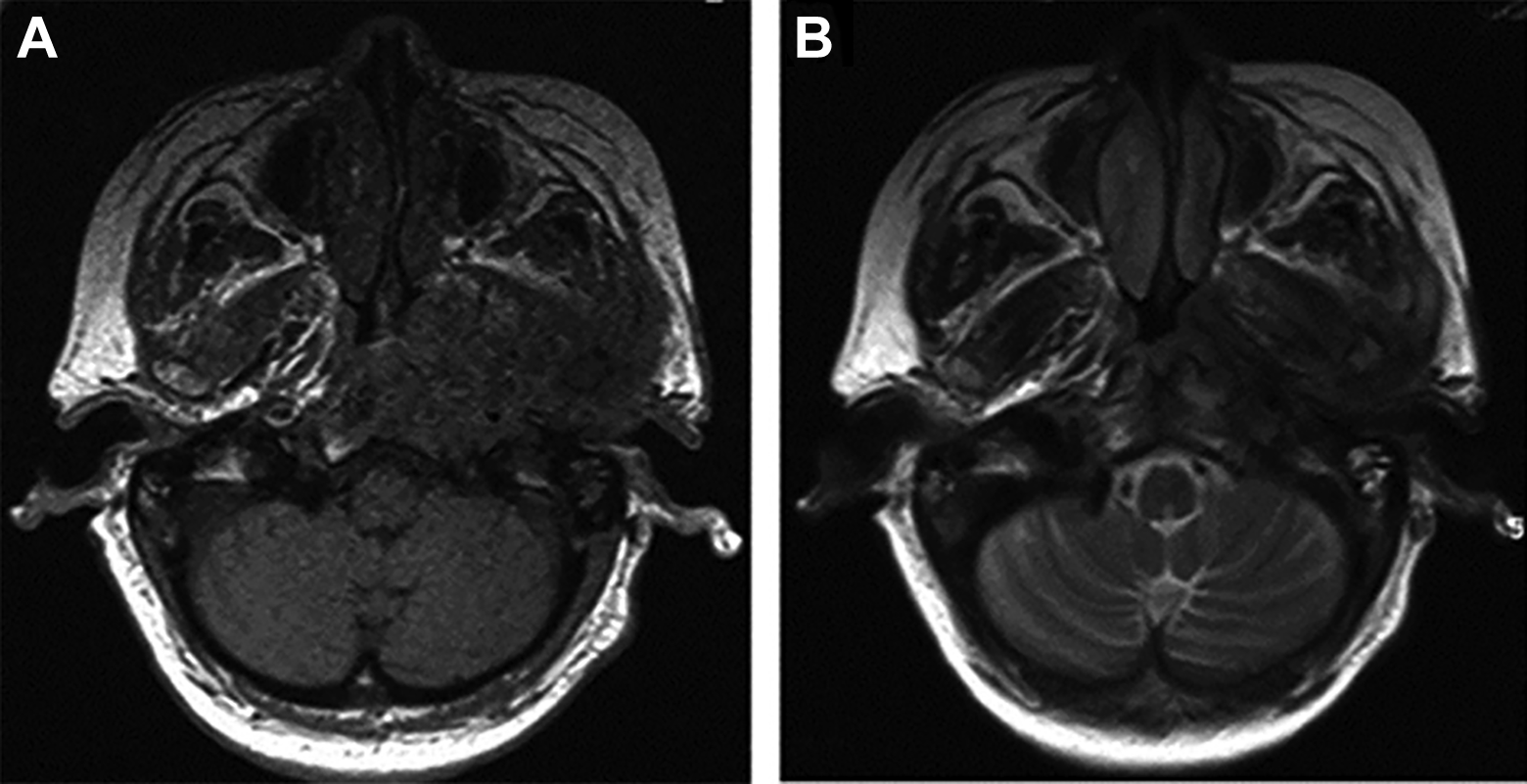
A, T1-weighted magnetic resonance (MR) image showing isointense signals opacity with extension into the temporomandibular join and infratemporal fossa. B, T2-weighted MR image showing moderate and slightly high signal opacity of external canal that extended into the temporomandibular joint infratemporal fossa parapharyngeal space and retropharyngeal space.
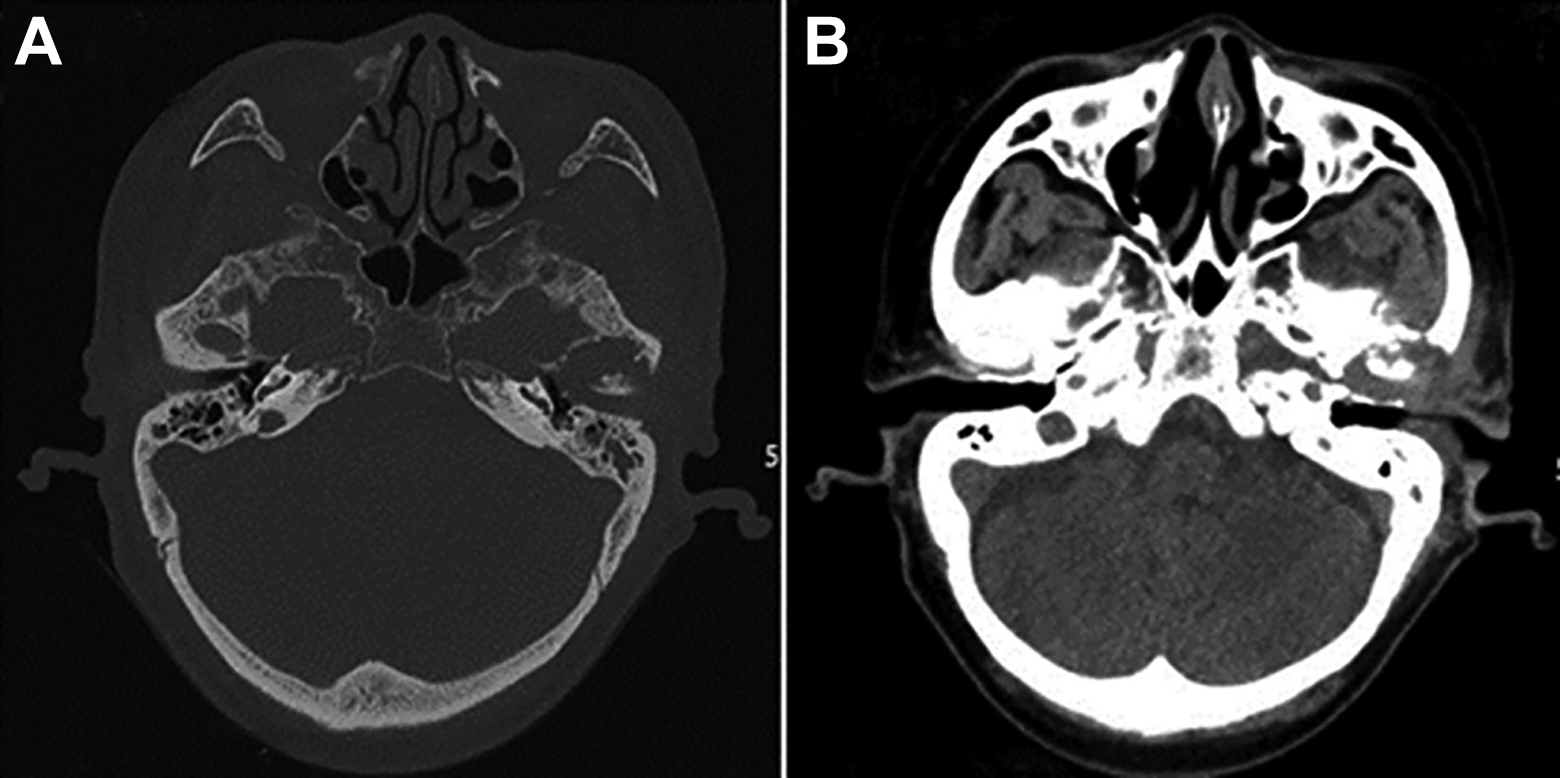
A and B, Horizontal computed tomography (CT) scans showing bony destruction of temporomandibular and extending into the infratemporal fossa.
Because of the long-standing history of right chronic otitis media and the possibility of malignancy, she was taken to surgery and a biopsy of the left infratemporal fossa was performed under local anesthesia. Histological analysis of the infratemporal fossa biopsy confirmed tissue invasion by Mucor with the formation of granuloma and fibrosis (Figure 3A and B). The hyphae exhibited deep tissue penetration, perivascular invasion, and right-angle branching of septae, which is in keeping with Mucor species (Figure 3C and D). The patient was treated with oral posaconazole (600 mg/d) for 3 weeks. Three weeks later, the patient was pain free.
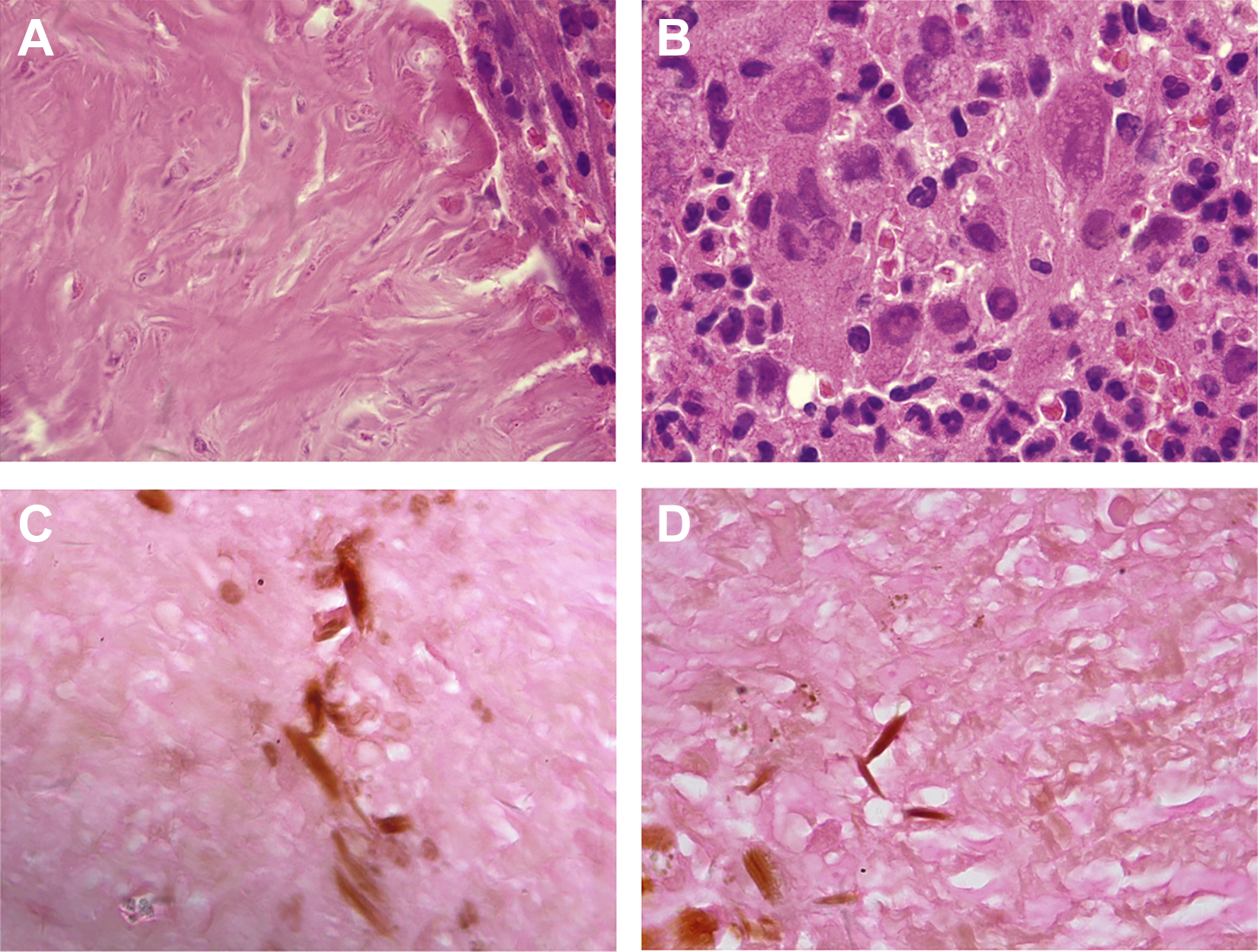
A, Fibrosis demonstrated by hematoxylin and eosin (H&E) staining (×1000). B, Granuloma and giant cells as identified by H&E staining (×1000). C, Gomori methenamine silver staining showing fungal hyphae (arrows; ×1000). D, Nonseptate hyphae with right angle branching hyphae consistent with mucormycosis (arrows), as identified by Gomori methenamine silver staining (×1000).
Discussion
Till now, only 10 cases of mucormycosis of the temporal bone have been reported in the literature. 4,6 -14 But extensive involvement of temporomandibular joint, infratemporal fossa, parapharyngeal space, and retropharyngeal space with bone erosion which exhibited no otologic or rhinologic signs as described in our patient may be the first case report till now.
The physical findings of temporal bone mucormycosis were similar to those seen in cases of infection caused by Pseudomonas aeruginosa so that it is often misdiagnosed as malignant otitis externa. Malignant otitis externa is almost always seen in the immunocompromised patient. 15 It is often aggressive and can spread through vascular and soft tissue planes into the neighboring skull base. 15 Necrotizing otitis externa and temporal bone mucormycosis have similar clinical characteristics and relevant factors, but the therapy and prognosis of the 2 diseases are different, so it is important to distinguish these 2 diseases. However, early and definitive diagnosis of mucormycosis is made by biopsy. Methanamine-silver nitrate stain allows excellent histologic visualization of the characteristic broad, nonseptate hyphae with right angle branching.
The classification of fungi infection for paranasal sinus disease was applied to temporal bone infections by Hall and Farrior. 16 The fungal infection of temporal bone was classified into 3 types: noninvasive, acute invasive (fulminant), and chronic invasive. In our case, the patient complained of otalgia for 4 months and left painful occlusion that had persisted for 2 months. The histopathologic examination revealed noncaseating granuloma with Langhans-type giant cells, vascular proliferation, and perivascular fibrosis (Figure 3). Hence, chronic invasive fungal infection was diagnosed because these findings were consistent with its diagnostic criteria.
Computed tomography and MRI imaging reveal bone destruction and soft tissue filling defects. These imaging findings are analogous to those of malignant lesions including bony destruction and extension beyond the temporal bone. Therefore, surgical biopsies may be necessary to arrive at a correct diagnosis.
Conclusion
This case highlights the need to include temporal bone mucormycosis in the immunocompromised host who presents with intractable otalgia and painful occlusion. Computed tomography and MRI are useful diagnostic aids for detecting lesions in or beyond the temporal bone. Surgical biopsies may be necessary to arrive at a correct diagnosis and to direct effective therapy. Thorough diagnostic evaluation and aggressive therapeutic intervention can lead to decreased morbidity and increased survival.
Footnotes
Author’s Note
Zhangcai Chi contributed to manuscript writing and data collection; Chen Zhang contributed to data collection and proofreading of the manuscript; Wuqing Wang contributed to study design and responsibility for the integrity of the content of the paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.