
Abstract
Dermoid cysts are benign cutaneous neoplasms that contain germ cells from the ectoderm and mesoderm. Approximately 70% are diagnosed during childhood before the age of 5. Although they can present throughout the body, the prevalence is 7% for those arising from the head and neck. These lesions present primarily as midline masses and are classified as sublingual, submental, or overlapping depending on their relationship with the muscles of the floor of mouth. A 10-year-old female presented with a 2-week history of right submental swelling. She denied pain, dysphagia, odynophagia, or respiratory distress. Physical examination showed nontender fullness of the submental region without erythema or induration and no palpable cervical lymphadenopathy. Ultrasound showed an oval-shaped cystic mass measuring 4.8 × 4.0 × 2.6 cm. After a course of clindamycin, a computed tomography was obtained which showed a right 4.5 × 4.0 × 2.6 cm fluid filled lesion, within the right lateral floor of mouth. Intraoral resection was performed and the mass was freed from the geniohyoid and mylohyoid. Histopathology was consistent with a dermoid cyst. Submental masses have a broad differential, but rarely are they dermoid cysts if they arise lateral to the midline. With appropriate diagnosis and total surgical excision, patients and their families can be reassured in similar cases.
Introduction
Dermoid cysts are benign cutaneous neoplasms that contain germ cells from the ectoderm and mesoderm. 1 Approximately 70% are diagnosed during childhood before the age of 5. 2 Although they can present throughout the body, the prevalence is 7% for those arising from the head and neck. Typically, they occur at embryologic fusion lines, including the lateral third of the eyebrow, midline neck, or nasolabial fold. 3,4 In this case, we present a rare presentation of a pediatric dermoid cyst.
Case Report
A 10-year-old female presented to the pediatric otolaryngology clinic with 2-week history of painless right submental swelling without dysphagia, odynophagia, or respiratory distress. Physical examination showed nontender fullness of the submental region with no evidence of erythema or induration. There was no palpable cervical lymphadenopathy. The neck ultrasound showed a well-circumscribed oval-shaped midline cystic mass measuring 4.8 × 4.0 × 2.6 cm. The patient was initially given oral clindamycin for 10 days without change in symptoms, therefore further imaging was obtained. A contrast-enhanced computed tomography (CT) revealed a 4.5 × 4.0 × 2.6 cm fluid filled lesion within the right lateral floor of mouth (Figure 1). With these findings, our differential diagnosis included a plunging ranula, lipoma, dermoid cyst, branchial cleft cyst, or thyroglossal duct cyst.

Coronal CT with contrast showing a fluid filled mass within the right lateral floor of mouth. CT indicates computed tomography. Photo credit: Department of Radiology, University Hospitals Cleveland Medical Center.
Surgical treatment was recommended, and given the location of the lesion, an intraoral approach was planned. Bimanual examination under anesthesia revealed a mobile mass within the floor of mouth that appeared to be separate from the submandibular gland. The submandibular papilla was cannulated with a 00 lacrimal probe to help with identification of the duct during the procedure. An incision was made along the right floor of mouth and blunt dissection was performed until the mass was identified. Once visualized, the mass appeared to have a thick capsule and did not appear consistent with a ranula. The mass was then dissected free from the submandibular duct. Additionally, during dissection, the lingual nerve was identified adjacent to the mass and preserved. Further, the sublingual gland was located sitting superficial to the mass and was therefore excised to allow for better visualization. Lastly, the mass was freed from the geniohyoid and mylohyoid musculature and successfully removed in its entirety (Figures 2 and 3). The tissue was sent for permanent histopathologic analysis, which showed a unilocular cystic lesion containing pasty, white material consistent with keratin (Figure 4).
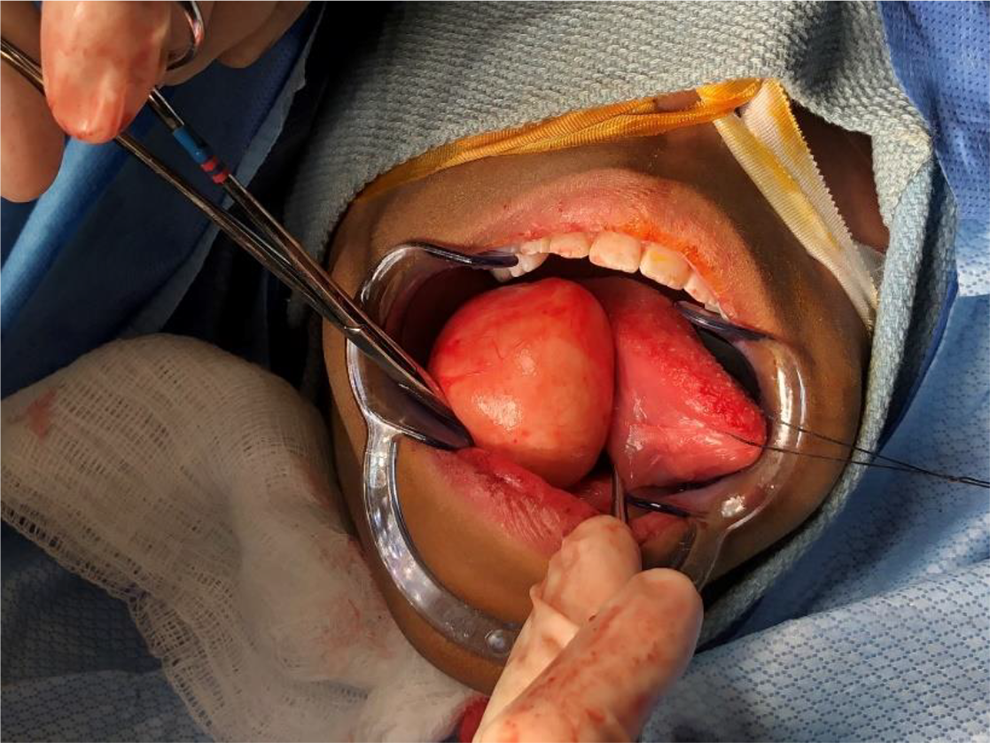
Intraoperative photograph showing the dermoid cyst being delivered through a right lateral intraoral incision. Photo credit: Department of Otolaryngology–Head and Neck Surgery, University Hospitals Cleveland Medical Center.

Intraoperative photograph of the floor of mouth mass following complete surgical excision. Note the thick capsule, which is typical for a dermoid cyst. Photo credit: Department of Otolaryngology–Head and Neck Surgery, University Hospitals Cleveland Medical Center.
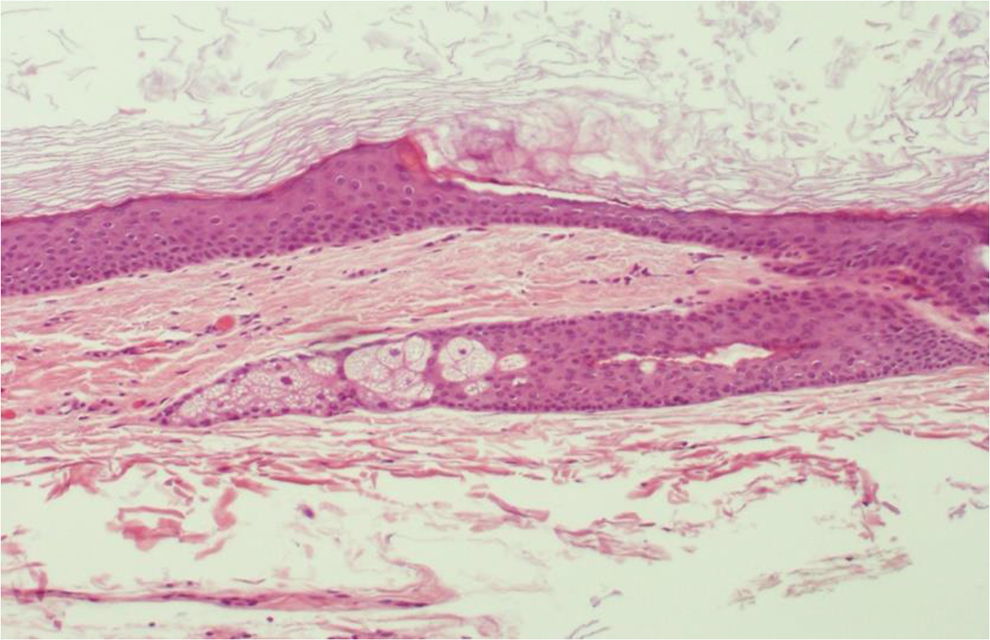
Histopathologic analysis of the mass. Note the stratified squamous epithelium and intracapsular contents consistent with keratin. Photo credit: Department of Pathology, University Hospitals Cleveland Medical Center.
Discussion
Dermoid cysts are slow-growing, benign tumors believed to be the result from both congenital and acquired manners. 5 Although the etiology of these cysts is still uncertain, there are 2 main theories of their origin. The most widely accepted theory proposes a congenital origin, in which a midline entrapment of ectodermic tissue occurs because of a defective fusion of the mandibular and hyoid branchial arches during the third and fourth weeks of development. 6,7 The second theory suggests that dermoid cysts can be acquired as the result of trauma or implantation of epithelial cells in utero. 8,9
Typically, dermoid cysts present as a nontender palpable firm mass. Within the head and neck, the most common presentation is midline, such as in the nose or neck. Conversely, presentation in the submental region is extremely rare, with an overall incidence of 1.6%. 5 Although the majority of patients, including ours, are asymptomatic, dermoid cysts can be associated with dyspnea, dysphagia, or dysphonia, and may necessitate urgent surgical treatment. 10,11
As demonstrated in our case, unusual presentations of neck masses may pose a challenge during the differential diagnosis because of the clinical similarities with other head and neck masses. For instance, a ranula is a pseudocyst formed due to the extravasation of mucus after trauma to the sublingual gland. This type of lesion typically presents on the floor of the mouth and is classically unilateral, while a dermoid cyst is usually midline and symmetrical. 10 Furthermore, thyroglossal duct cysts are also congenital neck lesions. However, these are the remnant of the descending thyroglossal duct, and rarely can occur in the floor of the mouth. 12
Diagnostic approach to dermoid cysts includes fine needle aspiration, ultrasound, CT, or magnetic resonance imaging (MRI). Ultrasound most commonly shows a heterogeneous mass with both solid and cystic features. A CT scan exhibits a thin walled, unilocular, fluid filled mass, and on MRI, dermoid cysts can vary in intensity on T1-weighted images; however, they appear hyperintense on T2-weighted images. Histopathology of these lesions show a cystic capsule lined with stratified squamous epithelium, comprised of dense fibrous connective tissue and cystic contents with an abundance of keratin.
The treatment of choice is complete surgical excision via either intraoral or extraoral approach depending on the location of the lesion compared to the mylohyoid muscle. 13 Some cysts require aspiration of contents in order to be removed completely to avoid rupture.
Given that the majority of dermoid cysts arise outside of the submental region, we found this case to be particularly interesting. It is even more peculiar in that this mass arose away from the midline, which is not commonly described. With appropriate diagnosis and total surgical excision, patients and their families can be reassured in similar cases.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.