
Abstract
Objectives:
To investigate the correlation between clinical features and endolymphatic hydrops (EH) in children with sudden sensorineural hearing loss (SSNHL).
Methods:
We collected 30 SSNHL children aged ≤17 years old, all of whom underwent intravenous gadolinium injection. After 4 hours, inner ear 3-dimensional inversion recovery sequence with real reconstruction (3D-real IR) magnetic resonance imaging was performed. Combined with their medical history such as gender, age, disease course, hearing loss, and so on, the results were analyzed.
Results:
Different degrees of EH were shown in the vestibule or different turns of cochlea in the affected ears of SSNHL children, and 12 (40%) of 30 children showed positive EH. Age, low and middle frequency hearing loss, and other clinical symptoms such as dizziness and ear fullness have been shown to be related to a certain degree of EH in vestibule or cochlea, whereas no relationship was found between EH and other clinical features such as high-frequency hearing loss, gender, affected side, and tinnitus.
Conclusions:
Endolymphatic hydrops may not reflect the trend of disease progression over time in children with SSNHL, but the age of onset may be an important factor in the presence or absence of EH. Endolymphatic hydrops may be one of the causes of dizziness and ear fullness but has no obvious connection with the occurrence of tinnitus. Older SSNHL children with dizziness and ear fullness should maintain long-term follow-up to dynamically monitor the changes in EH.
Introduction
Sudden sensorineural hearing loss (SSNHL) is a familiar inner ear disease, which is defined as rapidly developing hearing loss within less than 3 days, and the level of the hearing loss is more than 30 decibels in at least 3 consecutive frequencies. 1 In addition to hearing loss, SSNHL patients may have other symptoms such as tinnitus, dizziness, ear fullness, earache, and so on. A large number of SSNHL cases (96%-99%) occur unilaterally, 2 and its pathogenesis is still not very clear. There are some reports claiming that it may be related to virus infection, 3 autoimmune response,4,5 and the distribution of cochlear fluid. 6 Therefore, magnetic resonance imaging (MRI) with intravenous gadolinium injection is often applied clinically to evaluate endolymphatic hydrops (EH) in the inner ear of SSNHL patients. Sudden sensorineural hearing loss is common in 25 to 60 years old patients (the peak age is 46-49 years), 7 and the children cases are very rare. According to statistics, the incidence of SSNHL was 27 per 100 000 in America 8 and 20 per 100 000 in Germany. 9 The incidence of SSNHL in children (<18 years old) was only 1 per 100 000, accounting for about 6.6% of all SSNHL patients. 10 Due to the rare cases of SSNHL in children, knowledge about the relationship between its clinical symptoms and EH is limited. Therefore, we designed this study to accumulate cases of children with SSNHL in the past 3 years and collected their clinical history such as age, course of disease (the interval between the first onset of the disease and magnetic resonance inner ear imaging), hearing loss, dizziness, tinnitus, ear fullness, and so on. Each SSNHL child in our study underwent the MRI scan. The objective of this study was to explore the relationship between different degrees of EH evaluated using MRI with 3D-real IR sequence after intravenous gadolinium injection and various clinical features.
Methods
Patients
From January 2017 to June 2020, 30 SSNHL children (25 unilateral affected ears and 5 bilateral affected ears, totaling 35 ears) who underwent magnetic resonance (MR) scans via intravenous gadolinium injection of the inner ear at the Eye, Ear, Nose, and Throat (EENT) Hospital of Fudan University were collected in this research, including 12 males and 18 females, with an average age of 14.03 years (10-17 years). Some clinical features such as age, gender, affected side, course of disease, hearing loss, and other symptoms such as vertigo, tinnitus, and aural fullness were investigated (Table 1). The diagnostic standard of SSNHL was subjected to the AAO-HNS (American Academy of Otolaryngology-Head and Neck Surgery) guidelines 1 : A rapid-onset subjective sensation of sensorineural hearing loss (not less than 30 decibels), affecting at least 3 consecutive frequencies within a 72-hour window for the diagnosis of SSNHL. The medical ethics committee of the EENT Hospital of Fudan University had approved this research, and the informed consents of all patients in our group were acquired.
Patients’ Characteristics and Degrees of Endolymphatic Hydrops (EH).a
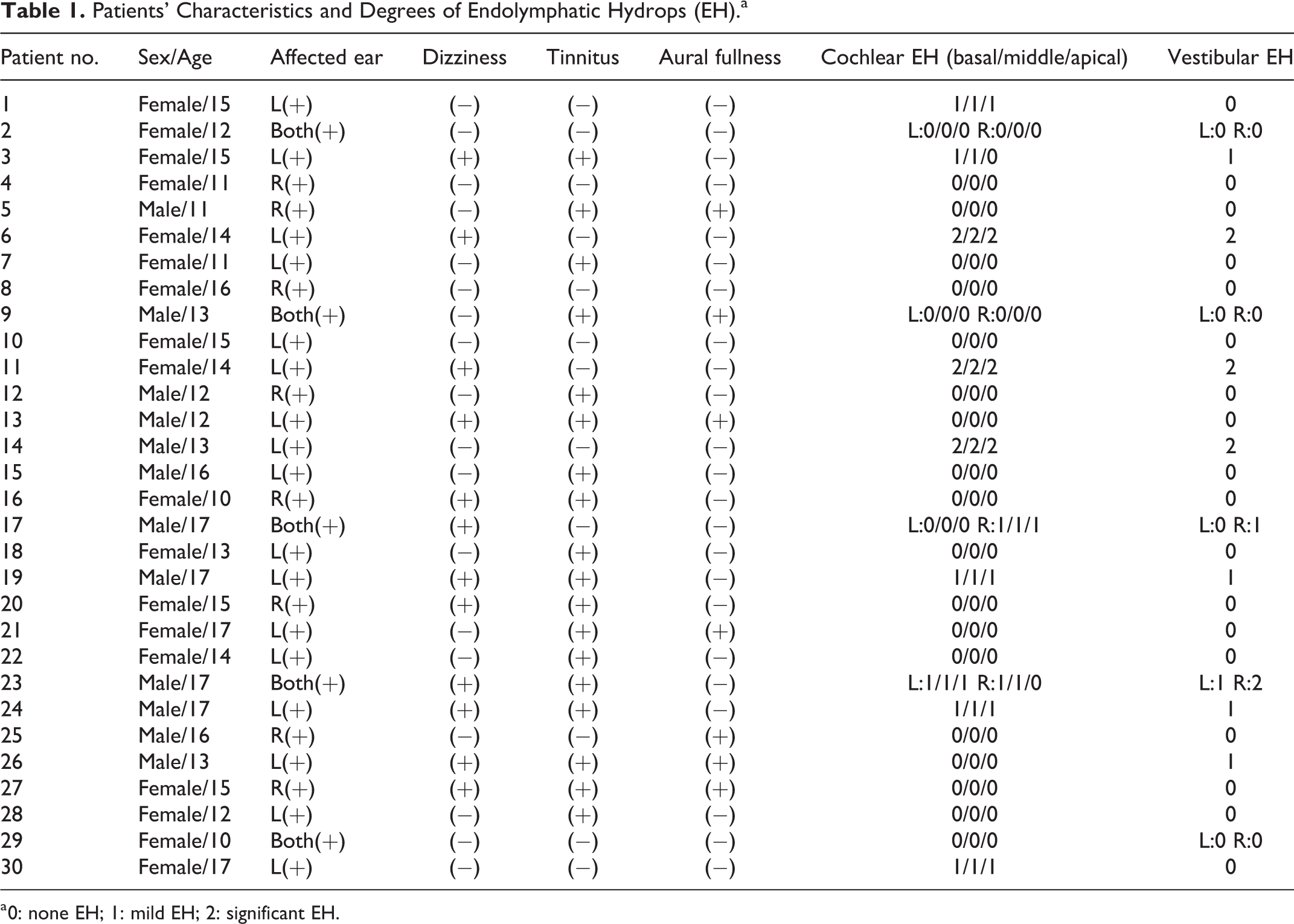
a 0: none EH; 1: mild EH; 2: significant EH.
Pure Tone Audiometry
Pure tone audiometry thresholds at all conventional frequencies (125-8000 Hz) were tested by applying a GSI 61 audiometer (Grason-Stadler). Furthermore, the frequency bands at the low (0.125-0.25 kHz), middle (0.5-2 kHz), and high (4-8 kHz) frequencies were appraised. All SSNHL children’s affected ears showed varying extents of SSNHL and the mean values at low, middle, and high frequency brands were 56.46 ± 14.59 dB (28-86 dB), 54.69 ± 12.46 dB (35-90 dB), and 60.49 ± 18.01 dB (32-105 dB), respectively. The specific distribution can be seen in Figure 1.
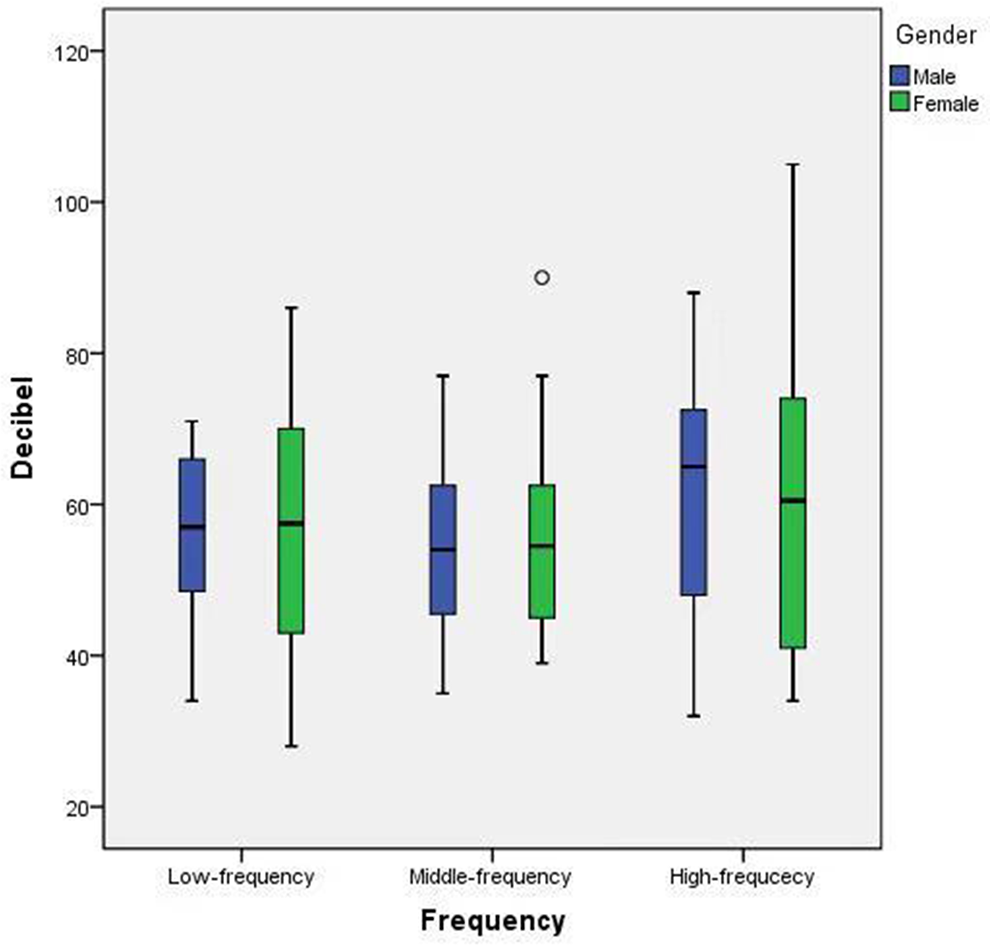
The specific distribution of low, middle, and high frequencies hearing loss in children with sudden sensorineural hearing loss.
Image Acquisition
All SSNHL children accepted intravenous gadolinium injection with the double dose (0.4 mL/kg body weight) of gadolinium (Magnevist, Bayer Healthcare). The dose we use was the double dose because satisfying images could not be achieved by applying 3D-real IR sequence with a conventional dose (0.2 mL/kg body weight). The ethics committee and patients were consentaneous with the adhibition of the double dose of gadolinium. Magnetic resonance scans were applied to all patients after 4 hours. All scans were carried out by a 3T MRI scanner (Magnetom Verio, Siemens Healthineers) with a 4-channel phased array coil. T2 SPACE (sampling perfection with application-optimized contrasts by using different flip angle evolutions) and 3D-real IR sequences were used in capturing images. The parameters of T2 SPACE sequence included slice thickness (0.6 mm), repetition time (1000 ms), echo time (132 ms), flip angle (120°), matrix (384 × 384), field of view (200 × 100 mm2), and scan time (2 minutes and 44 seconds). The parameters of 3D-real IR sequence included: slice thickness (0.6 mm), repetition time (6000 ms), echo time (181 ms), inversion time (1850 ms), flip angle (180°), matrix size (768 × 768), field of view (160 × 100 mm), and scan time (15 minutes and 20 seconds).
Endolymphatic Hydrops Evaluation
The collected 3-dimensional images are reconstructed with maximum intensity projection and multifaceted reconstruction using the JUSHA workstation (Nanjing JUSHA Commercial & Trading Co.,LTD.). Gadolinium contrast agent flows into the space of the perilymph in the inner ear via the circulatory system, making the perilymph space appear as a high signal in the image, and there is a barrier in the inner and outer lymph, which prevents the contrast agent from entering the labyrinth, so the endolymph space shows a low signal, which can be used to distinguish the inner and outer lymphatic spaces. According to the anatomical structure of the cochlea, the corresponding parts of the cross-section of the cochlea were identified as the basal turn, the middle turn, and the apical turn in MR images. In this study, the EH evaluation used the scoring method by Nakashima et al 11 for the diagnosis of EH (Table 2). According to the results of measurement and judgment, we further used “0, 1, 2” to represent “none EH, mild EH, significant EH,” respectively, for evaluation of EH degree in the cochlea and vestibule. According to the double-blind principle and the method described in Table 1, in this experiment, 2 radiologists with 10 and 12 years of practicing experience, respectively, in the diagnosis of inner ear diseases independently read and evaluated the images. For the different parts, the final results depended on their consensus.
The Evaluation Criteria for Endolymphatic Hydrops (EH) After Intravenous Gadolinium Injection.
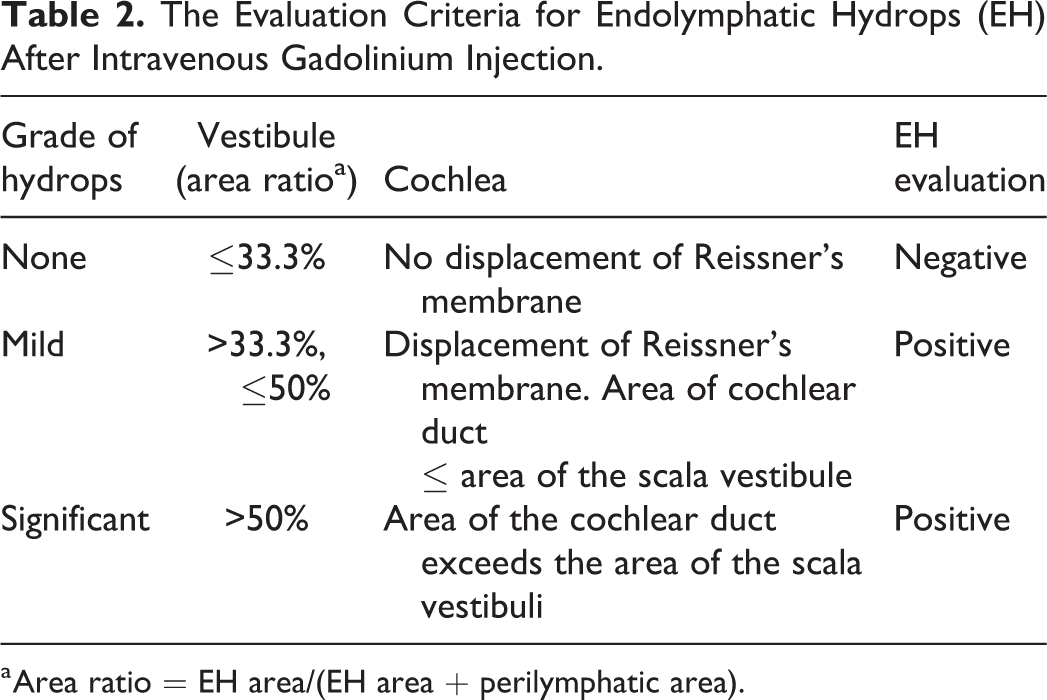
a Area ratio = EH area/(EH area + perilymphatic area).
Statistical Analyses
We used IBM SPSS (v.22; IBM, Armonk, NY) to calculate all statistical data. The Spearman’s test and Mann-Whitney U test were applied to explore the correlation between EH in the vestibule or different turns of cochlea and various clinical features. And p-value < 0.05 was considered statistically significant.
Results
After 4 hours of intravenous gadolinium injection, the EH condition of the cochlea and vestibule in all SSNHL children was observed. 3D-real IR MRI was applied to evaluate the extent of EH in the cochlea and vestibule of the affected ears. Figures 2 and 3 showed the conditions of vestibular and cochlear EH of different SSNHL children. Figure 4 showed the concrete number of diverse extents of EH in the vestibule and different turns of cochlea. Among all affected ears of SSNHL children, 10 vestibules showed positive EH (6 cases of mild EH and 4 cases of significant EH), and 12 cochleae showed positive EH of different turns. Nine children had both mild and severe vestibular and cochlear EH. One child showed mild vestibular EH without cochlear EH. Two children had cochlear EH in all turns without vestibular EH. Unexpectedly, mild and severe vestibular and cochlear EH were found in the contralateral asymptomatic ears of 2 children with unilateral severe vestibular and cochlear EH, respectively. Figure 5 showed the bilateral inner ear MRI of 1 of 2 cases, the image indicated that the asymptomatic ear opposite to the left affected ear of this SSNHL child also had significant vestibular and cochlear EH. Among all children, the ratio of the acreage of the low signal area of the vestibular to the total vestibular area ranged from 13.3% to 63.9% (mean value: 28.9%). Besides, a 13-year-old case without vestibular or cochlear EH had a positive family history. Both his mother and grandmother had the same symptoms at a similar age.

A 14-year-old female patient with unilateral (left) sudden sensorineural hearing loss, with the disease course of 10 days and the symptom of dizziness but no tinnitus and ear fullness, underwent magnetic resonance scan with gadolinium. The black arrow shows that there is mild endolymphatic hydrops in the cochlea. The low signal area marked by the black dashed line is the vestibular endolymphatic area, and the area marked by the black solid line is the total area of perilymph and endolymph, the ratio of the 2 areas is 47.3%, which means a mild endolymphatic hydrops exists in the vestibule.
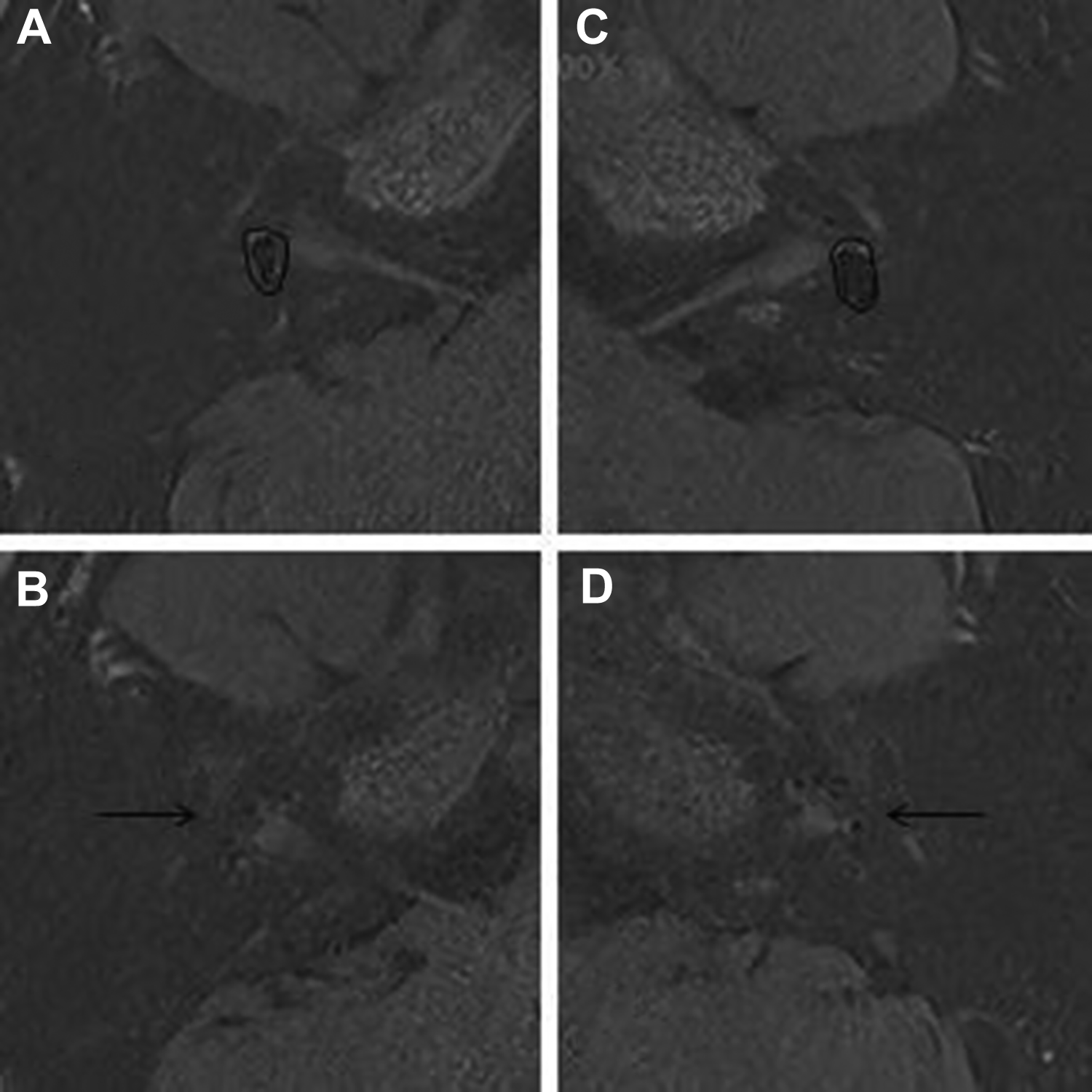
A 17-year-old male patient with bilateral sudden sensorineural hearing loss, with the disease course of 1 month and the symptom of tinnitus but no dizziness and ear fullness, underwent magnetic resonance scan with gadolinium. (A) The low signal area marked by the black dashed line is the vestibular endolymphatic area, and the area marked by the black solid line is the total area of perilymph and endolymph, the ratio of the 2 areas is 42.1%, which means a mild endolymphatic hydrops exists in the vestibule of the right affected ear. (B) The black arrow shows that there is mild endolymphatic hydrops in the cochlea of the right affected ear. (C) The low signal area marked by the black dashed line is the vestibular endolymphatic area, and the area marked by the black solid line is the total area of perilymph and endolymph, the ratio of the 2 areas is 37.7%, which means a mild endolymphatic hydrops exists in the vestibule of the left affected ear. (D) The black arrow shows that there is mild endolymphatic hydrops in the cochlea of the left affected ear.
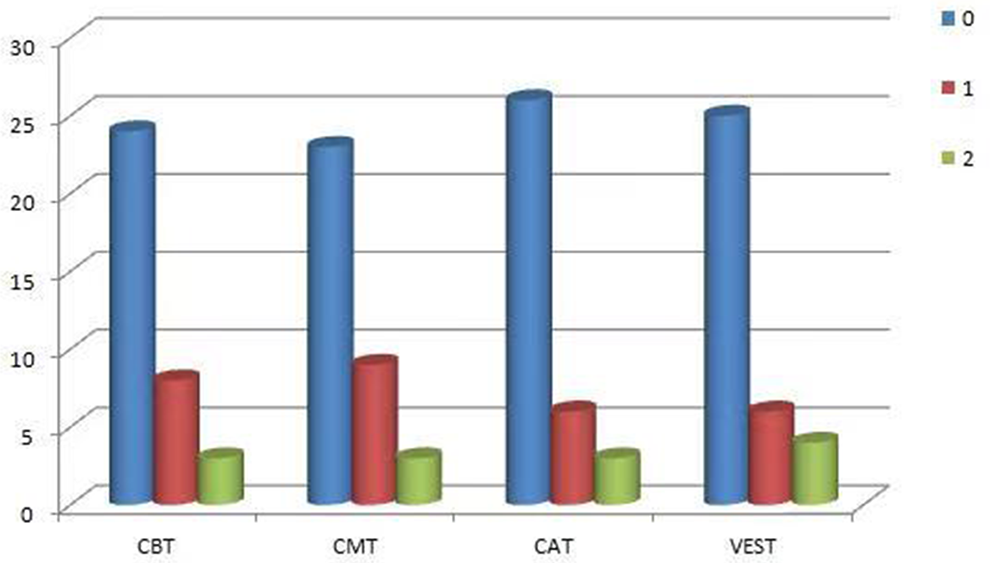
Endolymphatic hydrops sorted as (0), mild (1) and significant (2) ranging in the cochlea and vestibule of affected ears. The ordinate represents the number of affected ears with endolymphatic hydrops in the corresponding part of the cochlea and vestibule. CAT indicates cochlear apical turn; CBT, cochlear basal turn; CMT, cochlear middle turn; VEST, vestibule.
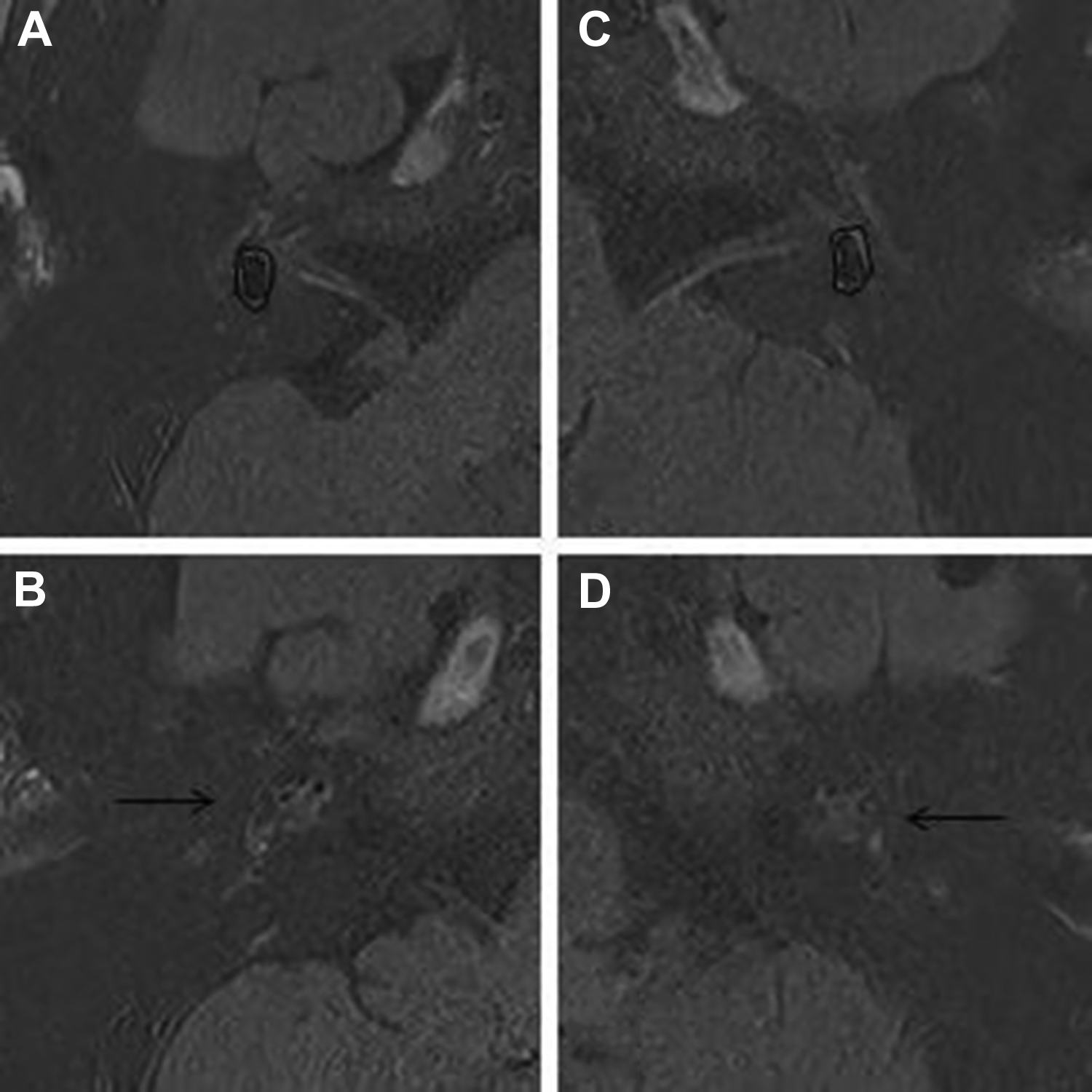
A 13-year-old male patient with unilateral (left) sudden sensorineural hearing loss, with the disease course of 7 days and no any symptoms such as dizziness, tinnitus, and ear fullness, underwent magnetic resonance scan with gadolinium. The contralateral asymptomatic (right) ear of left affected ear also has endolymphatic hydrops. (A) The low signal area marked by the black dashed line is the vestibular endolymphatic area, and the area marked by the black solid line is the total area of perilymph and endolymph, the ratio of the 2 areas is 35.9%, which means a mild endolymphatic hydrops exists in the vestibule of the right affected ear. (B) The black arrow shows that there is mild endolymphatic hydrops in the cochlea of the right affected ear. (C) The low signal area marked by the black dashed line is the vestibular endolymphatic area, and the area marked by the black solid line is the total area of perilymph and endolymph, the ratio of the 2 areas is 58.3%, which means a significant endolymphatic hydrops exists in the vestibule of the left affected ear. (D) The black arrow shows that there is significant endolymphatic hydrops in the cochlea of the left affected ear.
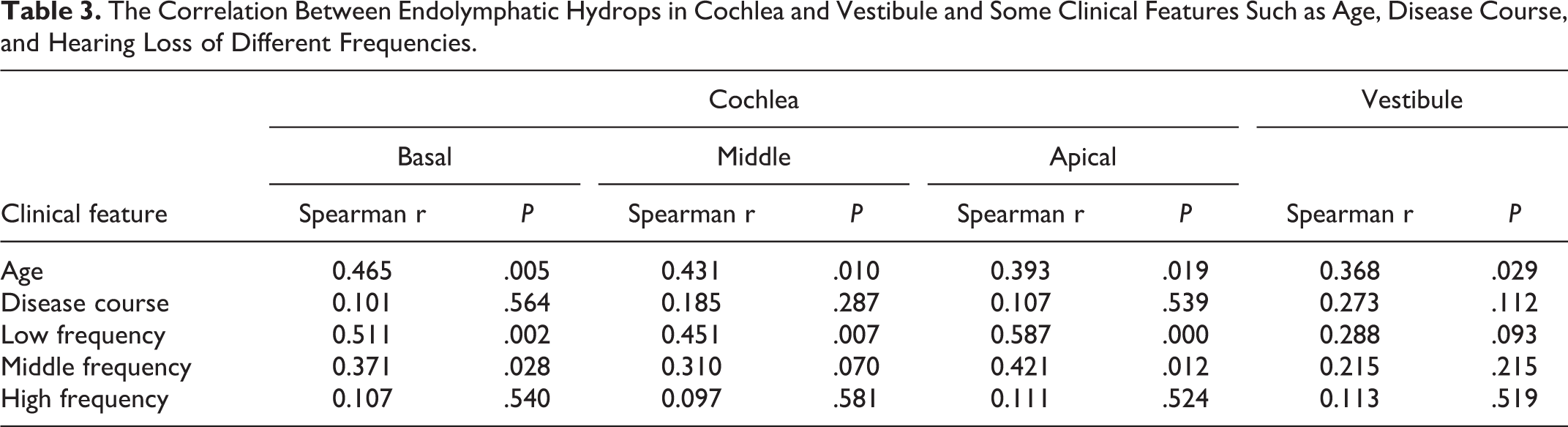
The Spearman test reflected a meaningful connection between the age of the child and the degree of EH of the vestibule and cochlea (all P < .05), but no connection was found between the course of disease and the presence of EH in the vestibule and cochlea. Hearing loss of low frequency was related to the EH of all turns in the cochlea (all P < .05), hearing loss of middle frequency was only related to the EH of basal and apical turns in the cochlear (P = .028 and .012, respectively), and hearing loss of high frequency was not related to the EH of all turns in the cochlea (all P > .05). Regarding the vestibular EH, low- or medium- or high-frequency hearing loss was not associated with vestibular EH (all P > .05). See Table 3 for specific data.
The Correlation Between Endolymphatic Hydrops in Cochlea and Vestibule and Some Clinical Features Such as Age, Disease Course, and Hearing Loss of Different Frequencies.
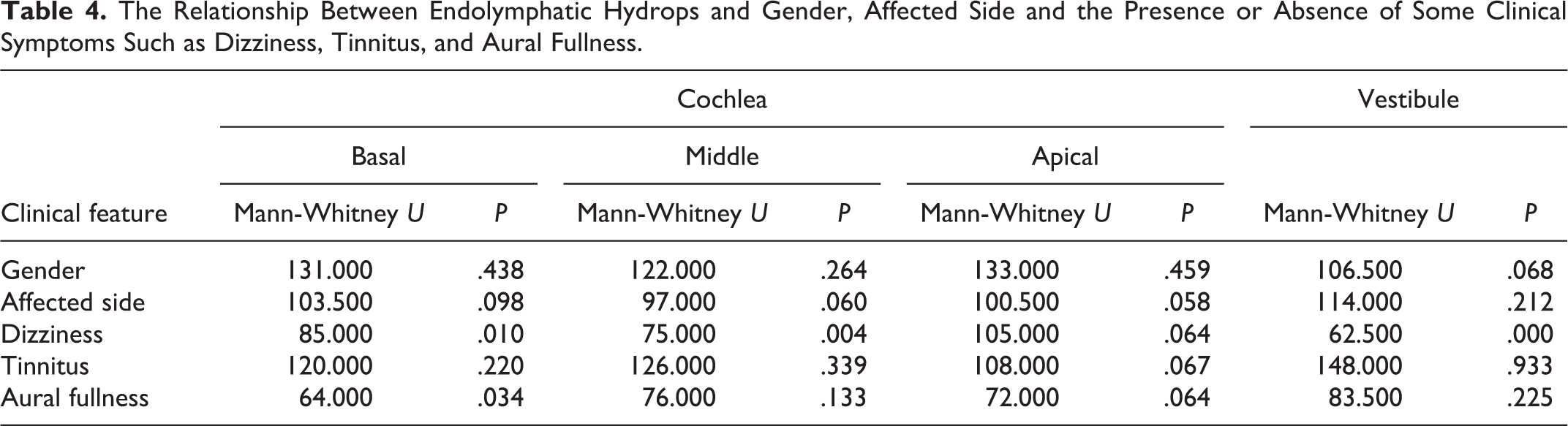
The Mann-Whitney U test reflected a significant connection between the existence or nonexistence of dizziness and the EH in the vestibule and cochlea (basal or middle turn; P < .05). Meanwhile, there was a certain correlation between the existence or nonexistence of ear fullness and the EH in basal turn of the cochlea (P = .034). Other clinical features such as gender, affected side, and tinnitus did not appear to be related to the EH in the vestibule or different turns of the cochlea (all P > .05). See Table 4 for specific data.
The Relationship Between Endolymphatic Hydrops and Gender, Affected Side and the Presence or Absence of Some Clinical Symptoms Such as Dizziness, Tinnitus, and Aural Fullness.
Discussion
Sudden sensorineural hearing loss is a common inner ear disease, whose concept was first described by De Kleyn. 12 Sudden sensorineural hearing loss is familiar in adult patients, children’s cases are very rare, which makes it difficult for us to fully understand the disease in children. The cause of SSNHL is still not very clear. Many scholars have put forward a series of conjectures such as virus infection, membrane labyrinth hydrops, nonorganic, migraine, and so on. Besides, Schieffer et al 13 reported that iron deficiency anemia may be related to children’s sensorineural hearing loss. Meanwhile, Choi et al 14 reported that air pollution may also increase the prevalence of SSNHL. The potential pathogenic factors of SSNHL in adults and children seem to be very different, which in adults often included the bad lifestyle habits (smoking, alcohol abuse, hyperlipidemia, etc) and other common diseases (anterior inferior cerebellar artery occlusion, multiple sclerosis, vestibular schwannoma, etc). Although these can also occur in children, they are very rare compared to adults. Therefore, the underlying pathogenic factor of SSNHL children is a mystery that has puzzled many scholars for a long time, and more research is still needed urgently.
At present, there are still relatively few reports about SSNHL in children, and the most direct reason is that children cases with SSNHL are relatively rare. Although there are some reports on the specific value of the incidence of SSNHL children, most scholars still remain skeptical about this due to children’s cognition and expression skills for diseases are far worse than adults and there are bound to be some potential cases that have not been detected and treated in time, which has a great negative impact on the statistics of incidence rate.
Sudden sensorineural hearing loss can be congenital or acquired, most patients occur unilaterally. 15 Yoon et al 16 reported that EH was the main pathological change in some SSNHL patients. Meanwhile, Chen et al 17 also found that SSNHL patients with vertigo symptoms had EH in the inner ears. However, there are still no reports about the relationship between various clinical features and EH in children. In order to specifically investigate the relationship between EH and SSNHL in children, we designed this experiment.
In our study, we successively collected 30 SSNHL children (35 affected ears in total), including 12 males and 18 females. There were 22 affected ears on the left and 13 affected ears on the right. Among all children, there were 25 unilateral cases and only 5 bilateral cases. The bilateral incidence rate was only 16.7%, which indicated that the number of unilateral cases was significantly more than that of bilateral cases. It coincided with the views of Na et al 18 and Fetterman et al. 19 Furthermore, Chen et al 20 reported that in children with SSNHL, the younger the age, the greater the possibility of bilateral SSNHL. In addition to hearing loss, tinnitus was one of the most common symptoms of SSNHL children. In our study, 18 (60.0%) of 30 children had tinnitus. Besides, 12 children had dizziness, of which 9 (75.0%) were positive for EH. Our analysis of the results proved that there existed a certain correlation between the occurrence of dizziness and EH.
Regarding 30 children, 12 cases had vestibular or cochlear EH and the positive rate was 12 (40.0%) of 30. Among them, 9 children had both vestibular and cochlear EH, which indicated that SSNHL children are more likely to have EH in both vestibule and cochlea. Moreover, EH was accidentally found in the contralateral asymptomatic ears of 2 children with unilateral SSNHL. This phenomenon was also discovered in the report of Okazaki et al. 21 We speculated that the impairment may also occur in the contralateral asymptomatic ear. In addition, we found a child with the likelihood of maternal family heredity. Both his mother and grandmother had the same symptoms at a similar age, which was consistent with the views of Varga et al. 22 In past studies, a battery of susceptibility genes such as HSP70, PRKCH, ITGB3, and MTHFR had been verified in SSNHL,23-26 which indicated that genetic factors may play a momentous role in the pathogenesis of SSNHL.
The limitation of our research is that our children’s cases are all older than 10 years old, and there are no cases younger than 10 years old, which may affect the comprehensiveness of the results. On the one hand, it may be due to the lack of the ability of children younger than 10-year-old to express the symptoms and feelings of the disease, which leads to the failure to seek medical treatment in time. On the other hand, multicenter cooperation and greater attention to younger children may be able to help solve this problem.
Conclusion
Three-dimensional inversion recovery sequence with real reconstruction MRI with intravenous gadolinium injection provides a good way to show lymphatic fluid in the inner ear of SSNHL children. Although EH may be a significant consideration in the pathogenesis of SSNHL, according to our experimental results, EH may not reflect the trend of disease progression over time in children with SSNHL, but the age of onset may be an important factor in the presence or absence of EH. EH may be one of the causes of dizziness and ear fullness but has no obvious connection with the occurrence of tinnitus. Older SSNHL children with dizziness and ear fullness should maintain long-term follow-up to dynamically monitor the changes in EH.
Footnotes
Authors’ Note
W.C. conceived and designed research; Y.G. collected data and conducted research; S.L. wrote the initial paper; N.L. revised the paper; Y.S. had significant contribution to the ultimate draft. W.C. and Y.G. had equal contributions to this manuscript and should be considered as cofirst authors. All authors read and approved the eventual manuscript.
Acknowledgments
The authors would like to express sincere gratitude to Dr. Zhang and Dr. Cheng for the work-related social support during the research and Dr. Chen for the image processing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Shanghai Shenkang Hospital Development Center clinical assistant department capacity building project under Grant [SHDC22015036].