
Abstract
A 42-year-old man was referred for a week history of severe dysphagia, odynophagia, fever (39 °C), fatigue, abdominal pain, pharyngeal swelling, and multiple neck lymphadenopathies. The medical history reported a mild form of COVID-19 one month ago. The biology reported an unspecified inflammatory syndrome. The patient developed peritonitis, myocarditis, and hepatitis. A myocardium biopsy was performed. A diagnosis of Kawasaki-like disease (KLD) was performed. The occurrence of KLD in adults is rare but has to be known by otolaryngologists regarding the otolaryngological clinical presentation that may precede the multiple organ failure.
Introduction
Coronavirus disease 2019 (COVID-19) is a worldwide infection that may be associated with renal, cardiovascular, gastrointestinal, hepatobiliary, cutaneous, and neurological complications. 1 In otolaryngology, COVID-19 may primary present as multiple lymphadenopathies, parotitis, laryngological, and smell and taste sense disorders.2-4 Recently, COVID-19 was associated with a new clinical entity named Pediatric Inflammatory Multisystem Syndrome Temporally Associated with Severe acute respiratory syndrome coronavirus 2 or Kawasaki-like disease (KLD) in children that may be associated with neck and chest multiple lymphadenopathies. In this article, we reported an adult patient presenting with otolaryngological signs and symptoms mimicking Kawasaki disease.
Case Report
A 42-year-old man with no significant past medical history was referred to the otolaryngological emergency department for a week history of severe dysphagia, odynophagia, fever (39 °C), fatigue, and abdominal pain. He had no comorbidity and no medical treatment. The medical history just reported a mild form of COVID-19 (positive reverse transcription polymerase chain reaction) one month ago, which was characterized by mild dyspnea, fever, headache, and fatigue for 7 days. The clinical examination revealed hypo- and oropharyngeal mucosa swelling, multiple right neck lymphadenopathy, and nonpruritic cervical skin rash. The initial biology reported the following abnormalities: CRP = 209 mg/L, leukocytes = 12.8/mm, 3 hemoglobin = 11.9 g/dL, prothrombin = 61%, and activated fibrinogen = 9.47 g/L. The otolaryngologist performed a neck, chest, and abdominal CT scan, which reported multiple hilar and neck lymphadenopathy (IB, IIA, and IIB), and diffuse neck infiltration involving the right parapharyngeal space, piriform sinus, palatal, and tongue tonsils (Figure 1). The abdominal CT scan was unremarkable but a few hours after the admission, the patient developed a circulatory collapse with a clinical picture of peritonitis, leading to an exploratory laparotomy. The digestive surgeon did not find any abdominal abnormalities and the patient was admitted into the intensive care unit (ICU). Over the next few days, the patient developed biological and clinical hepatitis, myocarditis, and multi-organ failure, which were medically controlled. During the ICU stay, the neck lymphadenopathy and swelling disappeared regarding clinical and radiological evaluations. Extensive infectious workup was unrevealing (eg, human immunodeficiency virus [HIV], Hepatitis B virus [HBV], Hepatitis C virus [HCV], mycoplasma, legionella, tuberculosis, syphilis, toxoplasmosis, Cytomegalovirus, Herpes Zoster virus, Epstein Barr virus ). The myocardium biopsy was performed, reporting a myocarditis with neutrophil and eosinophil infiltrate without necrosis. The patient was discharged from the ICU 10 days after the admission. A Kawasaki-like syndrome (KLS) was diagnosed.
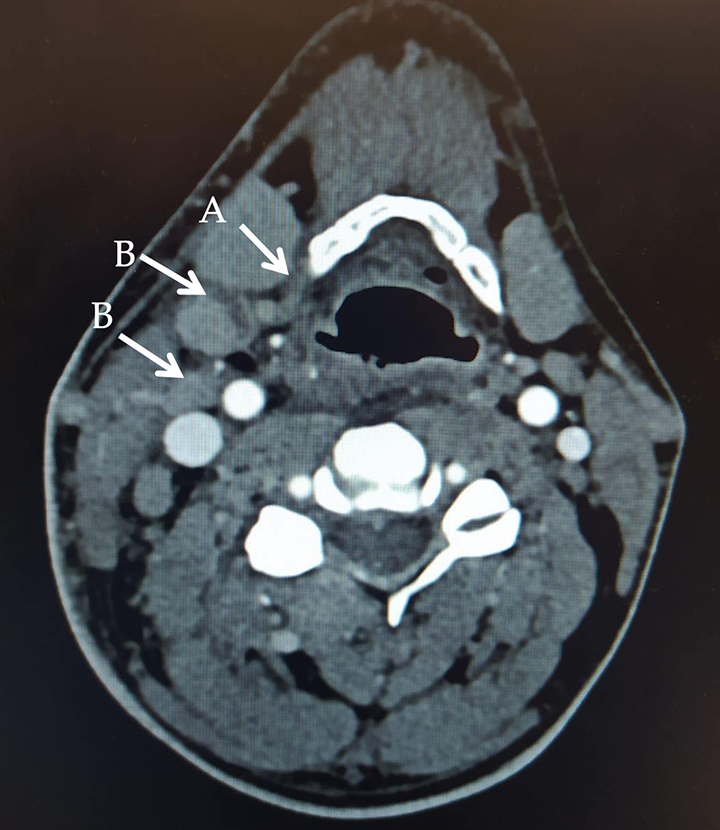
Cervical CT-scan. The admission cervical CT-scan reported right lymphadenopathy (B) and soft tissue infiltrate (A).
Discussion
The diagnostic criteria for KLS include prolonged fever of greater than 5 days, abdominal pain, upper aerodigestive tract mucosal swelling, conjunctivitis, skin rash, cervical, and hilar lymphadenopathy with laboratory evaluation consistently showing elevated inflammatory markers. Moreover, cardiac evaluation often demonstrates hypotensive shock, myocardial dysfunction, and occasionally coronary artery dilation or aneurysms. 5 According to recent data, KLS may develop a few weeks after the COVID-19 infection.5,6 To date, the majority of cases with post-COVID-19 KLS were children with unregulated inflammatory response, cardiovascular involvement, and multi-organ failure. The occurrence of KLS in adults remains exceptional. 7 The KLS not complete the diagnostic criteria of a classical Kawasaki disease that require fever lasting ≥5 days plus at least 4 of the following outcomes: cervical lymphadenopathy >1.5 cm diameter, oral mucosa abnormalities (pharyngeal erythema, strawberry tongue), bilateral bulbar conjunctival injection, polymorphous rash, and peripheral extremity changes (erythema/edema of palmar and plantar areas). 4 Note that patients with Kawasaki disease may have coronary artery disorder, cardiac arrhythmias, and ventricular dysfunction. 8 Although some features of KLS overlap with Kawasaki disease, KLS is more common among older children or adolescents, more often affects cardiovascular and gastrointestinal systems, and is more frequently associated with elevated inflammatory markers.
From a clinical standpoint, histiocytosis is usually characterized by skin and bone lesions with a histopathological examination reporting a high density of macrophages in the biopsy. In the present case, the myocardium biopsy did not report high density of macrophages but an infiltrate of neutrophils and eosinophils. The diagnosis of polyarteritis nodosa involves an impairment of the musculoskeletal system, kidney, or digestive tube where necrosis lesions may be found. In many cases, there was a history of HIV, HBV, or HCV infection. According to the patient history and the histopathological findings, this diagnosis was not retained.
The occurrence of KLS a few weeks after the COVID-19 infection led some authors to name this new clinical entity as Pediatric Inflammatory Multisystem Syndrome Temporally Associated with Severe acute respiratory syndrome coronavirus 2. 9 The pathophysiology is not well understood and would involve both abnormal immune response to the virus and vascular endothelial damage caused by viral infection. The diagnosis and its distinction from the other diseases should be primarily based on clinical presentation and laboratory findings of inflammation.
Conclusion
The occurrence of KLD in adults is still rare but has to be known by otolaryngologists regarding the otolaryngological clinical presentation that may precede the multiple-organ failure.
Footnotes
Authors’ Note
B. Johnson for the proofreading of the paper. IRB approved the study (CHUSP, 2020-01). Consent was obtained. This article does not contain any studies with human participants or animals performed by any of the authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.