
Abstract
Objective:
Current studies still find insufficient evidence to support the routine use of repetitive transcranial magnetic stimulation (rTMS) in tinnitus. This study aimed to assess response of tinnitus to treatment with rTMS and identify factors influencing the overall response.
Methods:
Between January 2016 and May 2017, 199 tinnitus patients were identified from a retrospective review of the electronic patient record at the Sun Yat-sen Memorial Hospital. All patients received rTMS treatment. Their clinicodemographic profile and outcomes, including the tinnitus handicap inventory (THI) and visual analog scale (VAS) scores, were extracted for analysis.
Results:
Regarding the THI results, 62.3% of all patients responded to rTMS. The analysis of the VAS score revealed an overall response rate of 66.3%. Both percentages were close to the patient’s subjective assessment result, of 63.8%. Patients with tinnitus of less than 1-week duration had the highest response rate to rTMS in terms of either THI/VAS scores or the patient’s subjective assessment of symptoms. Tinnitus duration was recognized as a factor influencing the overall response to the treatment.
Conclusions:
Repetitive transcranial magnetic stimulation treatment is effective for patients with tinnitus, but its efficacy is affected by tinnitus duration. Tinnitus patients are advised to attend for rTMS as soon as possible since therapy was more effective in those with a shorter duration of disease of less than 1 week.
Introduction
Tinnitus is a common auditory symptom characterized by persistent sensations of sound inside the ear or head in the absence of an external sound source or electromagnetic stimulation. 1,2 Approximately 10% to 15% of the world population has suffered from tinnitus, 10% of which may be afflicted by life-threatening effects of severe symptoms. 3 But preexisting studies fail to provide a reliable and accurate evidence-based medication management for tinnitus. 1
Animal experiments and functional imaging of the human brain show that abnormal patterns of auditory hair cell differentiation induce hypersynchrony and hyperactivity in the central auditory pathways and the latter results in more connections to nonauditory brain regions. These connections are recognized as the neuronal correlates of tinnitus. 4 -6 Repetitive transcranial magnetic stimulation (rTMS) is a noninvasive neuromodulation technique based on electromagnetic induction. Its application to the brain has been found to produce electrical currents intracranially after a train of repetitive pulses, modulating the excitability of the neurons and cortical activity. 7,8 Some studies ascertained that rTMS at low frequency (≤1 Hz) effectively altered neural activity and considered it a promising therapeutic modality for tinnitus. 9,10 Other trials found the relief of tinnitus symptoms after rTMS treatment in the left temporal cortex. 11,12 But the controversy of its efficacy continues as 2 latest class I clinical studies yielded an insignificant difference in the overall response between the active and placebo groups. 13,14 More in-depth studies are needed to provide answers to methodological and practical problems associated with rTMS application for tinnitus. Liang et al conducted a systematic review of rTMS studies for tinnitus published through April 2020, but the 29 randomized trials eligible for analysis only represented 1228 patients. 15 More clinical data are requested for a reliable analysis.
Therefore, we performed the current retrospective analysis of tinnitus patients undergoing rTMS, aiming to provide more reliable evidence for the efficacy of rTMS and identify factors influencing treatment response. We hope that this study will add to the evidence associated with the treatment of tinnitus.
Materials and Methods
Patients
We reviewed medical records of tinnitus patients seen at the Sun Yat-sen Memorial Hospital from January 2016 to May 2017. They were previously untreated, or drug therapy had been discontinued for at least 3 months due to unsatisfactory drug response. Patients with neurological diseases or organic diseases of the middle or inner ear, including those with eustachian tube dysfunction having started in the meantime, were excluded. Those fulfilling the above-mentioned criteria were only treated with rTMS and did not receive any other treatment to support auditory function. All patients gave written informed consent. The protocol was approved by the ethics committee of the Sun Yat-sen Memorial Hospital. Before starting an rTMS session, all patients must undergo complete otological and audiological examinations, such as otoscopy, tympanometry, pure-tone audiometry, and tinnitus matching. Data were extracted from the electronic patient record system at our hospital. Clinical characteristics of tinnitus consisted of tinnitus duration and position, hearing type, hearing loss, and the masking effect assessed using pure-tone audiometry at baseline. The tinnitus handicap inventory (THI) and tinnitus visual analog scale (VAS) that were frequently used to document the efficacy of therapies for tinnitus were employed. 16,17 In the 25-item THI, there was only 1 answer selected from 3 options for each question: yes (4 points), sometimes (2 points), and no (0 points). Within a maximum of 100 points, a higher score denoted a greater tinnitus-related handicap.
Treatment
In rTMS, a magnetic coil was positioned against the scalp while a train of repetitive pulses was being delivered to the left temporal cortex and the left prefrontal cortex. Both regions were recognized as better treatment options available for tinnitus based on magnetic resonance imaging. 18,19 Each patient underwent 10 sessions (2000 stimuli per session) of 1-Hz rTMS. We performed 5 times per week from Monday to Friday and a total of 10 times in a 2-week course of treatment. At the 3-month follow-up, the severity of tinnitus was assessed using the THI and VAS, and the subjective evaluation of the efficacy was described. A THI score reduction of more than 6 points from the baseline result was considered effective. 19 In turn, a THI score reduction of < 6 points just informed therapeutic failure, and a decline in VAS scores of ≥1 point indicated a valid treatment.
Data Analysis
SPSS 23.0 statistical software was used for analysis. Data were expressed as mean ± SD, and correlations were assessed using the χ2 test. A P value < .05 was considered statistically significant.
Results
Finally, 199 tinnitus patients were eligible for analysis, incorporating 88 (44.2%) males and 111 (55.8%) females. The youngest was 12 years of age and the oldest 86, with an average of 46.4 ± 15.0 years of age.
Using a cutoff of 6 for discriminating the THI difference before and after the treatment, 62.3% of patients included responded to rTMS. They were subsequently stratified by tinnitus duration. Those of less than 1-week duration revealed a higher response rate, of 82.8% (χ2 = 7.843, P = .048), versus other subgroups whose response rates were 57.6%, 53.5%, and 67.2% for patients of 1-week to 1-month, 1-month to 1-year, and over 1-year duration. Subgroup comparisons by sex, age, tinnitus position, hearing type, hearing level, and the masking effect did not demonstrate significant results (all P > .05), as shown in Table 1.
The Impact of Various Factors on THI Difference.
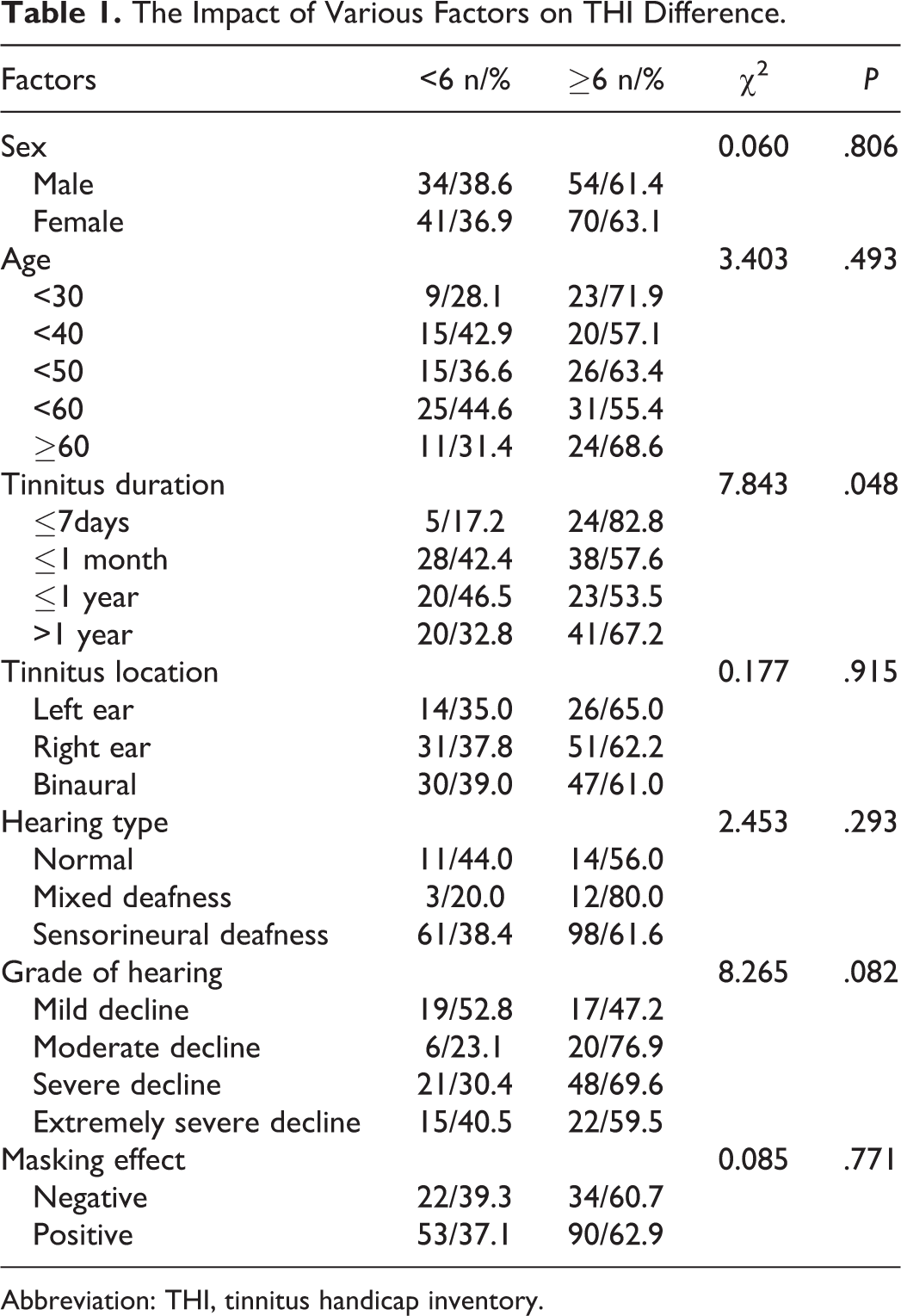
Abbreviation: THI, tinnitus handicap inventory.
With the VAS cutoff of 1, the overall response to rTMS was 66.3%. Subgroup comparisons by tinnitus duration and hearing level revealed significant effects on rTMS response (both P < .05). Specifically, the analysis by tinnitus duration revealed the strongest response in the ≤ 1-week subgroup (χ2 = 8.701, P = .034) versus the response rates of 60.6%, 55.8%, and 70.5% for patients of 1-week to 1-month, 1-month to 1-year, and > 1-year duration, respectively. Hearing level had a significant impact on VAS results (χ2 = 10.711, P = .030), with the response rates as follows: 61.3% for normal-hearing listeners and 47.2%, 84.6%, 69.6%, and 70.3% for patients with mild, mild-moderate, moderate-severe, and severe hearing loss. Other factors did not show significant effects on VAS results (P > .05; Table 2).
The Impact of Various Factors on VAS Difference.
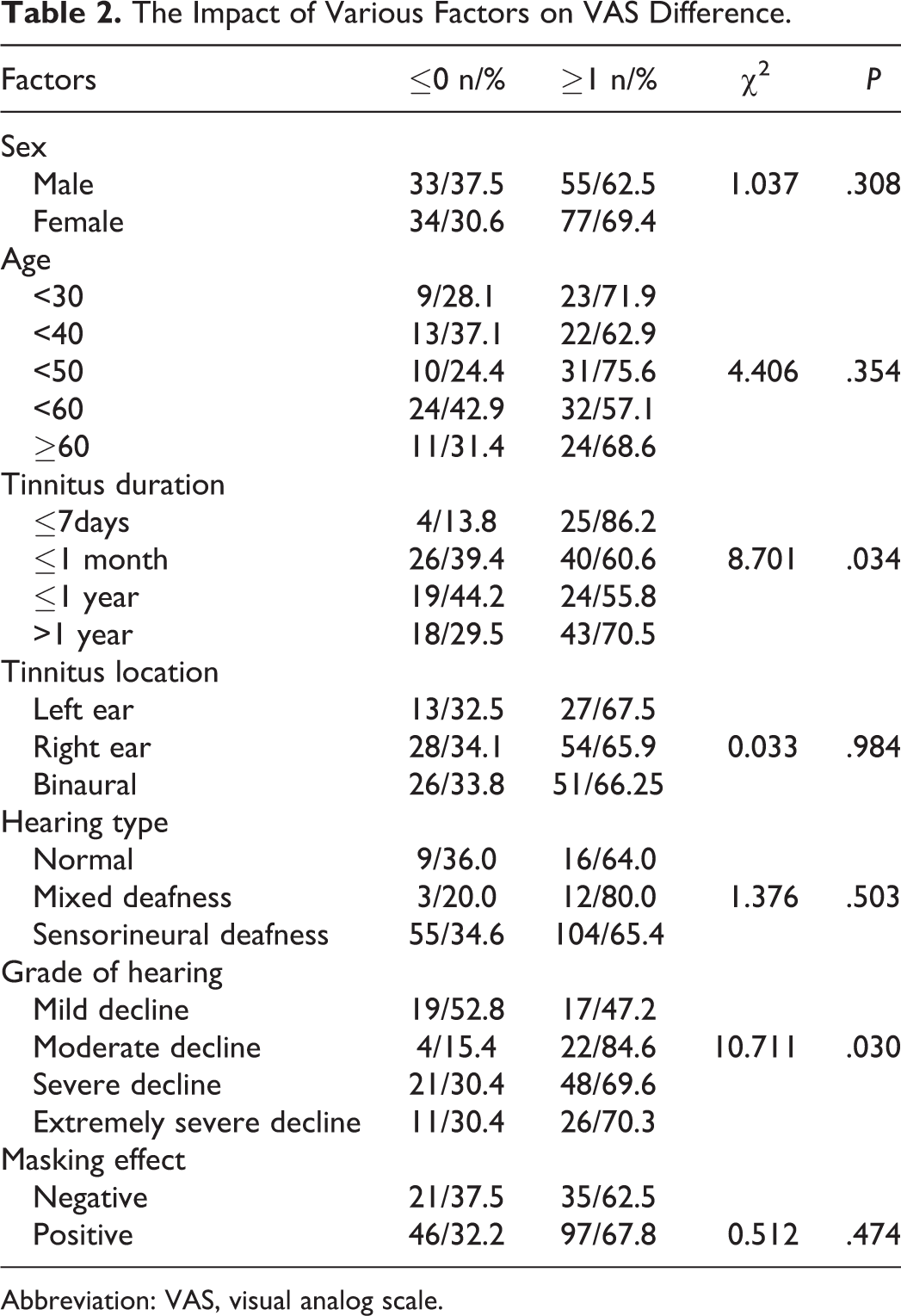
Abbreviation: VAS, visual analog scale.
The patient’s subjective assessment of symptoms was performed; 19.6% of them were apparently improved, 44.2% were improved, and 18.1% of patients reported slight and no improvements, respectively. Therefore, the overall response in terms of the patient’s perception of improvement was 63.8%, as shown in Figure 1. The multivariate regression analysis did not identify any factor markedly influencing the overall response.
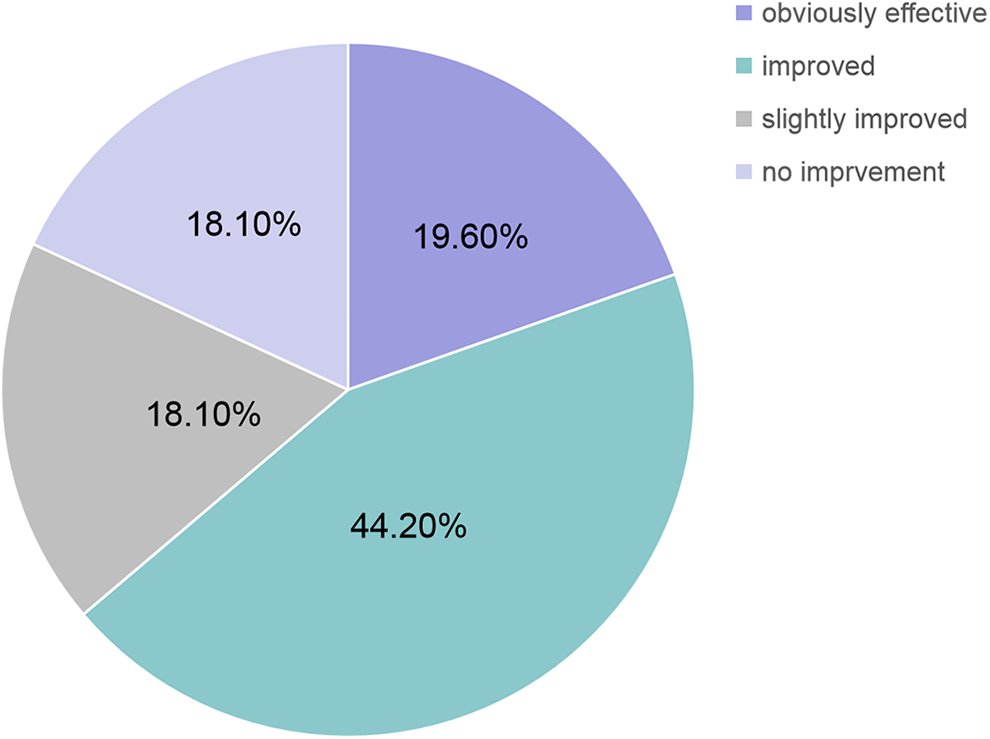
Subjective efficacy evaluation of patients.
Discussion
The incidence of tinnitus is high and differs across populations. Given a high frequency of hearing loss in tinnitus, peripheral auditory system components are most certain to be considered a contributor to the pathogenesis. While some studies regard damage of the peripheral auditory system structure damage as the only cause, others attribute the onset and persistence of tinnitus to hyperactivity or reorganization of cortical and subcortical structures as an increase in spontaneous activity and more neurons in the auditory pathways have been observed. Other possible mechanisms consist of enhanced synchronous electrical activity and recombination of the neural network between auditory pathways and the limbic system. Since the first introduction into cortical stimulation by Barker in 1985, TMS has been modified to regulate brain metabolism and nerve electrical activity in ways that stimulate currents in the cerebral cortex by time-varying magnetic fields, thus altering the action potential in cortical nerve cells. However, various rTMS strategies contribute to the heterogeneous response—for example, dual-site rTMS on the left temporal cortex and the left prefrontal cortex for tinnitus is superior to single-site rTMS over the left temporal cortex. 13,20 One-Hz rTMS on the left frontal cortex, with a view to reducing depression, can be an option to treat tinnitus-related depression. A substudy of low-frequency rTMS over the left temporal cortex and the left prefrontal cortex in tinnitus showed that either cranial tinnitus or tinnitus was temporarily, partially, or in some cases completely inhibited after the treatment. And patients with a shorter history of disease course tended to gain better symptom control, consistent with our results. The current retrospective analysis yielded the overall efficacy rates of 62.3%, 66.3%, and 63.8% regarding the THI and VAS scores and the patient subjective efficacy of rTMS in tinnitus, but slightly higher than previous estimates. 21,22 This may be attributed to the retrospective design, without access to information from well-matched placebo controls for double-blind trials, so the potential selection bias exists. Another important reason is that spontaneous remission in short-term tinnitus may add to the efficacy.
Besides, heterogeneous criteria may give insufficient adjustment for age, hearing level, disease course, and type of tinnitus and the like. But whether it is an influencing factor of clinical response to rTMS in tinnitus is still under debate. Some studies recognized short-term tinnitus (<2 years) and normal hearing as potential predictors of beneficial treatment outcomes. 23,24 Our analysis identified possible factors influencing response from all clinicodemographic parameters selected, including age, sex, tinnitus duration, tinnitus type, and location. We found a clear relationship between disease duration and the efficacy of rTMS in tinnitus, highlighting an exceptionally high proportion of responders in patients of <1-week duration. This finding suggests a shorter duration has a strong effect on rTMS efficacy. It should be noted that it is also possible those with shorter duration were more inherently prone to recovery regardless of intervention since the condition had not yet gone on to chronicity. The underlying mechanism is potentially associated with mild-to-moderate neurological dysfunction in this population, which can be readily restored after rTMS treatment. Had some of them progressed to severe disease with tinnitus persisting, their central auditory system components would have been damaged irreversibly, characterized by declining response until insensitive completely. The relationship of the efficacy of rTMS with recovery from hearing loss remains elusive, and our analysis for the THI score only reveals no significant effect on hearing recovery. There is a significant correlation of rTMS treatment with hearing type based on the VAS assessment. But it is still too early to make a definite conclusion on their relationship concerning inconsistent results based on THI and VAS data. Future studies of the potential association between hearing loss and rTMS efficacy are needed to provide strong results for better decision-making. Other factors, except for hearing loss and type and tinnitus duration, revealed no significant effect (all P > .05) on clinical response to rTMS. Besides, the multivariate regression analysis adjusted for age, sex, and tinnitus duration just showed no considerable effect on the overall response in terms of patient’s perception.
Conclusion
This study demonstrates a clear relationship between tinnitus duration, which is the only factor proved to affect the overall response in both objective assessments and the efficacy of rTMS. Patients with less than 1-week tinnitus benefit the most from rTMS, and better outcomes can be achieved in the first episode of tinnitus. Therefore, it is recommended to perform rTMS as soon as possible.
Footnotes
Authors’ Note
Haidi Yang, Gui Cheng, and Zhengrong Liang contributed equally to this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (81970887)and the Guangzhou Science and Technology Foundation (201903010088).