
Abstract
Objectives:
Holmium: YAG laser has gained its popularity throughout the years and is used to treat sialolithiasis, which helps to overcome the limitations of traditional sialendoscopic lithotripsy for larger-sized salivary stones. However, little information is available regarding factors predicting the success rate of Holmium: YAG laser intraductal lithotripsy. The purpose of this study is to investigate the factors affecting the success rates of Holmium: YAG laser lithotripsy for salivary stones treatment in a tertiary care hospital.
Methods:
A retrospective study conducted in patients receiving sialolithiasis surgery under sialendoscopy from May 2013 to March 2015 at Mackay Memorial Hospital, Taiwan. Data on various factors, including patients’ age, gender, glands, size of largest stone, multiple stones (≥2 stones), location of the stone (distal duct, middle duct, proximal duct, and hilum), and operative time. The success of the surgery defined as patients without any complaints such as swelling or tenderness. Logistic regression and Fisher exact tests were employed to examine these factors on the success rate.
Results:
Fifty-four patients who received sialendoscopy surgery with a mean age of 35.74 years old recruited. Logistic regression identified the operation time exceeding 210 minutes showed 23.497 folds higher odd ratio of having a result of operation failure (P < .05).
Conclusion:
The prolonged operation time is the sole independent factor affecting the successful outcome for salivary gland intraductal laser lithotripsy. We recommend operative time be no more than 210 minutes to increase the success rate in salivary gland Holmium: YAG laser intraductal lithotripsy.
Introduction
Sialolithiasis represents about 66% cause of obstructive sialadenitis, 1 which accounts for half of benign salivary gland disease. 2 The calcified structures usually lead to the mechanical obstruction of the salivary duct and subsequently result in an increased risk of bacterial infections or the development of mucoceles. 3 As initial conservative treatment fails, refractory cases may require surgery ranging from papillotomy to complete gland extirpation. Within the past 2 decades, the minimal-invasive sialendoscopically assisted lithotripsy has gained popularity. 4 The high water absorption and shallow penetration depth characteristics of Holmium: YAG laser has made the endoscopic laser lithotripsy a routine procedure in fragmenting the urinary stones. 5,6 Holmium: YAG laser has also been used to treat sialolithiasis, making it possible to overcome the limitations of traditional sialendoscopic lithotripsy for larger-sized salivary stones. 7 -9 From the experiences of treating ureteral stones, in a retrospective study including 105 patients, surgeon experience is the only factor predictive of complications and success for ureteroscopic holmium laser lithotripsy. 10 Another retrospective research in assessing the prognosis of Holmium: YAG laser lithotripsy for ureteral stones in 70 preschool children found the stone size and location were associated with success rates, while the stone location and operative times were the factors affecting the complication rates. 11 However, little information is available on factors predicting the success rate of salivary endoscopic laser lithotripsy.
The aim of the study is to investigate the factors affecting the success rates of Holmium: YAG laser sialendoscopic lithotripsy in the management of salivary stones in 54 Asian patients from a tertiary care hospital.
Methods
This retrospective study was conducted at the Department of Otolaryngology, MacKay Memorial Hospital, Taipei, Taiwan. The protocol was approved by the institutional review board at MacKay Memorial Hospital (14MMHIS082). Data from patients receiving surgery for sialolithiasis under sialendoscopy from May 2013 to March 2015 at Mackay Memorial Hospital were collected and analyzed, and informed consent was obtained. After excluding missing data, such as failures to return for follow-up, 54 participants diagnosed with sialolithiasis receiving sialendoscopic surgery assisted with Holmium: YAG laser (VersaPulse PowerSuite P20, Lumenis) were included. All the surgeries were conducted under sialendoscope with an outer diameter of 1.3 mm and a working channel of 1.15 mm (11577KE model, Karl Storz), through which the laser fiber could pass, were used. All surgical procedures were performed by the same surgeon at the Mackay Memorial Hospital.
We assessed logistic regression analysis to investigate whether these 7 covariates would affect the result or not, such as patients’ age, gender, glands, size of largest stone, multiple stones, location of the stone, and operative time.
We collected age and gender status based on patients’ personal information. Glands were divided into parotid gland groups and submandibular glands group. If stones number over than 2, then we defined as multiple. The location of stones grouped them as distal duct (papilla), middle duct, proximal duct, and hilum (post-hilar duct system). After the surgery, if the patient had any complaints such as swelling or tenderness, then we defined the surgery is failed.
We adopt SAS Statistics version 9.4. We performed Fisher exact test to evaluate categorical variable and logistic regression analysis to evaluate the continuous variable. We obtain a P value <.05 to be considered as a statistically significant difference.
Results
OVERALL Success Rate
Among 54 patients enrolled in this study, 3 patients was unsuccessfully managed by the definition of failure as persistence of symptoms. By this definition, the overall success rate is 94%. Of the 3 failure cases, all of them were found to have residue stone and symptoms. There were no clinical significant complications including postoperative stenosis with clinical relevance, rupture of the duct with salivary fistula, and abscess documented.
Age and Success Rate
Fifty-four patients who received sialendoscopy surgery aged from 14 to 71 years old (Figure 1). The average age of the patients is 35.74 years old. The ratio of men and women is 1:1.57. After conducting a logistic regression analysis, there are no significant differences between age and the success rate (P = .58).
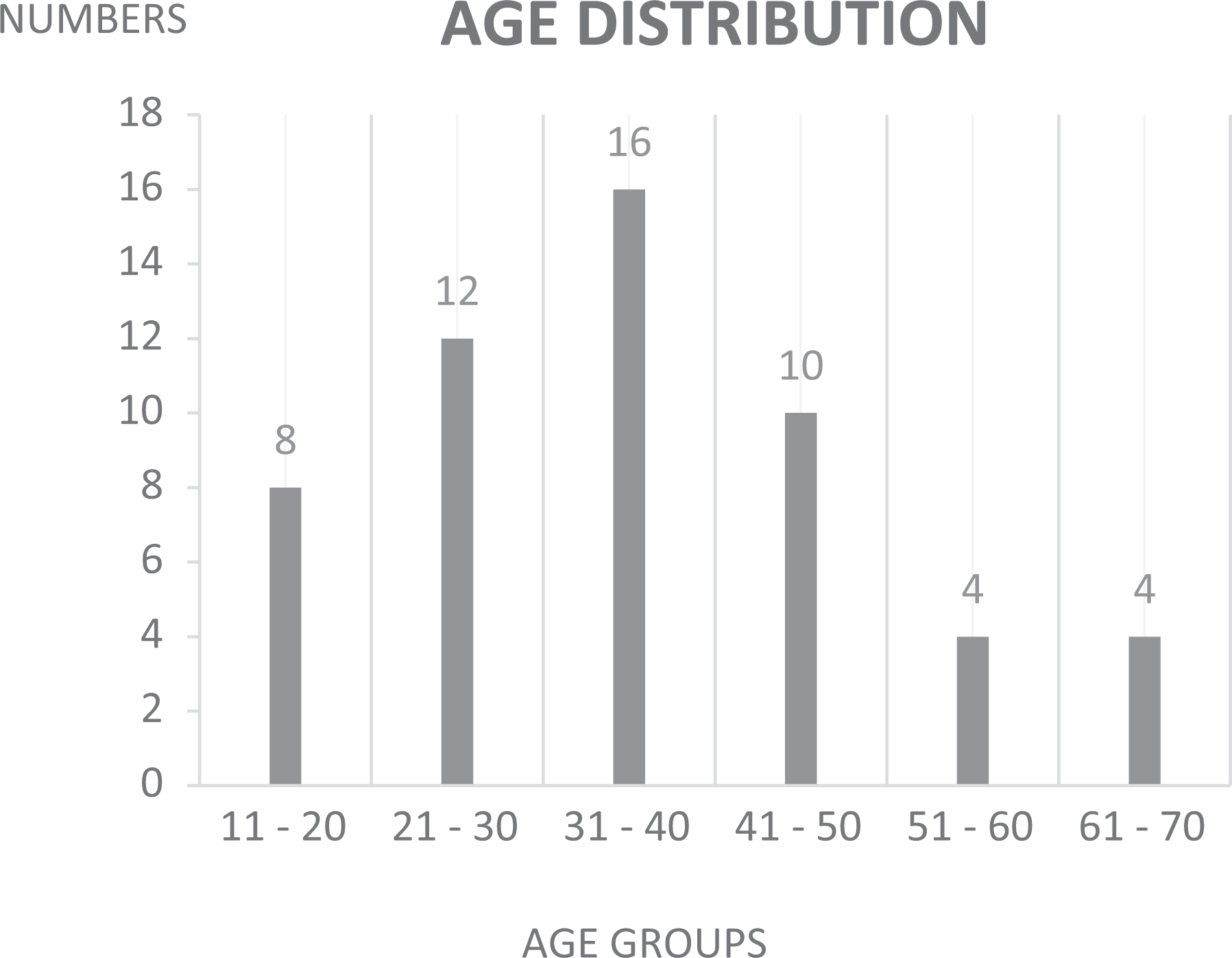
The age distribution of the cases.
Size and Success Rate
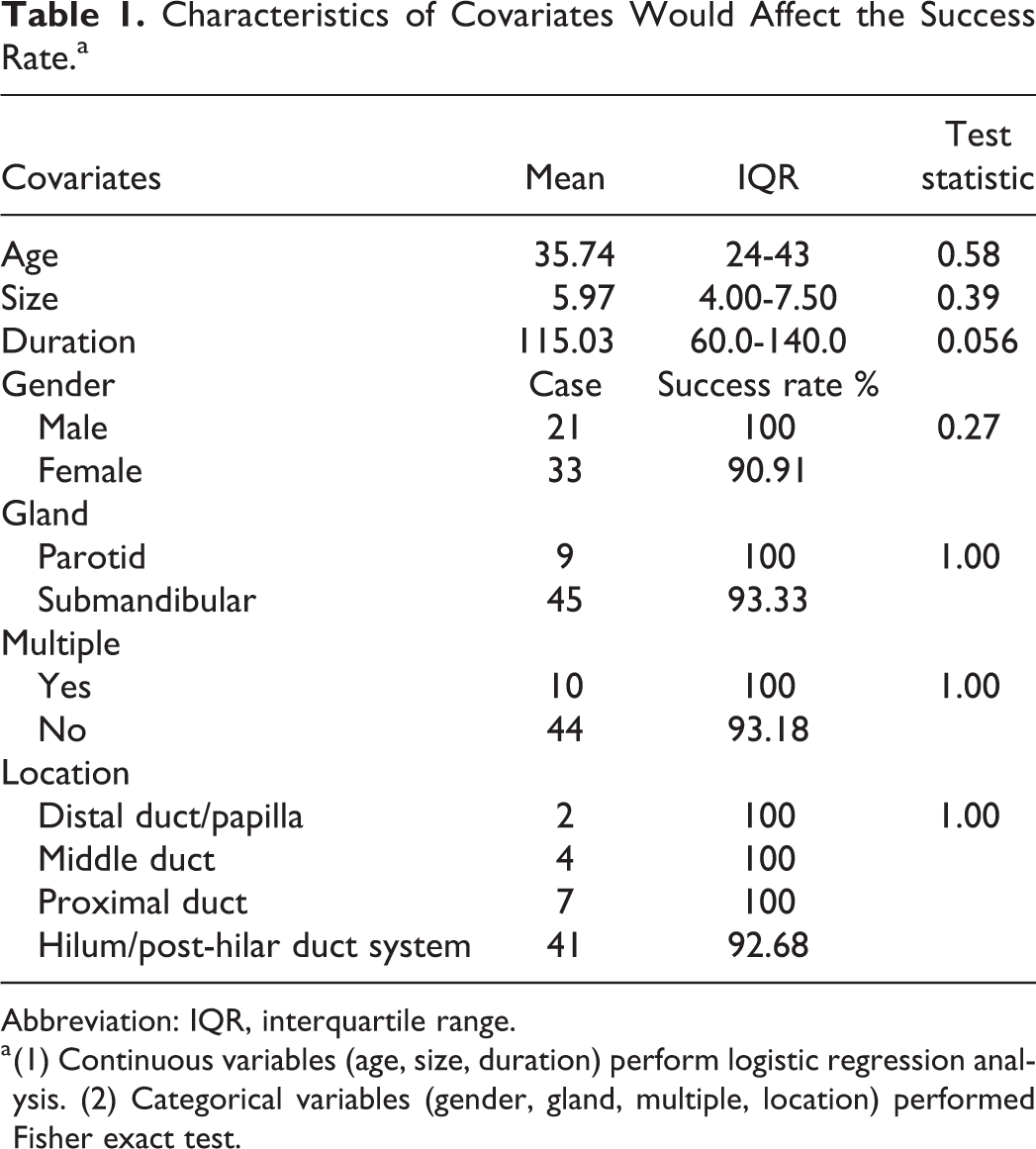
The mean size of stones is 5.97 mm (interquartile range = 4.00-7.50 mm; Table 1). After conducting a logistic regression analysis, there are no significant differences between the size and the success rate (P = .58).
Characteristics of Covariates Would Affect the Success Rate.a
Abbreviation: IQR, interquartile range.
a (1) Continuous variables (age, size, duration) perform logistic regression analysis. (2) Categorical variables (gender, gland, multiple, location) performed Fisher exact test.
Duration and Success Rate
The average duration is 115.03 minutes (Table 1). For the failure group, the average duration is 204 minutes, but regarding the successful group, the average duration is down to 110 minutes, which is almost half of the operative time. The logistic regression in evaluation operation duration as a prognostic factor for the successful rate revealed a borderline significant P value of .056, implying that the longer duration of surgery, the higher risk of failure. In further analysis as shown in Table 2, we took 30 minutes as an interval and found that when the operation time exceeds 210 minutes, the risk of failure became higher. Logistic regression shows that if the operation time exceeds 210 minutes, compared to those within 210 minutes, the odds ratio of having an operation failure is 23.497 (P = .0177).
The Odds Ratio of Operative Time.
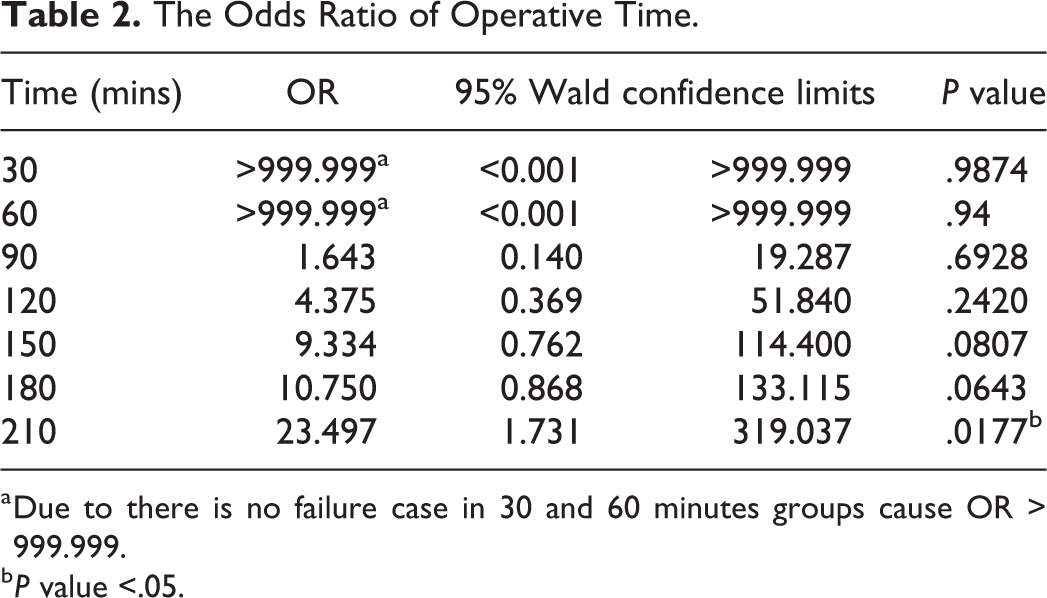
a Due to there is no failure case in 30 and 60 minutes groups cause OR > 999.999.
b P value <.05.
Gender and Success Rate
In this study (Table 1), we recruited 21 males (no failure case) and 33 females (failure cases = 3). Although in male group, all cases are successful, but the success rate in female group is also up to 90.9%. Fisher exact test was performed and showed that there is no difference in success rate between male and female (P = .27).
Gland and Success Rate
Nine patients had parotid stones, and 45 patients had submandibular stones, there were no significant differences between parotid gland and submandibular gland (P = 1.00).
Presence of Multiple Stones and Success Rate
In this study, 10 patients had multiple, and 44 patients had single stones. Fisher exact test showed no significant differences between multiple and single (P = 1.0).
Location and Success Rate
Most of the stones (75.93%) were located at the hilum (post-hilar duct system). Although stones at distal duct (papilla), middle duct, and proximal duct had a 100% successful rate, the hilum stones still had a 92.68% successful rate. The Fisher exact test showed no significant differences between location (P = 1.0).
Discussion
In this study, we have found that prolonged operation time is the sole independent factor affecting the successful outcome for salivary gland intraductal laser lithotripsy. The result from our study provides reference information which might help clinicians decide whether or not a more aggressive preventive managements, such as postoperative intraductal steroid irrigations, should be taken immediately and after once intraductal laser lithotripsy was completed.
The history of endoscopic laser lithotripsy for the salivary gland can be traced back decades ago when Gundlach et al reported the first application of endoscopic laser lithotripsy in the early ‘90s, which the salivary gland stones were successfully fragmented by the application of the Laser. 12 Since their early success, intraductal laser lithotripsy has become more popular in the management of salivary gland stones.
It is reported that salivary gland laser lithotripsy with Holmium: YAG Laser yields the most favorable success rates around 81% to 100% and thus became the standard of this procedure. 7 -9,13 Nevertheless, what about other factors affecting the outcome of laser lithotripsy? Durbec et al found the failure of laser fragmentation usually occurs in the invisible stones in stenotic or tortuous ducts. 14 Martellucci et al reports one case that had postoperational stenosis 3 months later and ascribes this stenosis to possible laser thermal damage or contact trauma by the stone. 13 Phillips and Withrow point out that stones located at the bend of the submandibular duct at the mylohyoid muscle may be the limiting factor for successful intraductal lithotripy. 8 Sionis et al report the only one failure case of laser lithotripsy was due to large stone size (15 mm) and subsequently excessive length of the procedure. 7
More recently, Ryan et al reported their experiences in the 1-year symptom outcomes after sialendoscopy-assisted salivary duct surgery. They found in patients with sialolithiasis, nonreachable parenchymal sialoliths, and concurrent inflammatory disease and/or stenosis may be the potential risk factors for symptom persistence. 15 Moreover, in patients with chronic obstructive sialadenitis without sialolithiasis, autoimmune sialadenitis, and glands with proximal or multifocal stenoses present with the highest proportion of persistent or recurrent disease. 16 The result from these studies implies that the location of the stone, size of the stone, and the presence of stenosis seem to be essential factors predicting outcomes for intraductal laser lithotripsy.
Interestingly, the result in our study reveals an entirely different result in which prolonged operation time appears to be the sole independent factor affecting the successful outcome for salivary gland intraductal laser lithotripsy. Although it is reported that the time required for sialendoscopic laser lithotripsy directly correlates with stone size, this phenomenon is not shown in our study. 8 It is possible that, as the laser device setting and efficiency improve, the percentage for the time spent during laser lithotripsy compare to total operation time might gradually decrease, making the stone size no longer the primary determining factor for the total operation time. This speculation is also supported by the result that the mean operation time in our study is 115 minutes, shorter than the average case time of 142 minutes in their series.
Several studies have been published reporting the effectiveness of different laser systems in disintegrating salivary stones through intraductal sialendoscopy with positive outcomes. 7 -9,12 -14,17,18 The Holmium laser poses a photomechanical effect to create a shock wave on the stone, along with a photothermic effect on the stone surface as the major contributing factors for stone fragmentation. Although Luers et al have demonstrated that during lithotripsy in an in vitro setup, the temperature around the laser fiber tip reduces by about 50% under continuous rinsing, 19 there is still the possibility that the energy might accumulate locoregionally in such a narrow salivary duct in vivo and predispose thermal injury under prolonged operation. 4,14,19,20 Besides, only 60% of the shock waves actually penetrate the stone, whereas about 40% is reflected from its surface and may cause thermal events. 21 Furthermore, strong continuous irrigation may increase the tendency of developing edema of the mouth floor and the gland tissue, 4,14 and repeated endoscopic passage with inflammatory content raise the chance of papillary stenosis and ductal perforation. 14 Apart from the above factors, the settings of the laser energy may contribute to the prolonged operation time. Schrotzlmair et al have presented in an in vitro study that holmium laser with low energy as 500 mJ per pulse is capable of fragmenting salivary stones, whereas increase in the laser energy up to 1.5 J per pulse does not lead to significantly more ablation; instead, the possible accompanying repulsion effect may decrease the efficacy of lithotripsy. 22 Aldoukhi et al compared the different settings of holmium laser systems for ureteroscopy and concluded that the settings using higher frequency with lower pulse energy are capable of not only disintegrating the stone into submillimeter fragments, so-called “Dusting” technique, but also reduce the procedure time. 6 Further studies comparing different holmium laser settings in salivary lithotripsy are warranted for reducing operation time and thus reaching higher success rates. More recently, Prof Koch et al reported the new Calculase II Ho: YAG laser for intraductal lithotripsy in sialolithiasis. 23 Although the authors concluded that the laser presetting with a frequency of 3 to 6 Hz, energy level of 0.5 to 1.2 J, and effective power of between 3 and 4.8 W is sufficient to achieve maximum success without any increased risk for complications, the study also reveals that the efficiency of the new Ho: YAG laser appears to be much higher compared to the traditional VersaPulse PowerSuite Ho: YAG laser, which potentially decreases the procedure time along with the risk of complications.
The limitations of our study include its retrospective nature, relatively small patient cohort, especially in the parotid group, and the lack of much of the patients’ clinical data. The location of the stone is mainly at the hilum/post-hilar ductal system. Nonetheless, all the operations were done by one surgeon utilizing the same holmium: YAG laser system and laser fiber tip with equal diameter. The average stone size, mean operation time, and success rate were comparable with other studies, 7,8,13 and we identified the prolonged operation time as the only independent factor affecting the successful outcome for salivary gland intraductal laser lithotripsy, with the cutoff point as 210 minutes.
Although it seems that efficient laser equipment with the optimal settings was crucial regarding the success rate of the lithotripsy, perhaps, the physician’s individual experience is the most important factor leading to better effectiveness and fewer side effects for the patient. Instead of using this 210 minutes operation time as an operation time limit, which is in many ways not practical, we believe is that this time of fewer than 210 minutes could serve as a “limit” or “ceiling” for institutions to take it as a reference, especially in their early phase of the learning curve, if the sialendoscopic practice is to be developed or established. For sialendoscopic procedures that are close to reaching this time benchmark, perhaps the senior surgeon or consultant should take over the procedure or even consider the procedure to be stopped if possible. Although large, multicenter trials are needed to identify other factors relating to the complication and successful outcome, physicians might be recommended to consider the result of our study and try not to carry the lithotripsy procedure for a too long time a prolonged operative time of more than 210 minutes. The time addressed in this study to be regarded as a reference time “limit” as an overall consequence of various factors, including stone size, disease severity, instrumentation, surgical skills, and so on, is significantly associated with operation failure.
In conclusion, the prolonged operation time is the sole independent factor affecting the successful outcome for salivary gland intraductal laser lithotripsy. Operative time of more than 210 minutes is significantly associated with operation failure in salivary gland Holmium: YAG laser intraductal lithotripsy.
Supplemental Material
Supplemental Material, sj-docx-1-ear-10.1177_01455613211010075 - Prognostic Factors for the Outcome of Salivary Gland Holmium: YAG Laser Intraductal Lithotripsy
Supplemental Material, sj-docx-1-ear-10.1177_01455613211010075 for Prognostic Factors for the Outcome of Salivary Gland Holmium: YAG Laser Intraductal Lithotripsy by Shuo-Jen Wang, Lung-Che Chen, Yi-Chih Lin, Yen-Chun Chen, Luong Huu Dang, Po-Yueh Chen, Chin-Hui Su and Shih-Han Hung in Ear, Nose & Throat Journal
Footnotes
Authors’ Note
S-.J.W. and L-.C.C. contributed equally to this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is supported by the Taipei Medical University Research Grant 106TMUH-NE-01.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.