
Abstract

Significance Statement
Metastatic carcinomas to the larynx are rare and account for less than 1% of all laryngeal tumors. Cutaneous melanoma and renal cell carcinoma are the most frequent laryngeal metastases. Only 16 cases of laryngeal metastases from colon adenocarcinoma have been previously described in the literature. We present the first clinical report of ileocecal valve and cecum adenocarcinoma metastatic to the larynx and one cervical neck lymph node that was treated successfully with surgical excision.
Case Description
A 68-year-old male patient underwent a partial right colectomy for a pT3N2aM0 adenocarcinoma of ileocecal valve and cecum in October 2018 (Figure 1A). He was treated postoperatively with 8 cycles of chemotherapy (oxaliplatin and capecitabine). The patient was disease-free until October 2020, when he presented to an otolaryngologist complaining of a foreign body sensation in his throat, progressive dysphagia, and hemoptysis. Fiberoptic laryngoscopy detected a tongue base and left vallecula mass (Figure 1B). Neck palpation did not reveal lymphadenopathy. A neck computed tomography (CT) scan and a fluorodeoxyglucose (FDG) positron emission tomography (PET)/CT scan were performed. The CT scan showed a lesion in the left vallecula. Positron emission tomography/CT scan showed intense FDG uptake of the lesion with SUVmax of 17.2 (Figure 2). Malignant tumor was suspected, and a biopsy was taken under local anesthesia.
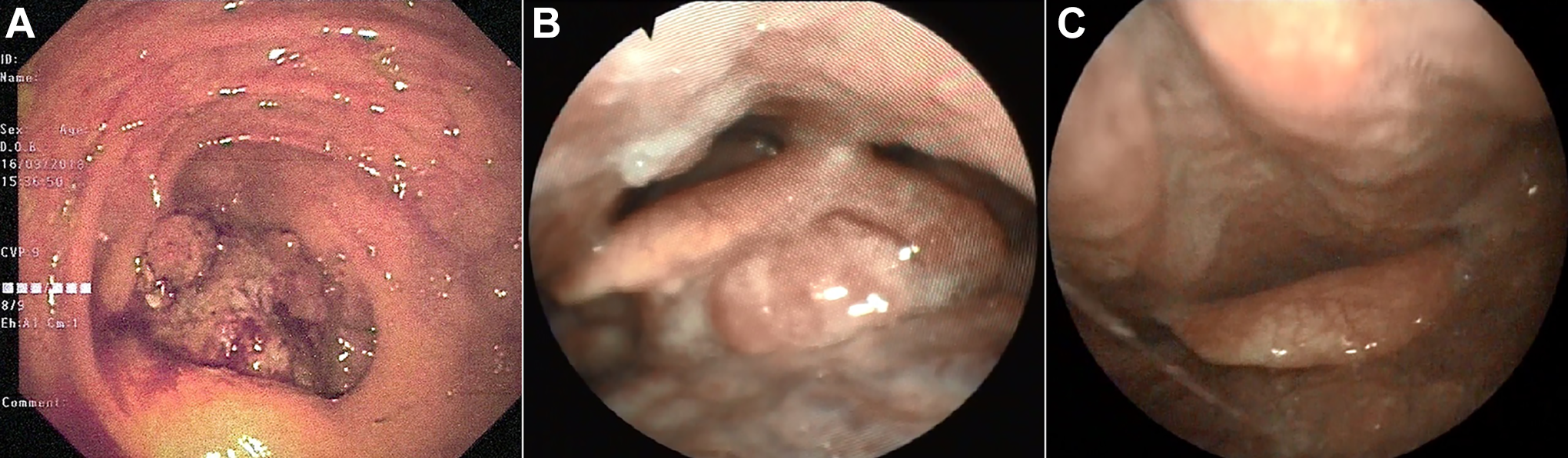
Endoscopic images. A, Endoscopic image of primary ileocecal valve and cecum tumor. B, Fiberoptic image of metastatic adenocarcinoma to the larynx. C, Postoperative fiberoptic image of supraglottic larynx after 3 months.
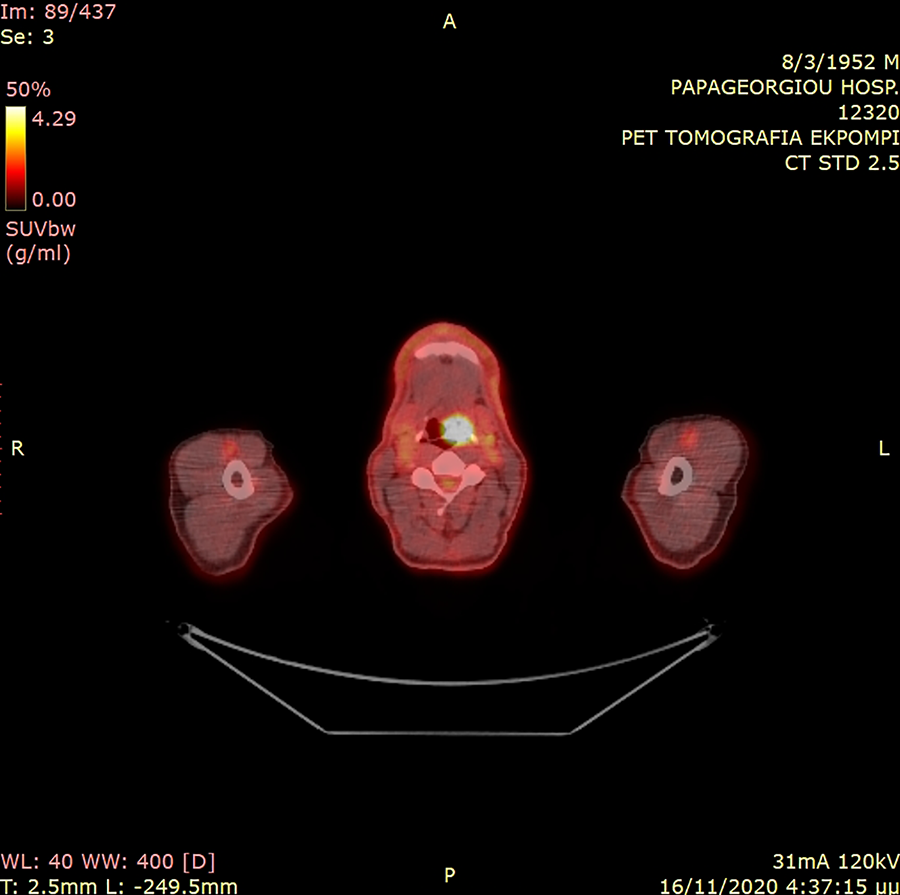
Combined fluorodeoxyglucose (FDG)-positron emission tomography (PET)/computed tomography (CT) imaging—the tumor appears as a hypermetabolic lesion (hot spot) in the left vallecula (time-of-flight [TOF] reconstruction).
The patient was referred to our ear, nose, and throat (ENT) department with the histopathological and immunohistochemical diagnosis of metastatic ileocecal valve and cecum adenocarcinoma to the larynx. Due to the outbreak of the COVID-19 pandemic in Northern Greece, the patient delayed his appointment in our Oncology ENT Clinic almost 1.5 months. At that time, although the fiberoptic endoscopic examination of his larynx was identical to his previous one, neck palpation revealed a palpable lymph node, measuring about 2 cm on the left side of the neck. After evaluation by the multidisciplinary team, direct laryngoscopy, surgical resection of the laryngeal tumor with the use of CO2 laser, and selective left side neck dissection were performed. Histopathological and immunohistochemical examinations confirmed the diagnosis of metastatic adenocarcinoma from ileocecal valve and cecum in both the larynx and one lymph node (Figure 3). Especially, the expression of cytokeratin 20 (CK20) and caudal-related homeobox transcription factor 2 (CDX2) showed that the adenocarcinoma was not a second primary malignancy but a metastatic one from ileocecal valve and cecum (Figure 3C and D). Postoperatively, the patient completed 12 cycles of chemotherapy (folinic acid, fluorouracil, irinotecan, and avastin). Follow-up after 3 months with fiberoptic endoscopy, neck palpation, and neck CT scan did not show any recurrence or metastasis of the tumor (Figure 1C).
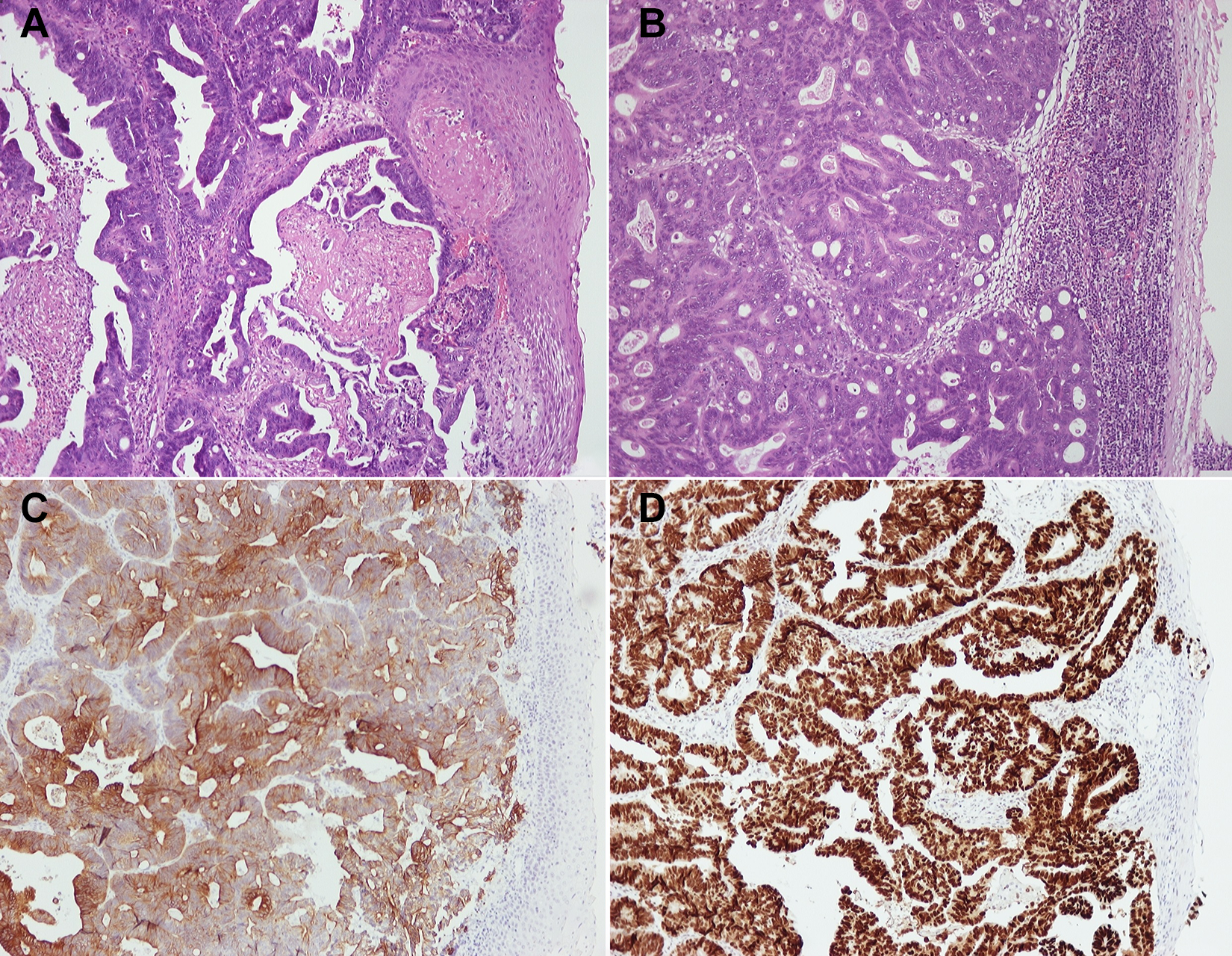
Histopathological and immunohistochemical examinations. A, Metastatic adenocarcinoma to the larynx from ileocecal valve and cecum (H&E, ×100). B, Metastatic adenocarcinoma to the lymph node (H&E, ×100). C, CK20 +. D, CDX2 +. CDX2 indicates caudal-related homeobox transcription factor 2; CK, cytokeratin; H&E, hematoxylin and eosin.
Discussion
Secondary laryngeal malignancy is an infrequent clinical entity, with an incidence ranging from 0.09% to 0.40% of all laryngeal tumors. The tumors metastatic to the larynx, in order of frequency, are skin melanoma, kidney, breast, lung, prostate, colon, stomach, and ovarian neoplasms. 1 The colon adenocarcinoma metastatic to the larynx is uncommon, and especially, the cecum and ileocecal valve adenocarcinoma is extremely rare. Only 16 clinical reports of laryngeal metastatic colonic adenocarcinoma have been presented in the literature. In 5 of these cases, the primary metastatic source was the sigmoid colon, in 1 the transverse colon, in 3 the right colon, in 1 only the cecum, and in 6 an unspecified colonic location. 2 -5 This is the first clinical report of ileocecal valve and cecum adenocarcinoma metastatic to the larynx in the literature.
The signs and symptoms of metastatic laryngeal tumors are similar to those of other primary laryngeal neoplasms, such as dyspnea, dysphonia, stridor, dysphagia, hemoptysis, otalgia, and globus sensation, depending on the site of laryngeal tumor. 6 The most common site for secondary laryngeal tumors is subglottic, followed by transglottic, supraglottic, and glottic. 2 Metastatic spread can occur via hematogenous and lymphatic routes, as in our patient. The mechanism for hematogenous spread is through the low-pressure systemic circulation, which supplies the larynx via the superior laryngeal artery. The route for lymphatic spread is via the thoracic duct, the left supraclavicular lymph nodes, and the subglottic lymph nodes. 2,6
When a primary cancer has been diagnosed previously in another site, such as the colon, a laryngeal secondary neoplasm should be considered in the presents of laryngeal symptoms. In addition, nowadays metastasis is easier to diagnose due to the increasing use of radiologic modalities such as CT, magnetic resonance imaging, and PET.
Patients with colonic adenocarcinoma metastatic to the larynx usually present with disseminated disease, so they have poor chances of long-term survival. In these patients, the laryngeal treatment is only palliative and aims at improving their quality of life. Palliative treatment includes laser endoscopic excision or debulking of the laryngeal tumor or tracheotomy in order to secure the airway. Curative treatment of laryngeal metastasis with or without lymph node metastases should be attempted in patients with no other simultaneous metastatic manifestation and a good general condition. The treatment ranges from endoscopic resection to total laryngectomy, with or without neck dissection, depending on the size and the location of the metastatic tumor.
Footnotes
Authors’ Note
The authors declare that written informed consent for patient information and images to be published was provided by the patient.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.