
Abstract
Objectives:
Olfactory dysfunction, a reduced or complete loss of the ability to smell, is gaining attention because of its substantial impact on an individual’s quality of life and the possibility that it is an important sign of underlying disease. However, olfactory dysfunction is underdiagnosed in the general population due to diagnostic difficulty and unpredictable prognosis. This study aimed to evaluate the prevalence of clinically diagnosed olfactory dysfunction in South Korea by using well-organized, nationwide, population-based cohort data, and the associations between olfactory dysfunction and risk of neurodegenerative disorders.
Methods:
We investigated the Korean National Health Insurance Service–National Sample Cohort for patients diagnosed with olfactory dysfunction according to the International Classification of Diseases. Annual and overall incidence and prevalence of olfactory dysfunction during 2003 to 2013 and patient characteristics were analyzed. Based on those identified patients who were later diagnosed with neurodegenerative disorder, hazard ratios (HRs) of sociodemographic factors and comorbidities associated with neurodegenerative disorder were evaluated using a Cox proportional hazard regression model.
Results:
In total, 6296 patients were clinically diagnosed with olfactory dysfunction during the study period (524.67 patients/year). The prevalence increased annually and was higher in female patients. The incidence of neurodegenerative disorders among patients with olfactory dysfunction was 4.2% within the study period. Multivariate cox regression analysis of the patients (n = 249) revealed that diabetes mellitus (HR = 1.976) and depression (HR = 2.758) were significant risk factors.
Conclusions:
Olfactory dysfunction is underdiagnosed in South Korea, but it is clinically important considering the possibility of presymptom of neurodegenerative disorders. In clinical practice, we should consider its association with neurodegenerative disorders and possibly other systemic conditions.
Keywords
Introduction
Olfactory dysfunction, a reduced or complete loss of ability to smell, is gaining increased attention because of its substantial impact on an individual’s quality of life and the possibility that it may be an important sign of underlying diseases. 1 Persons with olfactory dysfunction have an increased risk of harm from smoke, leaking gas, spoiled food, and hazardous chemicals. Furthermore, nutritional problems can develop due to changes in appetite caused by olfactory dysfunction. 2 However, as olfactory dysfunction is not life-threatening per se, olfactory dysfunction remains underdiagnosed in the general population, partly due to the related diagnostic difficulty and unpredictable prognosis. 3
According to the US National Health and Nutrition Examination Survey (NHANES), 12.4% of individuals in a geriatric population were found to have an impaired sense of smell and were exposed to danger from leaking gas (31.3%) and smoke (20.3). 4 A Swedish population–based study of olfactory dysfunction in individuals aged 60 to 90 years showed a prevalence of olfactory dysfunction of 24.8%. 5 In South Korea, a cross-sectional study of subjective olfactory impairment was conducted using the 2009 Korean National Health and Nutrition Examination Survey (KNHANES) data and showed a prevalence of 4.5%, which increased with increasing age. 3 However, there has been no large cohort study of olfactory impairment, clinically diagnosed by physicians, in an Asian population.
In practice, most olfactory research has been related to neurodegenerative disorders. Many reports have shown that olfactory dysfunction is the initial sign of Alzheimer disease and Parkinson disease. Olfactory dysfunction was reported in 100% of patients with Alzheimer disease, 90% of those with Parkinson’s disease, 96% of those with frontotemporal dementia, and 15% of those with vascular dementia. 6 There have been no reported investigations of possible risk factors of being diagnosed with neurodegenerative disorders in patients first diagnosed with olfactory dysfunction in South Korea.
This study therefore evaluated the incidence and prevalence of clinically diagnosed olfactory dysfunction in South Korea by using a nationwide population–based study. In this 12-year study, we investigated the incidence and prevalence of clinically diagnosed olfactory dysfunction and the associated comorbidities. Additionally, the risk of neurodegenerative disorder diagnosis in patients with olfactory dysfunction was assessed, using a representative nationwide sample of 1 million people from the National Health Insurance Service–National Sample Cohort 2002-2013 (NHIS-NSC 2002-2013) of South Korea. 6,7,8
Patients and Methods
Statement of Ethics
This study adhered to the tenets of the Declaration of Helsinki. All components and procedures of this study were approved by the institutional review board (IRB) of the National Health Insurance Medical Center, Gyeonggi-do, Korea (IRB File No.: NHIMC 2017-08-025).
Database
A retrospective cohort study was performed using the NHIS-NSC (NHIS-2017-02-032) of South Korea (2002-2013). The profile of the NHIS-NSC 2002 to 2013 was published elsewhere in detail. 7,8 In brief, a representative sample of approximately 1 million South Korean individuals was randomly selected, comprising 2.2% of the total eligible Korean population in 2002 as Korean National Health Insurance Service (KNHIS) database. 6 This sample was followed for 12 years, until 2013. The database provides detailed information on diagnostic codes, procedures, and personal information on this population sample and contains reimbursement records from all types of medical facilities. 7,8,9 This database included 6296 patients diagnosed with olfactory dysfunction. Patients with olfactory dysfunction were defined as those diagnosed with “anosmia,” “parosmia, hyperosmia, hyposmia,” 10 “other and unspecified disturbances of smell and taste,” and “disorders of olfactory nerve,” according to the International Classification of Diseases-10 (ICD-10; R43.0, R43.1, R43.8, and G52.0, respectively) by a physician (Table 1). Korean National Health Insurance Service data do not include any information about the validity of the diagnosis and severity of olfactory dysfunction. Korean National Health Insurance does not cover objective olfactory tests, and so olfactory dysfunction group was defined based only on the diagnostic codes of the claim data. Allergic rhinitis, chronic sinusitis, nasal septal deviation, and nasal polyps have been found to lead to conductive olfactory dysfunction by obstructing the olfactory fissure. The prevalence of these rhinologic disorders was evaluated. Common chronic diseases, including hypertension, diabetes mellitus, asthma, thyroid diseases, arrhythmia, chronic heart failure, chronic renal failure, and depression, were considered as other comorbidities for analysis. All comorbidities evaluated were diagnosed on the basis of the ICD-10 in 2002 to 2013.
ICD-10 Code and Diagnoses Related to Olfactory Dysfunction.
Abbreviation: ICD-10, International Classification of Diseases-10.
The second part of the study focused on the relationship between olfactory dysfunction and neurodegenerative disorders. Patients diagnosed with olfactory dysfunction from 2003 to 2013 (n = 5919), excluding year 2002 as a washout period, were analyzed to establish the relationship with neurodegenerative disorders. Within the olfactory dysfunction group, we counted patients who were newly diagnosed with neurodegenerative disorders during the study period (n = 249). Neurodegenerative disorders were defined as a physician-based clinical diagnosis of dementia in Alzheimer disease, vascular dementia, Huntington disease, Parkinson disease, Alzheimer disease, or multiple sclerosis on the basis of the ICD-10. In those patients with newly diagnosed neurodegenerative disorders, we analyzed the hazard ratio (HR) and 95% CIs for each variable. A P value < .05 was considered significant. All analyses were performed with SAS Version 9.4.
Results
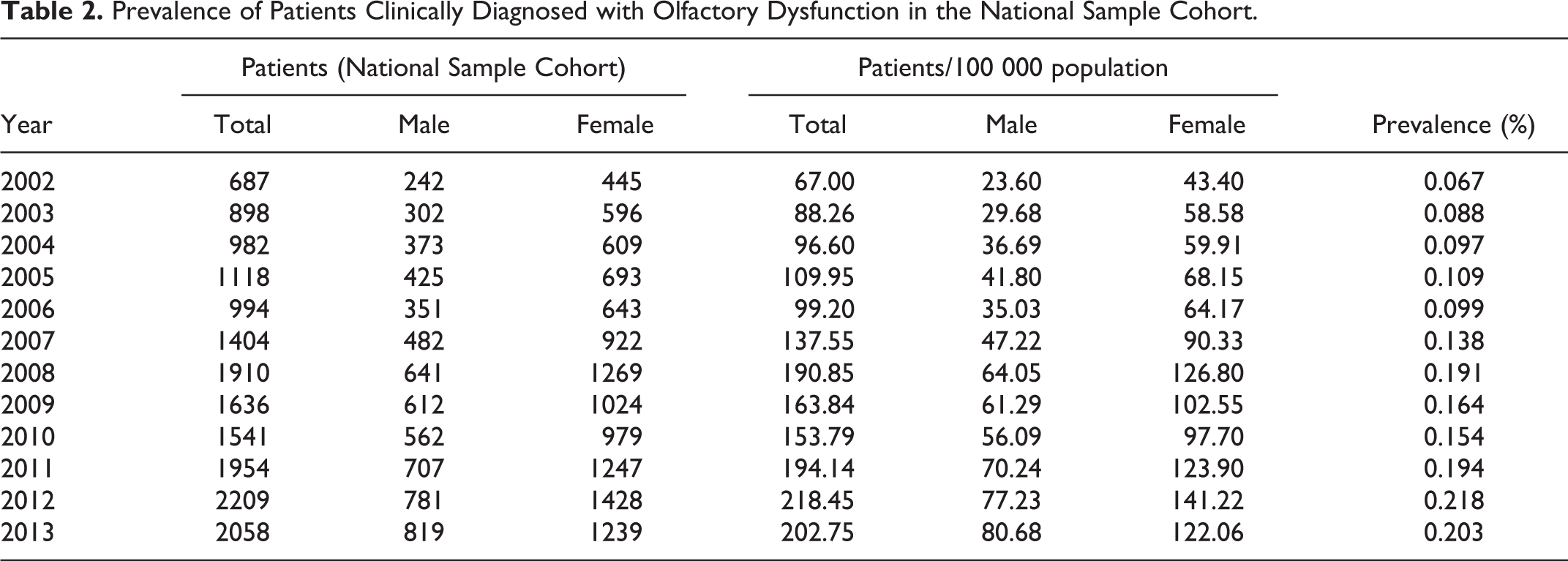
A total of 6296 patients were clinically diagnosed with olfactory dysfunction during the study period (2002-2013), with an average of 524.67 patients per year. The prevalence of olfactory dysfunction gradually increased from 2002 to 2007, and there was a rapid increase from 2007. In 2013, there were about 3 times more patients diagnosed with olfactory dysfunction than in 2002 (Table 2). The incidence of olfactory dysfunction also rapidly increased from 2011, while that, in 2013, was 1.78 times higher than in 2002 (Figure 1). The prevalence in females was consistently higher than that in males, in every year (1.76 times higher on average), and the incidence in females was also similarly higher.
Prevalence of Patients Clinically Diagnosed with Olfactory Dysfunction in the National Sample Cohort.
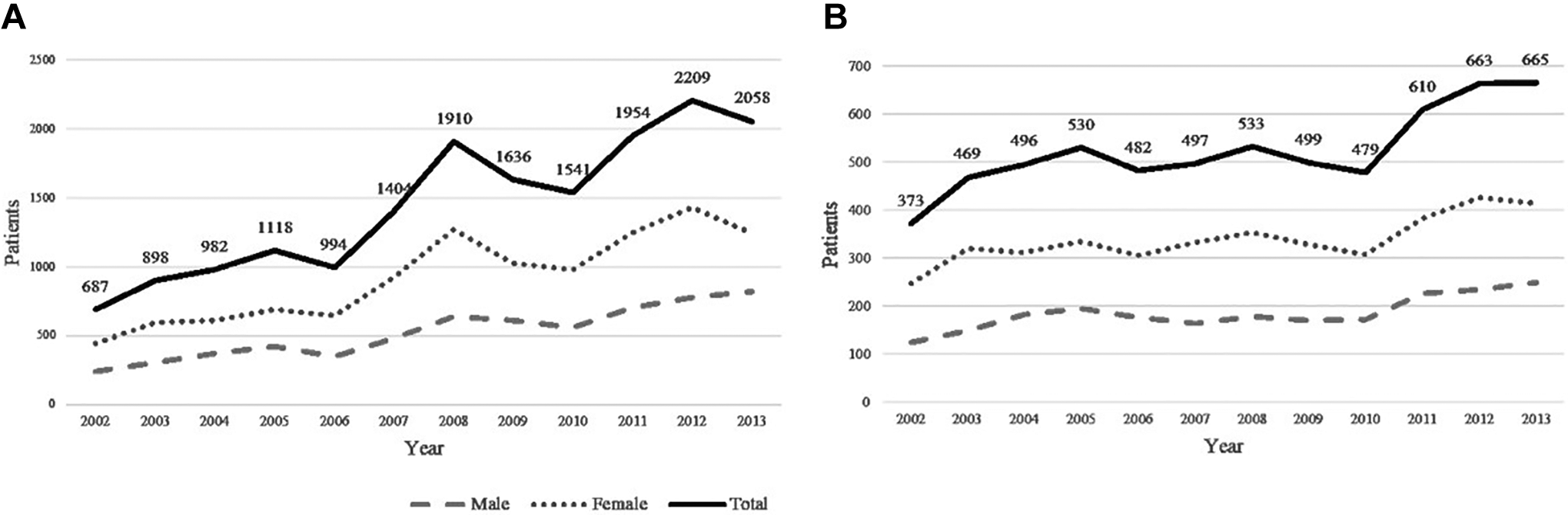
A, Prevalence of clinically diagnosed olfactory dysfunction in National Sample Cohort. B) Incidence of clinically diagnosed olfactory dysfunction in National Sample Cohort.
Table 3 shows the demographic characteristics of patients clinically diagnosed with olfactory dysfunction in the NSC. Pediatric patients less than 10 years of age were not investigated. The incidence of olfactory dysfunction was highest in those in their 40s until 2010, and from 2011, the incidence was highest in those in their 50s, while the prevalence was highest in the 40- to 50-year age-group (mean 45.91 years). However, recently, the tendency for olfactory disorder diagnosis in patients over 60 years has increased, as below. Residence, body mass index (BMI) and smoking were not significantly different between groups.
Cox Proportional Hazard Regression Analysis of the Risk of Developing De-Novo Neurodegenerative Disorders Among Patients With Olfactory Dysfunction.
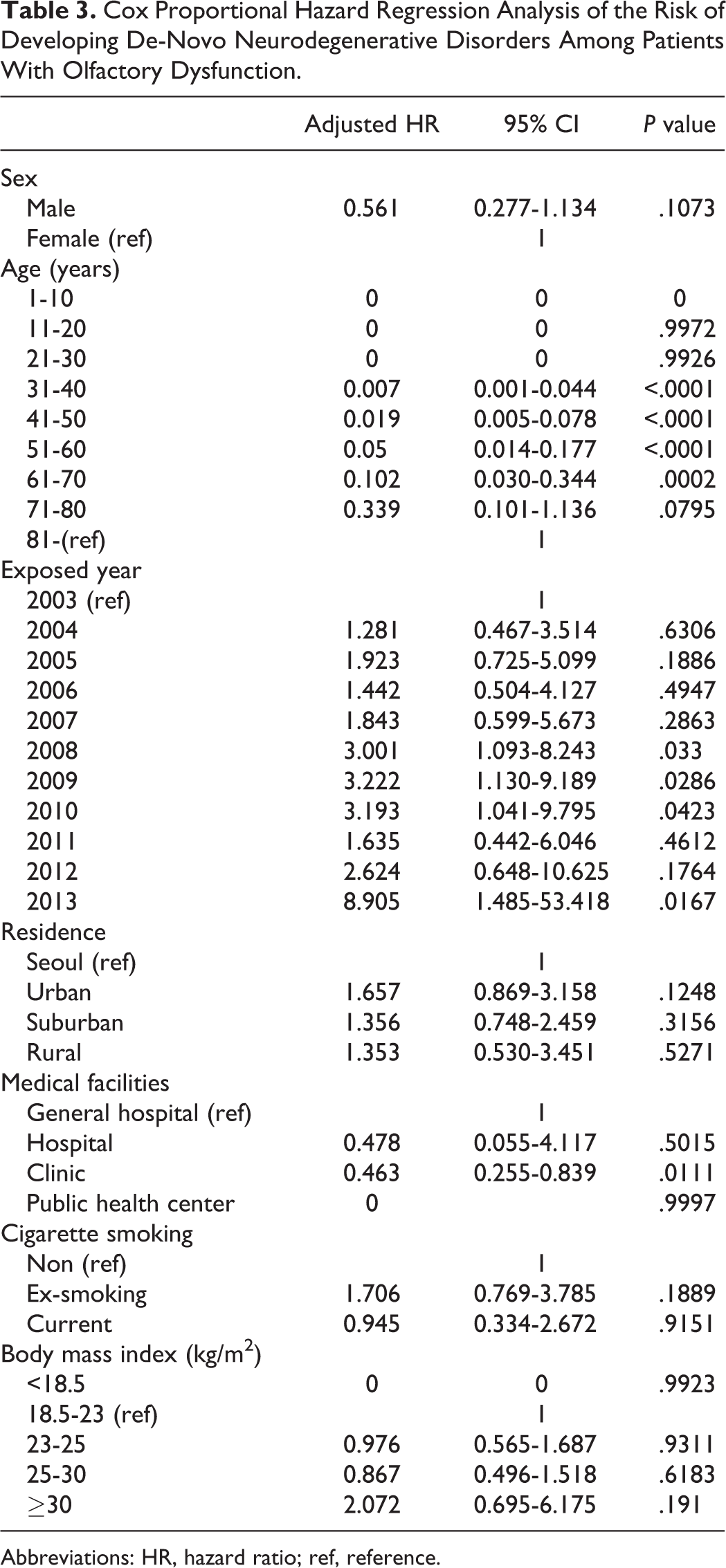
Abbreviations: HR, hazard ratio; ref, reference.
Relation of Olfactory Dysfunction, Comorbidities, and Neurodegenerative Disorders
Table 4 shows the HR for olfactory dysfunction during the follow-up period from 2003 (considering 2002 as a washout period) in patients with no history of neurodegenerative disease (n = 5919), based on multivariate Cox proportional hazard regression analysis. An increased prevalence of olfactory dysfunction was significantly associated with increasing age in both men and women; however, no significant difference was observed between the sexes. Patients under medical care were more likely to have neurodegenerative disorders than patients with regular medical insurance (HR = 3.344, P < .05). Patients who belonged to the low-income subgroup were more likely to have neurodegenerative disorders than those in the medical aid program group, the minimum livelihood of low-income households (HR = 2.791). Body mass index, cigarette smoking, and medical facility did not show any significant relationship with olfactory disorder diagnosis.
Cox Proportional Hazard Regression Analysis on the Association Between Comorbidities of Olfactory Dysfunction Patients and Neurodegenerative Disorders.
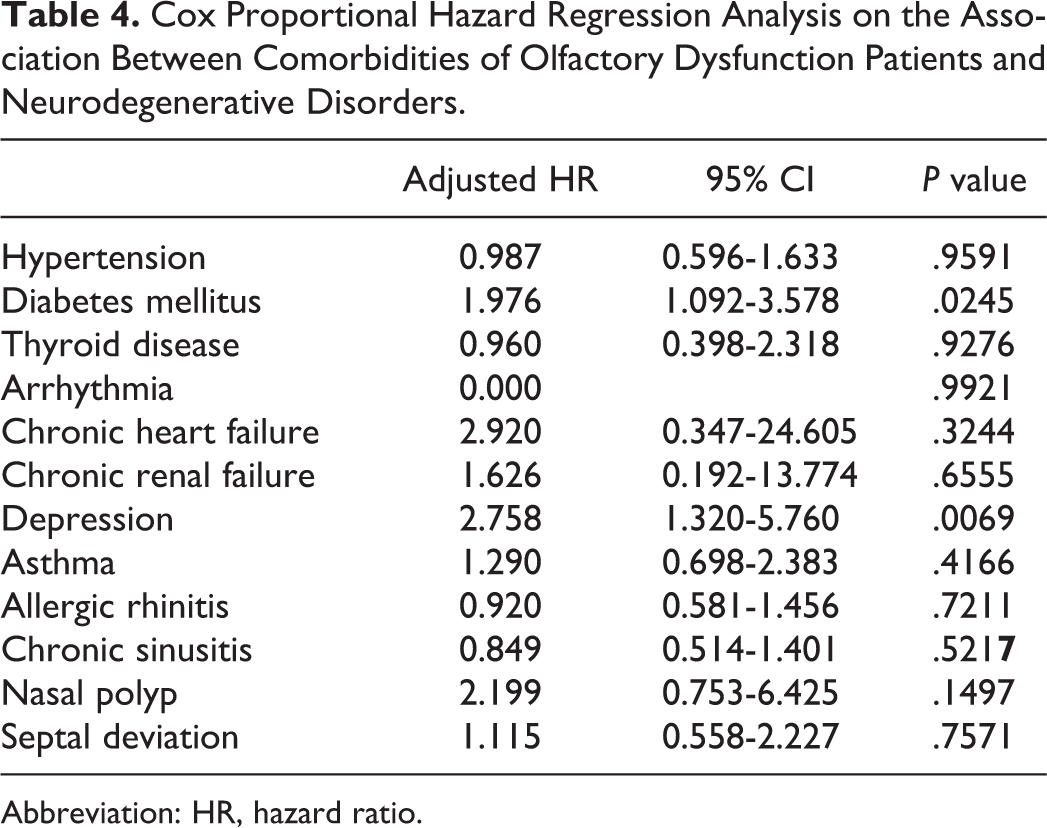
Abbreviation: HR, hazard ratio.
The period from diagnosis of the olfactory dysfunction to the diagnosis of neurodegenerative disorder was also evaluated. The closer the year was to the reference year, 2003, the higher the risk ratio was, with statistical significance, which showed that patients with longer duration having olfactory dysfunction were less likely to be diagnosed with neurodegenerative disorders subsequently (2013: HR = 8.905).
In terms of comorbidities, in descending order by effect size (as approximated by HR), patients with depression (HR = 2.758) and diabetes mellitus (HR = 1.976) were more likely to be diagnosed with neurodegenerative disorder after a diagnosis of olfactory dysfunction than were those who did not have such medical conditions (Tables 3 and 4, Figure 2).
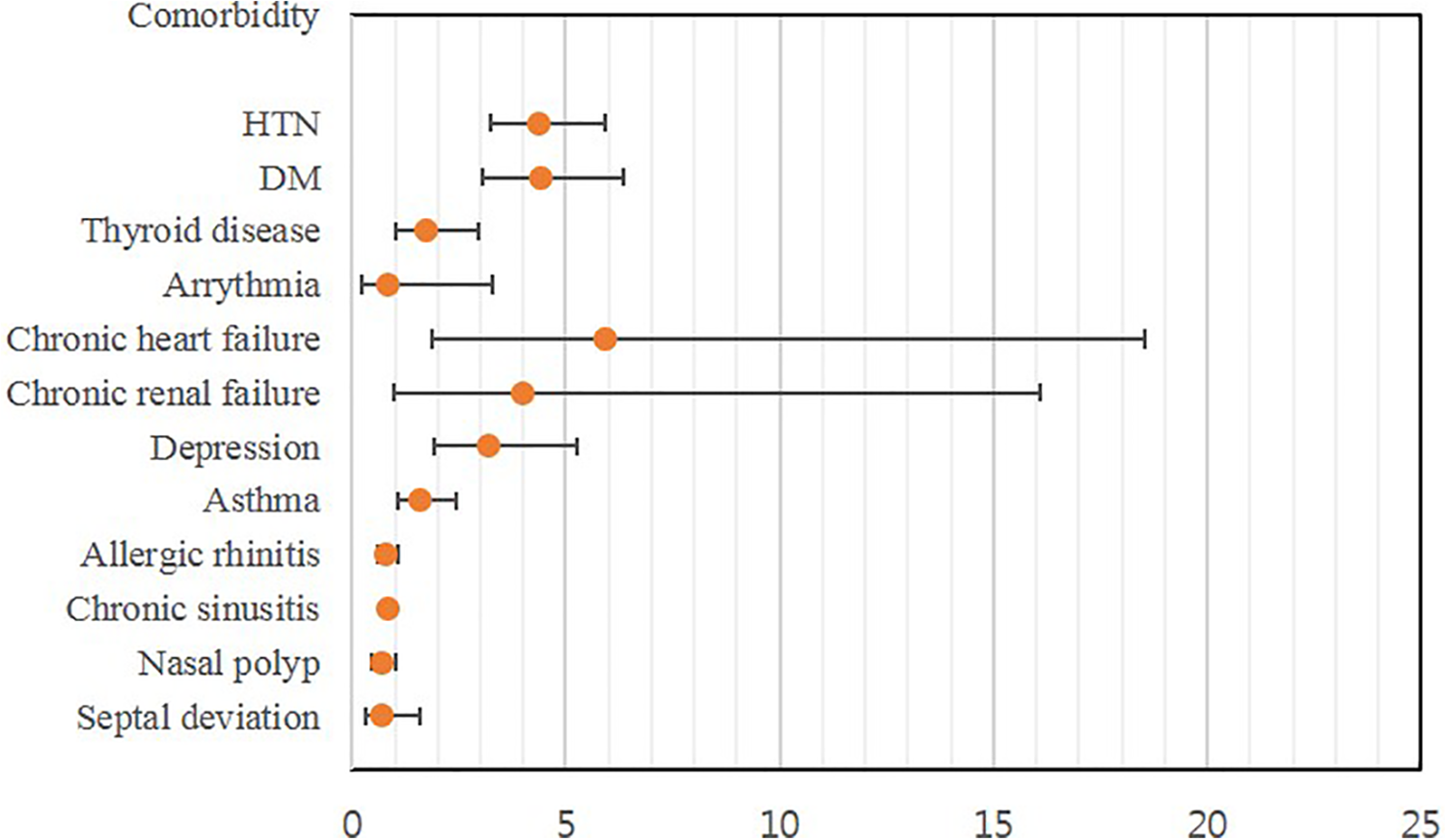
Forest plot of hazard ratio (HR) between comorbidities of patients with clinically diagnosed olfactory dysfunction and neurodegenerative disorders.
Discussion
In this study, we assessed the prevalence and incidence of olfactory disorders in a national population–based cohort in South Korea and also investigated the likelihood of such patients subsequently receiving a diagnosis of neurodegenerative disorder. The condition is still underdiagnosed in South Korea, but it may be associated with later neurodegenerative diseases, especially in patients with comorbid diabetes and depression.
According to published reports in other countries using cohort study, the prevalence of olfactory dysfunction has been reported as follows in general population over 55 years: hyposmia in 13% to 18%, anosmia in 4% to 6%, and in 9% of males and 4% of females, olfactory impairments were proven with objective olfactory tests. 1 Previously, Lee et al reported the prevalence of self-reported olfactory dysfunction in South Koreans as 4.5%, based on KNHANES data. 3 However, self-reported olfactory dysfunction had a low sensitivity (43.9%), and high specificity (85.4%), which emphasizes that there are much fewer patients who actually visit the hospital with an olfactory problem than there are individuals experiencing symptoms subjectively. 9,11,12 It is important to know and analyze the prevalence of patients diagnosed with olfactory dysfunction and to understand their characteristics, including comorbidities, but no previous study has investigated patients with olfactory dysfunction using KNHIS data to analyze at a nationwide, population-based level. Using KNHIS data, actual claim data registered by clinicians could be analyzed including diagnostic code, comorbid disease, and sociodemographic data.
The present study found that the average incidence of clinically diagnosed olfactory dysfunction in South Korea was 51.9 per 100 000 person-years and its overall prevalence was 0.14% during 2002 to 2013. The prevalence tended to increase throughout the observation period, from 0.07% in 2002 to 0.21% in 2013. The significant characteristics of patients diagnosed with olfactory dysfunction, that is, female, middle-aged (40s-60s), were similar to those previously reported. In terms of comorbidities, allergic rhinitis, acute sinusitis, chronic sinusitis, and septal deviation were common; these can affect olfactory mucosa inflammation and swelling locally, resulting in conductive olfactory dysfunction. Hypertension, asthma, diabetes, thyroid disease, and depression were the most prevalent comorbid medical conditions in patients diagnosed with olfactory dysfunction.
The prevalence of olfactory dysfunction in the study is very low compared to the other studies including the KNHANES study. We could not certainly explain the difference in the prevalence using KNHIS data and other studies. One possible explanation could be a discrepancy made by Korean National Health Insurance system between symptoms of patients and claim data which diagnosis (ICD-10) was registered by clinicians. In clinical consultation, patients describe about their olfactory symptoms; however, it usually does not proceed to registering the diagnosis of olfactory dysfunction and rather diagnostic code of sinusitis and/or rhinitis with easier clinical accessibility in primary care. However, our findings at least show that the prevalence of olfactory dysfunction tends to increase over 3 times in 11 years, and physicians have perceived a clinical importance of olfactory dysfunction as its own diagnostic meaning.
Since 2007, the incidence of olfactory dysfunction has increased, and particularly since 2011, it has increased in the age subgroup of 60 years and older. This may emphasize the recent increased public interest in olfaction and the need for improved quality of life, 12,13 while the mass media has reported the importance of olfaction and its possible association with neurodegenerative disorders.
Several previous reports have described a significant association between neurodegenerative disorders and olfactory dysfunction; thus, this study sought to identify the demographic factors and comorbidities of patients with olfactory dysfunction that can affect the likelihood of developing neurodegenerative disorders. Age, lower socioeconomic status, diabetes, and depression were the significant factors associated with an increased risk of subsequently developing neurodegenerative disorders.
Depression had the highest HR associated with neurodegenerative disorders. Patients with olfactory dysfunction often complain about a poorer quality of life and decreased appetite and social activities. 13 A decreased interest in eating and experiencing social security, increased anxiety regarding safety, and difficulty in managing personal hygiene could lead to less social participation and is likely to foster development of depression. 13,14 Decreased inputs in the olfactory bulb lead to decreased signals to the amygdala and limbic circuit, and eventually affect general cerebral function, which may result in depression and affect about 25% to 33% patients with olfactory dysfunction. 15
Taalman et al stated that there are changes in olfactory functioning in depression after reviewing the relationship between olfactory dysfunction and depression reported in the literature. 16 They also suggested that treatment of depression could improve not only the depressive symptoms but also the associated olfactory dysfunction. However, the causal relationship between olfactory dysfunction and depression is not yet clear. Further studies are needed to clarify the relationship between olfactory dysfunction and depression and to investigate the change in this pattern after treatment of depression.
The percentages of individuals with low BMI and those who were overweight/obese were higher than that of individuals with normal BMI in this study, which might reflect how appetite is affected by olfactory dysfunction. Loss of appetite could lead to weight loss, and increased food intake caused by decreased olfactory and taste cognition could lead to weight gain. Interestingly, patients with eating disorders tend to have olfactory dysfunction. In studies of olfactory dysfunction in individuals with eating disorders, patients with anorexia nervosa had a significantly lower detection threshold for food-related odors, but only when hungry, and these patients also showed significant deficits in odor discrimination and identification. 17 Rapps et al reported significant differences in odor identification between patients with anorexia nervosa and healthy controls: Patients had lower scores of odor identification. 18 Other studies reported that patients with bulimia and anorexia nervosa showed poorer olfactory and gustatory functions than did healthy controls and showed hyposmia in olfactory function tests. 19 Olfactory dysfunction was noted in both anorexia and bulimia patients, which implies that eating habits could be altered in relation to olfactory dysfunction.
Thus, considering the long-term effect caused by olfactory dysfunction to the neurologic system, several other psychiatric and neurodegenerative disorders might have significant associations, and further studies should be conducted.
Few studies have reported the relationship between olfactory dysfunction and diabetes and have suggested a significantly higher prevalence of olfactory dysfunction in patients with diabetes. Zaghloul et al reported that patients who had had diabetes for a long period had associated neuropathy, including microvascular and macrovascular neuropathy, and complained about olfactory dysfunction. 20,21 Furthermore, a significantly higher prevalence of olfactory dysfunction was reported in patients with diabetic retinopathy. 22 Several recent study data indicated that different forms of diabetic neuropathy are associated with impaired olfaction. As well as the relationship between diabetes and olfactory dysfunction, both disorders in relation with cognitive dysfunction need to be studied for their relations considering durations of diseases and associated complications.
Little is known about the epidemiology of olfactory dysfunction, despite a clinical awareness that olfactory dysfunction is one of the most commonly encountered symptoms. This may be because the diagnosis of olfactory dysfunction is complicated by the lack of imaging confirmation in sensorineural components and the lack of standardized olfactory tests. 9,10 Several olfactory tests, such as the Sniffin’ Stick test and UPSIT, have been suggested as objective olfactory tests; however, as olfaction mostly relies on cultural and social lifetime exposure, it remains difficult to standardize olfactory tests. 2,12
This study has several limitations. First, diagnosis of olfactory dysfunction was based only on the diagnostic code of the claim data. This study could not distinguish between patients diagnosed with clinical objective olfactory tests and patients based on subjective reporting. Thus, the results are based on statistical analysis of individuals who presented at a clinic with symptoms of olfactory dysfunction and were assigned a diagnostic code related to olfactory dysfunction, either alone or together with other diagnostic codes, by the examining physicians. Therefore, this study may not be an exact reflection of the true epidemiology of olfactory dysfunction as its lower prevalence compared to other previous epidemiologic studies. This could emphasize the physician might underestimate the olfactory dysfunction as a symptom, not as diagnosis. Also, presently, objective olfactory function test is not covered by the National Health Insurance System in South Korea, and it is infeasible to distinguish that the diagnosis was based on the objective test and/or self-reported symptom. Second, this study could not represent general population with olfactory dysfunction, as this study analyzed NHIS claim data, representing patients visited clinics and diagnosed with the certain diagnostic codes. The general population especially geriatric population would also contain a large number of patients with olfactory dysfunction.
Third, there were not enough data available on confounders involved in both olfactory dysfunction and neurodegenerative disorders, including environmental and genetic factors. It is not impossible to clearly establish a causal relationship. Fourth, this study was not a controlled experimental study, survival analysis on patients with olfactory dysfunction and control group in 2003 would be needed to confirm presence of olfactory disorder really associated with the diagnosis of neurodegenerative disorders. These limitations need to be considered in a future study.
Conclusion
Olfactory dysfunction is underdiagnosed in South Korea, but its clinical importance should be considered as the possibility of presymptom of neurodegenerative disorders.
Supplemental Material
Supplemental Material, sj-docx-1-ear-10.1177_01455613211012906 - Incidence of Olfactory Dysfunction and Associated Factors: A Nationwide Cohort Study From South Korea
Supplemental Material, sj-docx-1-ear-10.1177_01455613211012906 for Incidence of Olfactory Dysfunction and Associated Factors: A Nationwide Cohort Study From South Korea by Hyo Jin Chung, Hyun Seon Lim, Kyuin Lee, Hyun Seung Choi, Junhui Jeong, Hyang Ae Shin, Chang-Hoon Kim and Jung Hyun Chang in Ear, Nose & Throat Journal
Footnotes
Authors’ Note
All components and procedures of this study were approved by the Institutional Review Board (IRB) of National Health Insurance Medical Center (NHIMC) (IRB File No.: NHIMC 2017-08-025).
Acknowledgments
This study used the NHIS-NCS 2002-2013 (NHIS-2017-20-032), provided by the National Health Insurance Service.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study used National Sample Cohort data (NHIS-2017-20-032), provided by NHIS and financially supported by NHIS.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.