
Abstract
Relapsing polychondritis (RP) is a rare systemic disease that is characterized by recurrent episodic inflammation of the cartilaginous structures of the body, resulting in their progressive destruction and subsequent replacement with fibrotic scar. We present a case of RP that initially manifested with subglottic involvement and we propose an innovative strategy for the treatment for laryngeal RP in phase of active inflammation. A multidisciplinary approach (rheumatologist, otolaryngologist, immunologist, internist, cardiologist, etc) and adequate follow-up are essential. The timeliness of the diagnosis is fundamental to contain the destructive effects on the cartilages involved.
Keywords
Introduction
Relapsing polychondritis (RP) is a rare systemic disease characterized by recurrent episodic inflammation of the cartilaginous structures of the body, resulting in their progressive destruction and subsequent replacement with the fibrotic scars. It is a rare disease, with an estimated annual incidence of 3.5 cases per million. The etiology of RP is unknown, but an autoimmune origin has been proposed. 1 Moreover, it has been learned that the degree of disability caused by the disease varies. 1
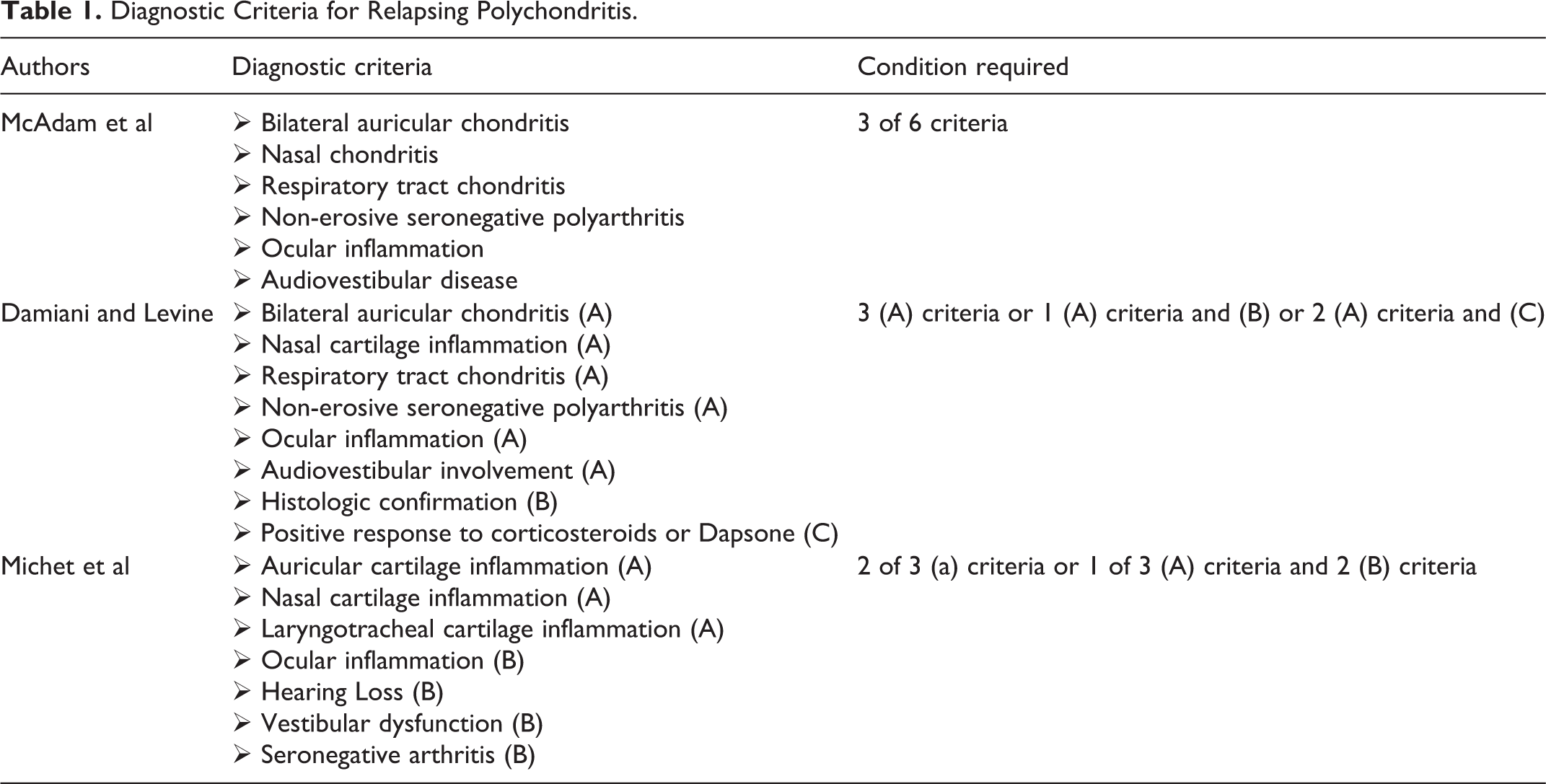
Relapsing polychondritis has no pathognomonic clinical, radiological, and histopathological features. Hence, the diagnosis depends on the presence of clinical features and diagnostic tests. In 1976, McAdam et al 1 described the clinical criteria of the disease, which were later modified by Damiani and Levine 2 and Michet et al, 3 who proposed including histological features and therapeutic response (Table 1). However, some authors have suggested liberalizing these criteria not to include histologic confirmation, although the diagnosis can be made with considerably more confidence if a tissue biopsy is available that demonstrates focal inflammatory destruction of cartilage. 4
Diagnostic Criteria for Relapsing Polychondritis.
The average age of onset of the disease is 40 to 45 years, and there appears to be no gender, racial predilection. Nevertheless, women are more affected than men (4:1 ratio). 3 Ear cartilages are the most frequently involved site in RP, accounting for almost 90% of cases. Laryngeal involvement occurs in 40% to 55% of the patients with RP and is a severe manifestation of the disease 3 ; however, only 12% of them exhibit initial airway involvement. Symptomatic airway compromise is considered a common cause of morbidity and mortality because the most frequent reason of death in RP is pulmonary infection with airway stenosis or collapse.
Patients usually present with airway compromise during the active inflammatory stages of the disease due to intense inflammatory edema of the glottic and subglottic subsites, rather than the tracheomalacia of long-standing inactive disease. Over time, dissolution of any or all laryngeal and bronchial cartilages may occur, resulting in the disruption of normal cricoid and tracheal cartilage architecture and tracheobronchial chondromalacia with inspiratory collapse. Laryngeal and tracheal involvement is characterized by diffuse circumferential involvement of the cartilages. These airway manifestations occur at a later stage in the disease and indicate a poor overall prognosis. A standard treatment protocol for RP is yet to be established. Current medical therapy is largely empirical and based on case reports. Early medical intervention can prevent and delay irreversible cartilage destruction; thus, the early detection of airway involvement is critical.
We present a case of RP that initially manifested with subglottic involvement and propose an innovative treatment strategy for laryngeal RP during the active inflammation phase.
Case Report
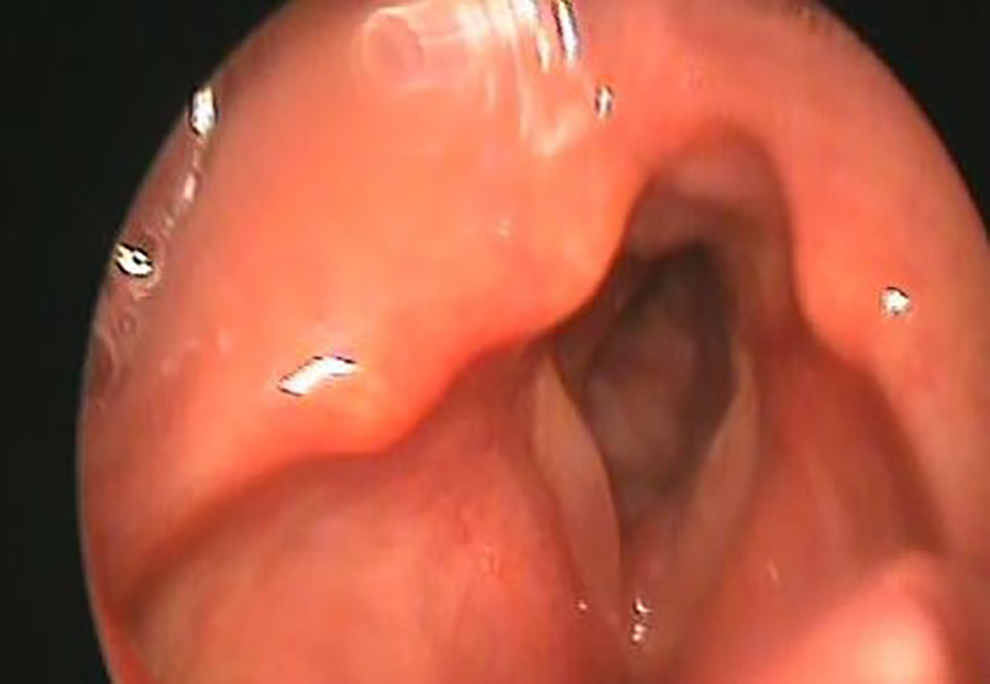
A 45-year-old female patient came to our attention for mild dyspnea, slowly worsening for 6 months, and dysphonia occurring for about one week. She had practiced 2 cycles of therapy for bronchial asthma with fast-acting β2-agonists (Salbutamol spray 2 puff, 200 µg every 8 hours for 15 days) and corticosteroids (prednisone 5 mg/d for 5 days) prescribed by the pulmonologist with modest symptomatic improvement. Fiber laryngoscopy revealed multiple spindle-shaped stenotic lesions in the subglottic area with a smooth mucosal surface that projected concentrically in the lumen, reducing its diameter and consequently the respiratory space. Vocal cord motility was preserved (Figure 1).

Laryngoscopic examination: a spindle-shaped stenotic area with smooth mucosal surface was observed in subglottic area.
The neck and chest computed tomography (CT) examination showed diffuse airway wall stenosis of the cricoid ring profile that extended to the first 2 tracheal rings. The lesions involved the cartilaginous tissue, which appeared thickened and partially calcified with an intense enhancement. Also, the CT examination indicated a distinct and widespread thickening of the tracheal ring, with the posterior connective membrane absent (Figure 2). The positron emission tomography (PET)/CT suggested an accumulation of Fluorodeoxyglucose [18F] (FDG) in correspondence with the cricoid cartilage and the cervical trachea (SUV 14). Spirometry highlighted a typical obstructive picture. No cardiovascular involvement or thyroid disease was observed. The patient underwent a laryngotracheal biopsy under general anesthesia. Histopathological examination revealed that the chorion had a massive cellular infiltrate consisting of lymphocytes, plasma cells, histiocytes, and fibroblasts gathered in some areas to form aggregates with a granulomatous appearance.

Computed tomography (CT) axial section: stenosis in the subglottic region.
The biopsy examination results correlated with the results of the laboratory tests (high inflammation indexes: sedimentation rate, C-reactive protein, fibrinogen), indicating an inflammatory pathology. The antinuclear antibody, antineutrophil cytoplasmic antibody, anti-neutrophil type P perinuclear antibodies, and rheumatoid factor were all normal in laboratory tests. In the immediate postoperative course, the patient reported an exacerbation of pain at the auricle, worsened by pressure on it, which she had suffered cyclically in the past.
The physical examination of the pinna showed a bilateral swelling of the cartilage involving helix and antehelix with tenderness and erythematous changes. The external auditory canal was normal. Moreover, the vestibular system and audiological examinations were both normal.
The patient was treated with corticosteroid therapy (prednisone per os at the dose of 1 mg/kg/d for 5 days and then switched to the dosage of 0.5 mg/kg/d for another 10 days) with an improvement of the clinical picture as early as 2 to 3 days. Subsequently, maintenance therapy was started with intramuscular triamcinolone acetonide 3 fl, 40 mg/mL every 10 days (Figure 3). The patient was enrolled in the follow-up with monthly control for the first 3 months, then quarterly.
Laryngoscopic examination after therapy.
For 11 months, there were no exacerbations of polychondritis affecting the auricles, larynx, and/or trachea. After one year, an episode of nasal chondritis occurred with pain at the root of the nose and nasal respiratory obstruction. Nasal objectivity revealed diffuse nasal mucosa congestion. In this case, the patient underwent corticosteroid therapy (prednisone per os at the dose of 1 mg/kg/d for 5 days and then switched to the dosage of 0.5 mg/kg/d for another 10 days) with a sudden improvement of the clinical symptomatologic picture. However, a deformity in the lateral view of the profile of the nose with a typical “saddle nose” appearance persisted following this episode (Figure 4).

In lateral view of the nose’s profile typical “saddle nose.”
Discussion
Relapsing polychondritis is a rare disease (3.5 cases per million people per year) with an unknown cause. It affects adults in their fourth and fifth decades of life, with Caucasians being the most affected. The prevalence is higher in women than men (4:1 ratio). The first clinical criteria were illustrated by McAdam et al 1 in 1976, later expanded by Damiani and Levine 2 in 1979, and then modified by Michet et al 3 in 1986. Diagnostic criteria for RP are shown in Table 1.
McAdam et al 1 reported that nearly half of the patients with RP had laryngotracheobronchial involvement, while, as observed in our case, extensive subglottic involvement was a rare initial manifestation. Later, typical auricular and nasal chondritis developed. A severe laryngeal involvement at presentation was described only in 10% of the cases (Table 2). Initial RP airway symptoms such as cough, hoarseness, dyspnea, wheezing, and choking, as in our case, can be misdiagnosed as bronchial asthma.
Laryngeal Sites and Management of Initial Airway Involvement in Literature Reports.
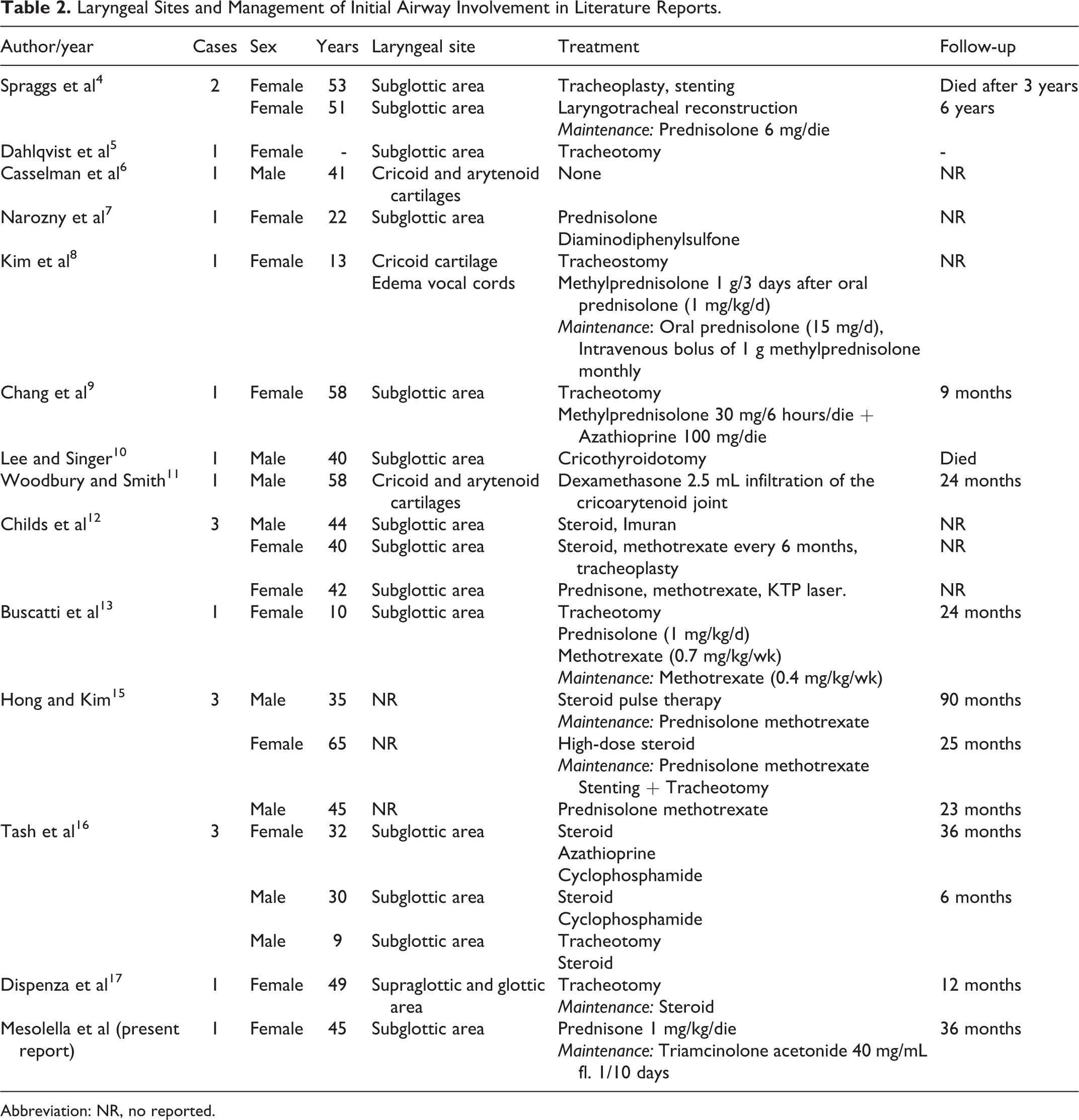
Abbreviation: NR, no reported.
In laryngeal involvement, edema develops in the airways during the active period of the disease, and fibrous tissue develops in the late period due to chronic inflammation, while the airway collapses as a result of the destruction of laryngotracheal cartilages. 1 More than 30% of the patients have other autoimmune systemic diseases (rheumatoid arthritis, necrotizing vasculitis, myelodysplastic syndromes, Graves’ disease, etc). Relapsing polychondritis is challenging to diagnose and potentially fatal because it is characterized by recurrent episodes of inflammation and the progressive destruction of the cartilage tissues.
All types of cartilage, including elastic (auricle and nose), fibrous (vertebral discs), and hyaline (tracheobronchial cartilages and small and large joints), as well as other proteoglycan-rich tissues (eye, heart, inner ear), can be involved.
There are no specific laboratory tests for RP diagnosis; however, blood tests can indicate an increase in inflammatory markers, such as elevated erythrocyte sedimentation rate and C-reactive protein. Computed tomography scans of the airway in patients with RP can reveal circumferential thickening or a “worm-eaten” appearance in affected cartilage. In the late stages, a narrowed, irregular airway lumen will develop. Computed tomography with intense post-contrast enhancement, high FDG uptake to PET-CT total body at the laryngotracheal level (standardized uptake value = 14), and the absence of specific laboratory tests and/or instrumental diagnostic elements can mimic a neoplastic lesion leading to airway obstruction. Biopsy of the involved cartilage is not usually needed if the signs and symptoms are typical. However, histopathologic findings in affected cartilage specimens, in our case, revealed loss of normal cartilage and inflammation of the perichondrium, infiltrated by neutrophils, eosinophils, lymphocytes, and plasma cells.
Due to the rarity of RP, a standard management protocol is yet to be established. 14 The treatment mainly involves the provision of symptomatic relief during different phases of the disease (initial therapy, maintenance, exacerbation phases, follow-up). 18 The diagnostic delay influences the effectiveness of the therapy and, consequently, the prognosis. In a recent study, the average interval from the onset of the first symptoms to diagnosis was 2.9 years. In 68% of the 66 patients studied, the delay in diagnosis was one year, and more than one-third of the patients had visited over 5 doctors before diagnosis.
The timely diagnosis of RP is critical for establishing an adequate therapeutic treatment to contain the destructive effects on the cartilages involved and the consequent fibrotic replacement with functional outcomes. 19 -22 Most patients experience recurrent episodes of inflammation that last from a few days to weeks. Many are asymptomatic during the remission stages, while others develop some degree of disability. Without treatment, respiratory tract involvement can be complicated and lead to airway collapse in the advanced RP stage, which is the main cause of death, accounting for almost 30% of mortality. 1 The majority of patients have a pathology with a benign course, while the minority (10%-50% of cases) can experience lethal respiratory or cardiovascular complications.
Long-term, high-dose, or pulse steroid therapy may reduce the frequency and severity of acute episodes, but it is unknown whether it affects disease progression or prevents vital organ involvement. 6,23 -26 However, steroids remain the mainstay during disease flare-ups, and continued long-term steroid use is often recommended to prevent relapses. 6,27 Methotrexate, cyclosporine, azathioprine, and cyclophosphamide have all been used to treat RP because of their steroid-sparing effect. There is no evidence that one has greater benefit than the others. Recently, biological agents (rituximab and tocilizumab) have been used in patients with RP refractory to conventional treatment, but the efficacy varies from case to case, and the experience regarding their use is minimal. Tracheotomy is necessary for patients with severe dyspnea due to obstruction that is unresponsive to medical therapy and patients with the laryngeal or tracheal cartilaginous rings collapse, airway obstruction, or broad subglottic localization. 1 Tracheotomy can complicate subsequent surgical treatments such as laryngotracheal reconstructions, 18 stenting, or laryngoplasty in case of stenosis. 5
Conclusion
Relapsing polychondritis is a rare systemic disease with various presenting manifestations that often raise major diagnostic dilemmas. 28 Many clinical criteria have been introduced for its diagnosis as there are no specific laboratory tests available. No pathognomonic biopsy finding is known for diagnosing RP. The disruption in the cartilage structure and granulation tissues appears during the natural course of the disease. The timeliness of the diagnosis is fundamental to contain the destructive effects on the cartilages involved. A multidisciplinary approach (rheumatologist, otolaryngologist, immunologist, internist, cardiologist, etc) and adequate follow-up are essential. A standard treatment protocol for RP is yet to be established. Laryngeal involvement is exhibited by only 10% of cases at presentation, but it eventually develops in half of all patients, more commonly in females. In our case, the patient’s initial manifestation of RP was only cricoid chondritis. For the first time in the literature, the patient was treated with a low-dose steroid during an acute exacerbation, with clinical improvement as early as 2 to 3 days, followed by maintenance therapy with intramuscular triamcinolone acetonide 3 fl, 40 mg/mL every 10 days. The patient responded well to treatment without any complications. This therapy could be recommended as a therapeutic option in patients with RP involving airways.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.