
Abstract
Objective:
As a result of the COVID-19 pandemic that occurred in the last year, it has been revealed that severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) does not only cause viral respiratory tract infection but can also affect many organs in the short or long term. In our study, we aimed to reveal that COVID-19 infection affects the endocrine system and triggers subacute thyroiditis (SAT) in the acute period.
Material and Method:
In our retrospective study, the ear-nose-throat examination, internal diseases consultation (investigation of COVID-19 symptoms and polymerase chain reaction [PCR] test), routine blood tests, T3, T4, thyroid-stimulating hormone, antithyroglobulin (anti-TG), antithyroid peroxidase (anti-TPO), thyroid scintigraphy, and thyroid ultrasonography results of 5 patients who applied to the otorhinolaryngology clinic due to complaints of neck pain and odynophagia between April 2020 and February 2021 were examined.
Findings:
All 5 patients were female patients (30.4 years) with odynophagia and pain in the front lower region of the neck. These patients had no previous history of thyroiditis. COVID-19 PCR tests of the patients diagnosed with SAT were positive, and there were no typical COVID-19 signs and symptoms except odynophagia and neck pain.
Result:
It comes in view that SARS-COV-2 affects thyroid functions and causes SAT and the main symptoms in patients are pain in the neck and odynophagia.
Introduction
During the ongoing COVID-19 pandemic caused by severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2), nearly 100 million people have become sick and more than 2 million have died worldwide. 1 Many researchers have focused on the pathological activity of SARS-CoV-2 in the respiratory tract and lungs, although it also affects many other organs and systems, including the respiratory, cardiovascular, gastrointestinal, genitourinary, and neural systems.2,3 Recently, thyroid pathologies associated with the endocrine system during or after COVID infection have been reported in the literature. During the active period of COVID-19 infection in these cases, symptoms of thyroiditis, including swelling and pain in the front part of the neck, were observed. Subacute thyroiditis (SAT; eg, de Quervain thyroiditis, granulomatous thyroiditis) is a self-limiting inflammatory thyroid disease resulting from viral infection accompanied by thyrotoxicosis. 4
The patients in the present study, who had been admitted to the otorhinolaryngology polyclinic due to complaints of neck pain and odynophagia, were asymptomatic COVID-19 patients identified based on routine laboratory examinations and polymerase chain reaction (PCR) tests. Whether SARS-CoV-2 triggered SAT was investigated.
Methods
This retrospective study included 5 patients who had been admitted to the otorhinolaryngology polyclinic of Istanbul’s Yeni Yuzyil Faculty of Medicine, Bahat Hospital. The patients complained of neck pain and odynophagia and were admitted between April 2020 and February 2021. Patients were followed up on for an average of 10 weeks from the day on which they first complained of neck pain.
Patient age, gender, and anamnesis data were obtained, and a detailed ear, nose, and throat examination, investigation of COVID-19 symptoms and PCR test, routine blood tests (C-reactive protein [CRP] and erythrocyte sedimentation rate [ESR]), FT3, FT4, thyroid-stimulating hormone (TSH), antithyroglobulin (anti-TG), and antithyroid peroxidase (anti-TPO) analyses, and thyroid scintigraphy and ultrasonography (USG) were performed.
Approval from the Istanbul Yeni Yuzyil University Ethics Committee for Non-Invasive Health Sciences Research (Date: February/01/2021; Decision No: 2021/02-594) was obtained for the study.
Results
The 5 patients were all female and their average age was 30.4 years. Common complaints included neck pain, ear pain when swallowing, and odynophagia. Symptoms of thyrotoxicosis such as palpitations, irritability, sweating, weight loss, and weakness were noted in their anamnesis. None of the patients had any previous complaints or symptoms associated with thyroiditis.
All patients had pain and stiffness in the thyroid region upon neck palpation and painful lymphadenopathy in the cervical and submandibular regions.
Although none of the patients had signs of active viral respiratory tract infection, PCR tests showed all patients were positive for COVID-19.
As shown in Table 1, the FT3 and FT4 levels were high, TSH was low, and the CRP sedimentation rate was high in all patients. Moreover, all patients were anti-TPO- and anti-TG-negative. On thyroid USG and Doppler examinations, diffuse lobular growth, a hypoechogenic thyroid gland, and reduced blood flow were observed in the thyroid tissue (Figure 1). On thyroid scintigraphy, low uptake was observed in the remaining thyroid tissue (Figure 2).
Summary of Patient Results or Summary of Patient Data.a
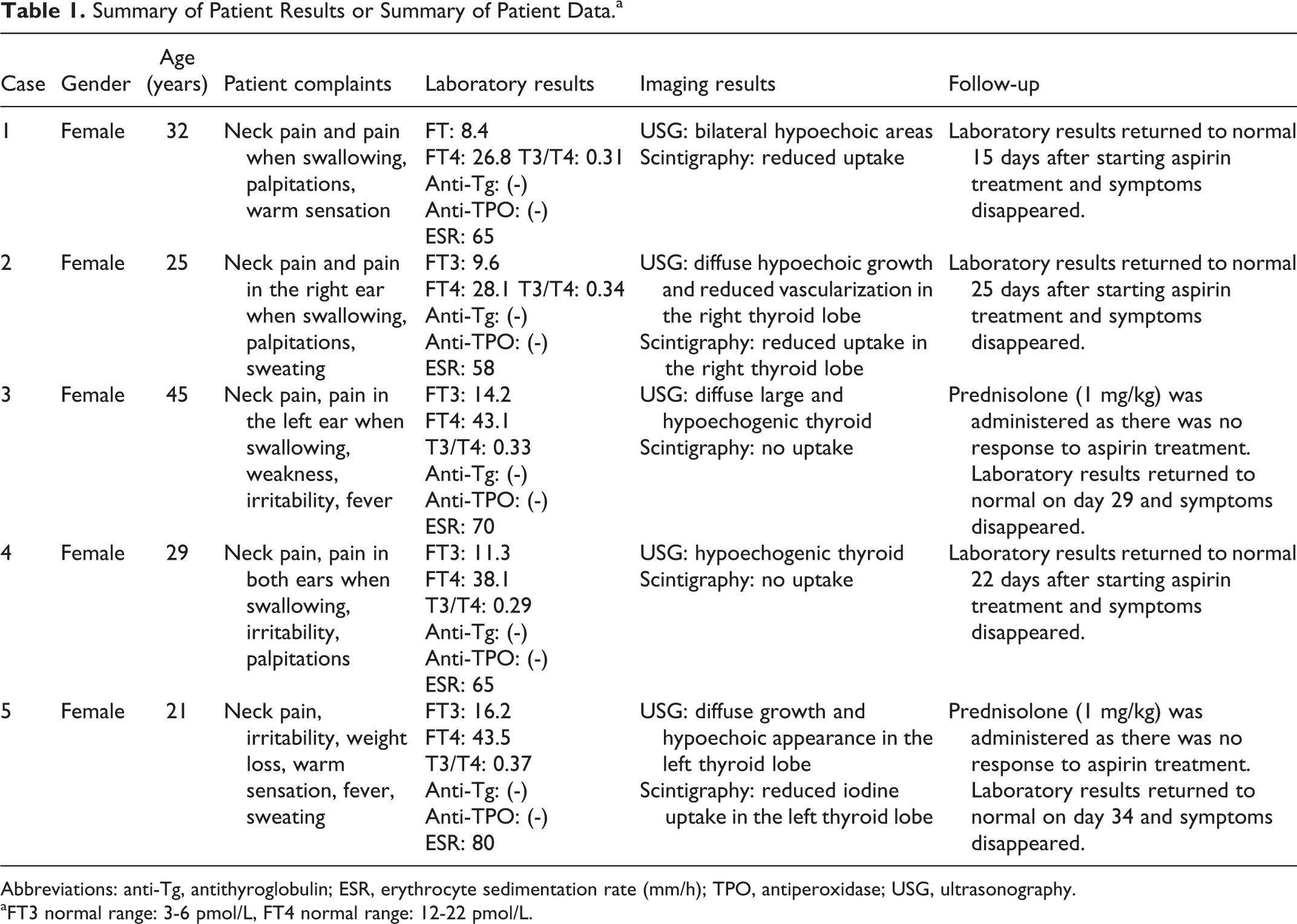
Abbreviations: anti-Tg, antithyroglobulin; ESR, erythrocyte sedimentation rate (mm/h); TPO, antiperoxidase; USG, ultrasonography.
aFT3 normal range: 3-6 pmol/L, FT4 normal range: 12-22 pmol/L.
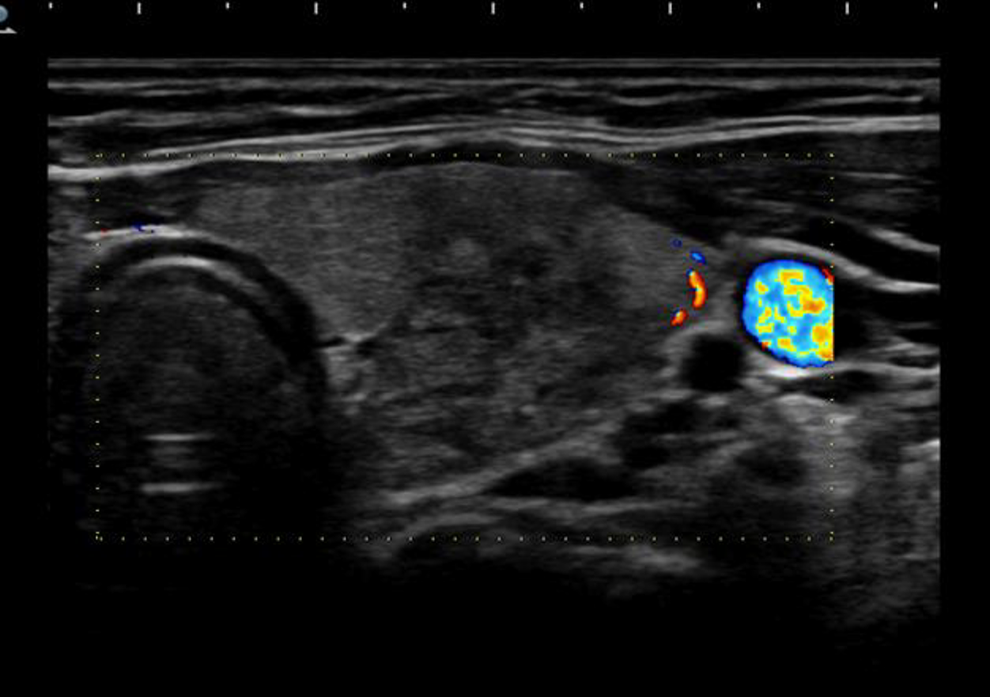
Thyroid ultrasonography (USG) and Doppler reveled enlarged thyroid tissue, hypoechogenicity, and low blood flow.
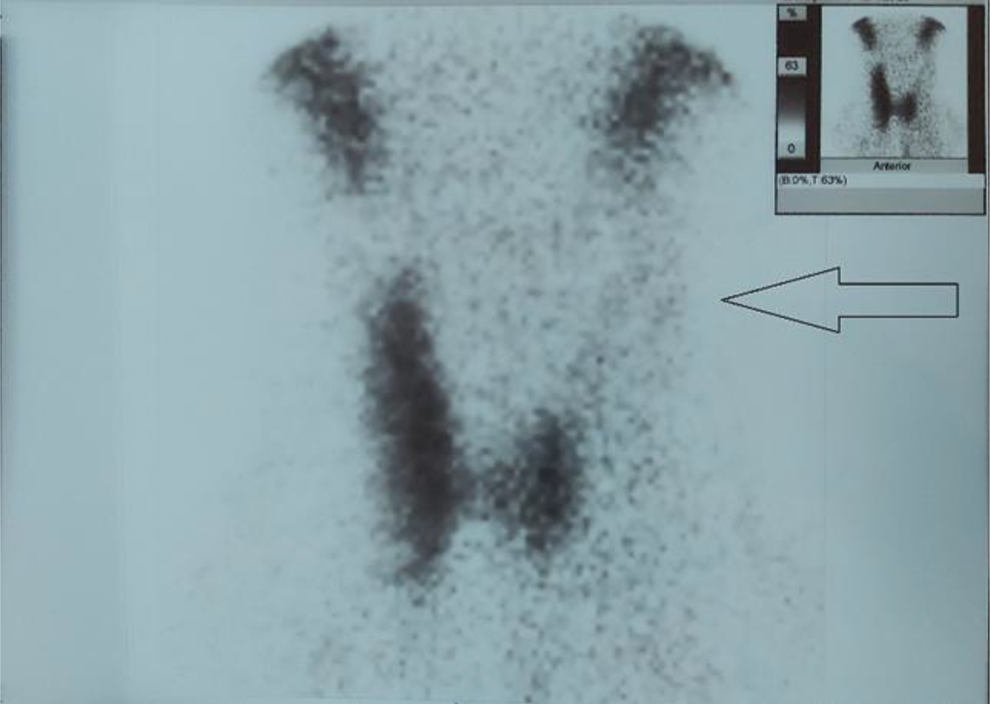
In thyroid scintigraphy, there was no uptake in the left thyroid lobe (indicated by the arrow).
All patients received aspirin (approximately 3 g/d) for 5 days. However, because thyrotoxicosis and neck pain did not decrease in 2 patients, prednisolone was started at a daily dose of 1 mg/kg and was then tapered off over 10 days. The symptoms, signs, and T3, T4, and TSH values of all patients decreased within an average of 25 days (range: 15-34 days) to normal values.
Discussion
Subacute thyroiditis is generally triggered by upper respiratory tract infections such as influenza, adenovirus, Coxsackievirus, Epstein-Barr virus, and cytomegalovirus. 4 The incidence of SAT has increased with the COVID pandemic (12.1 cases per 100 000 patients per year) and is mostly observed in young females.5,6
Patients characteristically complain of swelling and neck pain. In addition, painful diffuse goiter upon palpation, pain in the neck and ear while swallowing, myalgia, subfebrile fever, weakness, and hyperthyroidism may be present during the acute period. Shortly after the onset of pain, complaints such as irritability, insomnia, heat intolerance, sweating, tremor, and palpitations may occur in association with the thyrotoxicosis, indicating that SAT leads to destruction, dysfunction, and fibrosis in follicular cells. Thyroid hormones (FT3 and FT4) increase in the circulation, and TSH is suppressed due to follicular destruction during the acute phase of the disease. Radioactive iodine uptake during follicular destruction is minimal or undetectable. In addition, an increased ESR (>50 mm/h), and higher CRP expression levels, are observed in laboratory tests. Anti-TPO and anti-TG remain at normal levels. In patients with Basedow-Graves’ disease and an autonomous thyroid gland, an abnormal increase in the T3 level is observed. T3 and T4 increase equally in SAT cases. 7 In the present study, the T3: T4 ratio of the 5 patients was approximately 1:3, consistent with SAT laboratory findings.
We used USG and scintigraphy (radioiodine or technetium) as the imaging modalities in our cases. Thyroid USG revealed focal or diffuse hypoechogenicity with enlarged thyroid tissue (Figure 1). On Doppler USG, blood flow in the thyroid tissue was low. In addition, low uptake (<1%-3%) was detected on scintigraphy (Figure 2). Subacute thyroiditis was diagnosed based on painful thyroid tissue upon palpation, a high ESR, negative thyroid antibodies, and a low uptake on thyroid scintigraphy. Thus, SAT was diagnosed based on clinical, laboratory, and imaging methods instead of histopathological examination of the thyroid tissue.7-10
All of our patients were female and their average age was 30.4 years. Reasons for visiting the otorhinolaryngology polyclinic included neck pain, odynophagia, and ear pain. There was no history of thyroiditis, and no evidence of the condition was revealed by examination. The T3 and T4 levels were high, the TSH level was low, and the ESR was high in all patients. In addition, all patients were anti-TPO- and anti-TG-negative (Table 1). On thyroid USG and Doppler examinations, diffuse lobular growth in the thyroid tissue, a hypoechogenic thyroid gland, and reduced blood flow were observed. On thyroid scintigraphy, low uptake was observed in the retained thyroid tissues (Figures 1 and 2).
In many cases, the use of high-dose aspirin (eg, 600 mg/4-6 h) or nonsteroidal anti-inflammatory drugs is sufficient for treating SAT. However, if these treatments prove insufficient and the pain and fever are severe, prednisolone should be given. The standard dose of prednisolone is 40 to 60 mg, but this may vary depending on the severity of the disease. 11
In our patients, aspirin (600 mg/4-6 h) was administered for 5 days because COVID-19 was in the acute phase and there was antiaggregation activity. However, prednisolone treatment (1 mg/kg) was initiated in 2 cases (and then tapered off over 10 days) due to insufficient improvement. Duan et al showed that short-term steroid therapy was shown more reliable in moderate and mild cases of SAT. Because the clinical findings of the 2 patients in our study were not severe, short-term steroid therapy was administered. 12 In both cases, clinical and laboratory findings returned to normal within an average of 31.5 days. Our patients were followed up on for an extended period in the internal disease polyclinic since an SAT recurrence rate of 20% to 30% had been reported. 13 Some researchers have noted that short-term steroid therapy increases the rate of SAT recurrence. 14 Recent data have also revealed the presence of genetic predisposing factors in SAT recurrences. Especially in patients with HLA-B18 and HLA-B35 haplotypes, the rate of SAT recurrence was found to be significantly higher. 15
Of 4 published studies, thyrotoxicosis symptoms were noted in 3 cases except for one SAT case associated with COVID-19 infection (all patients were female and ranged in age from 18 to 69 years). Subacute thyroiditis occurred between days 5 and 30 after the diagnosis of COVID-19, and the recovery period was 7 to 30 days in duration.5,16-18 Our 5 female patients ranged in age from 21 to 45 years and showed no signs of low-intensity thyrotoxicosis. The average recovery time was 25 days.
Severe acute respiratory syndrome coronavirus-2 is thought to cause SAT via a mechanism similar to that of other viral agents. In previous studies, SARS-CoV-2 showed an affinity for ACE2 receptors and caused thyroiditis, similar to lung infection (and where these receptors are also present in thyroid tissue).13,15
Thyroid dysfunction has also been observed in asymptomatic COVID-19 cases (ie, in those without respiratory system pathologies) in association with numerous mechanisms. Severe acute respiratory syndrome coronavirus-2 stimulates the immune system; this causes the release of interleukins 1 to 6 and tumor necrosis factor, leading to “cytokine storm.” In the acute phase of the cytokine storm, the serum FT3 level rapidly increases in parallel with interleukin 6, resulting in thyrotoxicosis.19-21 In some advanced cases, thyrotoxicosis may cause thromboembolic attacks, cardiac arrhythmias, and mortality.22-25 Dysregulation of the immune system, which also occurs during cytokine storm, leads to autoimmune pathologies such as phospholipid syndrome, thrombocythemia, hemolytic anemia, Guillain-Barré syndrome, and Graves’ disease, in addition to SAT. 26
The present results for asymptomatic COVID-19 patients with SAT support the hypothesis that ACE2 receptors are mostly found in patients with thyroid tissue. Isolation of SARS-CoV-2 virus in thyroid tissue and investigation of HLA-B35 and HLA-B18 antigen should be targets for future studies.
Conclusion
Severe acute respiratory syndrome coronavirus-2 affects thyroid function and may cause SAT. The main symptoms in our patients were neck pain and odynophagia. Physicians managing patients with symptomatic or asymptomatic COVID-19 infection should suspect SAT, especially in cases with swelling and pain in the lower front part of the neck. Although typical COVID-19 signs and symptoms were not observed in patients diagnosed with SAT for the first time during the COVID-19 pandemic, underlying SARS-CoV-2 infection should not be ruled out, especially since this could help prevent contagion.
Footnotes
Authors’ Note
Acknowledgments
The authors thank the chief physician of Bahat Hospital, Dr. Hamza Bahat, as well as Yeni Yuzyil University and the Department of ENT of Istanbul University.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.