
Abstract
Objectives
To evaluate the effectiveness of selective neck dissection of sublevel IIa and level III in cases of glottis and supraglottic laryngeal carcinoma in the absence of lymph node metastasis and to show if there is value in dissecting the sublevel IIb or level IV in these cases.
Patients and Methods
Twenty-five patients with N0 glottic or supraglottic cancer were subjected to unilateral or bilateral selective neck dissection according to the site and the extent of the tumor, and the specimens were histopathologically examined for metastasis.
Results
Twenty-five patients (23 males and 2 females) with mean age of 55.72 years were included in the study. Lymph node metastasis to sublevel IIa and level III was found in 6/25 (24%) cases with glottic or supraglottic carcinoma, while to sublevel IIb and level IV was found in 1/25 (4%) with P-value of 0.05, which is statistically significant.
Conclusion
Selective neck dissection of level IIb is not required in cases of the supraglottic laryngeal cancer. Dissection of sublevel IIa and level III takes less time and is effective. Dissection of level IV is not needed in the case of supraglottic cancer.
Introduction
Knowledge of the lymphatic system is essential in order to understand the pattern of spread of cancer in the neck. 1
Nodal metastases are associated with a high rate of regional recurrence and decreased survival. In fact, a single ipsilateral lymph node metastasis decreases survival by 50%, taking into account all sites of head and neck squamous cell carcinoma. 2 Contralateral or bilateral lymph node metastasis gives rise to an additional 50% reduction of the survival rate. 3
Optimal management of N0 cases is controversial. Functional neck dissection entails a non-negligible risk of nervous and lymphatic morbidity, especially when applied to sublevel IIb and level IV. As these are the least frequently affected levels, the advisability of dissection is questionable, given advances in various diagnostic strategies. 4
Because clinical palpation is not sufficiently sensitive to detect cervical nodal metastasis, computed tomography (CT), magnetic resonance imaging (MRI), and positron emission tomography imaging are useful; however, these techniques have a limited power for detection of metastasis less than 1 cm in diameter. Histopathology remains the gold standard method for detection of metastatic lymph nodes. 5
Assessing the effectiveness of selective dissection of sublevel IIa and level III nodes in cases of glottic and supraglottic laryngeal carcinoma in the absence of lymph node metastasis and addressing if there is value in dissecting the sublevel IIb or level IV in these cases were the aims of this study.
Patients and Methods
This prospective study included 25 patients with glottic, supraglottic carcinoma and with clinically and radiologically N0 nodal stage, who underwent surgery for the treatment of the primary tumor and the possible occult cervical lymph node metastasis during the period from May 2012 to February 2014 in the Otorhinolaryngology-Head and Neck Surgery Department, Kasr-El Aini hospital, Cairo university.
Informed consent was obtained from all the patients included in the study and ethical approval was taken before the start of the study from the ethical committee of the Depart ment of Otorhinolaryngology, Faculty of Medicine, Cairo University. The research complied with the principles of the Declaration of Helsinki.
Inclusion criteria
Patients with strictly N0 stage resectable tumors.
Patients accepting to be included in the study.
Patients who are surgically fitted for operation.
Patients of any age and gender.
All the patients were subjected to full history taking and full otorhinolaryngological examination. Full neck examination to exclude the presence of lymph node swelling was also done.
Endoscopic assessment through flexible laryngoscopy and direct laryngoscopy was done for all patients under general anesthesia to confirm the nature and stage of the tumor.
CT scans with contrast material were done for all patients to confirm the tumor stage (T) and the N0 stage.
Surgeries for the primary tumor were done according to the site and stage of the tumor.
All the patients had N0 stage for which extended supraomohyoid neck dissection (removal of levels I, IIa, IIb, III, and IV nodes) was done. It was done according to the site and stage of the primary tumor. Unilateral neck dissection was performed for strictly unilateral tumors, while midline tumors or those crossing the midline and all supraglottic tumors had a bilateral neck dissection.
After surgery, individual lymph nodes were grossly dissected and each level of lymph nodes of the neck dissection specimen was sent separately for histopathological examination. All the dissected nodes were labelled (Fig. 1), and then fixed in 10% formalin. The standard processing was followed and paraffin-embedded blocks were prepared. Four micrometer serial sections were mounted on glass rods for routine hematoxylin and eosin (H&E) staining and histopathological examination. According to the American Joint Committee on Cancer Staging (AJCC, 6th edition), micrometastasis was considered when it was 0.2–2 mm and macromatastasis was considered when it was more than 2 mm.

The specimen and the labeled levels of lymph nodes.
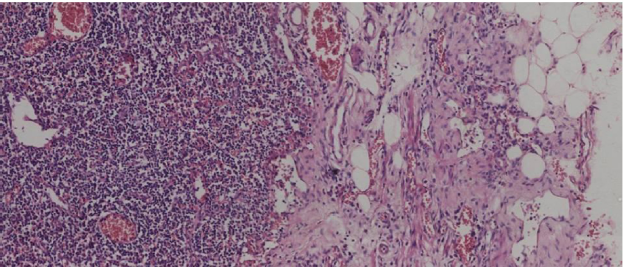
The usual metastatic nodes are shown in Figures 2 and 3. Metastases viewed with low-power microscopic field were considered positive for occult histologic macrometastases, and in this case, no further histological examination was done for these nodes.
Metastatic lymph node by H&E.
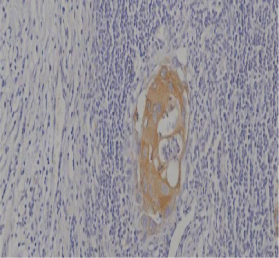
Metastatic lymph node by CK.
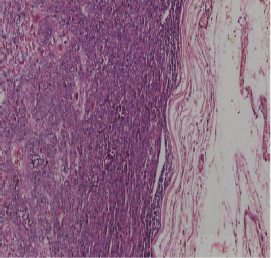
The suspicious nodes (Fig. 4) from the remaining lymph nodes that are found to be negative on routine H&E staining were submitted to immunohistochemical staining with cytokeratin (CK) followed by histopathological examination for detection of occult histologic micrometatasis.
The main significance of the study of the CK profile by immunohistochemical techniques is that it can be used as a tool of great value for tumor diagnosis and characterization in histopathology, because CK fingerprints allow classification of different epithelial tissues and also remains constant in malignant conditions.
Suspicious lymph node by H&E.
The following criteria of suspicion were settled for the selection of these suspicious nodes:
Stromal fibrosis
Granulomas
Sinus histocytosis
Endothelial proliferation
Presence of epithelioid cells as macrophages and endothelial cells, which are not easily distinguished from metastatic epithelial cells.
Nodes were considered positive for occult micrometastases if they stained positive for CK together with cytomorphological changes of malignancy.
Statistical analysis
The data were collected and tabulated, and descriptive statistics for all parameters were submitted. The SPSS program (version 17) for Windows was used for statistical analysis. The non-parametric Pearson χ 2 test was used for statistical analysis to compare macrometastasis and micrometastasis with respect to different parameters such as the level of lymph nodes involved, the site of primary tumor, and the stage of the primary tumor.
Results
Twenty-five patients with clinically and radiologically N0 nodal stage glottic, supraglottic carcinoma were included in this study. They were admitted in the Department of Otorhinolaryngology–-Head and Neck Surgery, Kasr-El Aini Hospital, Faculty of Medicine, Cairo University, in the period from May 2012 to February 2014.
The age of the patients ranged from 40 to 68 years with a mean age of 55.72 years. Patients included in this study comprised 23 males and 2 females. All patients were heavy cigarette smokers.
All the patients had extended supraomohyoid neck dissection of levels I, IIa, IIb, III, and IV lymph nodes.
The primary tumor sites of the 25 patients with laryngeal carcinoma included 11 glottis and 14 supraglottic tumors (Table 1).
Primary tumor site, laterality, and stage of patients in the study.
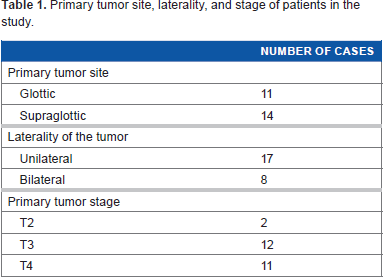
The tumor was unilateral in 17 patients, while it was midline or crossing the midline in 8 patients. Staging of the primary tumors at the time of surgery revealed that 2 cases were classified as T2, 12 as T3, and 11 as T4. All patients had clinical N0 cervical nodal stage before surgery (Table 1).
Among the 25 patients participated in this study, 8 patients had cervical lymph node macrometastasis with an incidence rate of 32%. Of them, two patients showed both macrometastasis and micrometastasis.
In the analysis based on the primary tumor sites, the incidence rates of nodal macrometastasis with H&E staining were 18.1% (2/11) and 42.8% (6/14) for glottic and supraglottic tumors, respectively, which was statistically significant (Fig. 5).
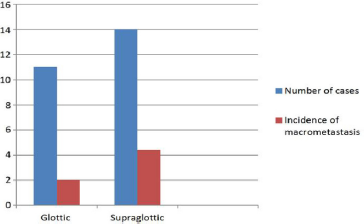
Number of macrometastasis in the study with respect to the site of the primary tumor.
In the analysis based on the primary tumor staging, the incidence rates of nodal macrometastasis with H&E staining were 50% (1/2) in T2 tumors, 25% (3/12) in T3 tumors, and 36.3% (4/11) in T4 tumors with no statistically significant difference.
In the analysis based on the level of lymph nodes, the incidence rates of nodal macrometastasis with H&E staining were 8.3% (1/12) in level I, 7.8% (7/90) in sublevel IIa, 0% (0/88) in sublevel IIb, 4.4% (7/159) in level III, and 4.9% (2/41) in level IV (Fig. 6).
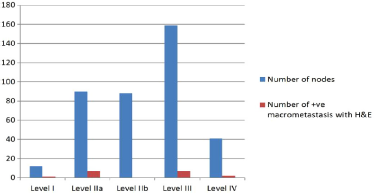
Number of macrometastasis with respect to the level of lymph nodes.
With further histopathological examination after staining with CK antibody stain for the nodes that were reported to be negative (371 nodes out of 390 dissected nodes), two nodes showed micrometastasis in the form of micrometastatic focus (cluster of cells).
In this study, among the 25 patients, 2 patients had cervical lymph node micrometastasis with an incidence rate of 8%.
In the analysis based on the primary tumor sites, the incidence rates of nodal micrometastasis with CK antibody staining were 0% (0/11) and 14.3% (2/14) for glottis and supraglottic tumors, respectively, which was not statistically significant.
In the analysis based on the primary tumor staging, the incidence rates of nodal micrometastasis with CK antibody staining were 0% (0/2) in T2, 16.7% (2/12) in T3 tumors, and 0% (0/14) in T4 tumors.
In the analysis based on the level of lymph nodes involved, the incidence rates of nodal micrometastasis with CK antibody staining were 0% (0/12) in level I, 1.1% (1/90) in sublevel IIa, 0% (0/88) in sublevel IIb, 0% (0/159) in level III, and 2.4% (1/41) in level IV (Fig. 7).
When comparing the results of metastasis based on the level of lymph nodes, metastasis was found to sublevel IIa and level III in 6/25 (24%) cases with glottic and supraglottic carcinoma, while to sublevel IIb and level IV in 1/25 (4%) with P-value = 0.05, which is statistically significant.
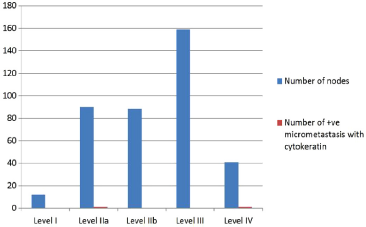
Number of micrometastasis with respect to level of lymph nodes.
When comparing the results of metastasis based on the primary tumor site, positive lymph node metastasis was commonly found in 6/11 (54.5%) supraglottic cases than in 2/14 (14.3%) glottic cases with P-value = 0.03, which is statistically significant.
Discussion
Lymph node metastasis remains the single most important prognostic factor for most tumors and determines the choice of therapy in patients with head and neck squamous cell carcinoma (HNSCC). 6
If metastases to the cervical lymph nodes are clinically evident at diagnosis, treatment of the neck is mandatory. This situation is more controversial when no clinical signs of neck disease are found (N0 neck).
In this situation, the surgeon must decide whether to electively treat the neck or wait for metastases to develop and then treat the patient whenever they occur. The limitations in the identification of micrometastases and the negative impact of recurrences in the neck are still a challenge. 7
It should be noted that neck dissection has the advantage of staging the neck disease and determines whether an adjuvant therapy is required. If the choice of neck dissection for the treatment of N0 neck is decided, then the question of whether the neck dissection should routinely be directed at both sides of the neck arises. 8
In this study, 10 patients with laryngeal cancer who were cN0 before surgery were upstaged after selective neck dissection to pN1 and two of them were diagnosed with micrometastasis after immunohistochemical staining with CK.
Yao et al in their study in 2005 stated that at the time of salvage surgery, 10 of 22 patients received elective neck dissections and 2 (20%) of 10 patients were found to have occult metastases. These two patients with pathologically positive adenopathy survived less than 2 years. 9
It is important to bear in mind that lymphatic anatomy of the neck at sublevel IIb is more related to the lymphatic chain of the spinal accessory lymph nodes and is not a primary route of laryngeal cancer. 10
In this study, where 42 selective neck dissections were performed, no single metastasis was observed in sublevel IIb even in cases in which sublevel IIa was involved.
Based on the study by Corlette et al in 2005, the sublevel IIb lymphatic metastases were derived from nasopharynx, nasal cavity, oral cavity, and pharynx primaries. 11
In addition, the prospective series of Silverman et al in 2003 demonstrated that the sublevel IIb was involved only if the sublevel IIa was pathologically positive. 12
In light of all this, the sublevel IIb might be spared from cancer of the larynx with a clinically N0 neck.
In this study, we observed that nodal metastasis is more common with cases of supraglottic laryngeal carcinoma. Also nodal metastasis increases with increasing stage.
Wax and Touma in their study in 1999 stated that supraglottic cancer has a high rate of metastatic adenopathy. They advocate bilateral elective treatment of the necks during primary therapy. They also recommended bilateral elective neck dissections in the cases of recurrent supraglottic laryngeal cancer because of a frequent rate (28%) of occult metastases. 13
In this study, we observed that patients may complain of some shoulder pain after neck dissection, especially when we try hard to remove the sublevel IIb lymph node in the cases of T3 or T4 laryngeal carcinoma.
Several studies have been carried out to compare health-related quality of life in patients having no neck dissection and those having an and those having Selective Neck Dissection (SND), with particular emphasis on postoperative shoulder dysfunction.
It is interesting that patients who underwent unilateral level III or IV dissections had similar mean scores for shoulder dysfunction for patients who did not undergo neck dissection, whereas patients with bilateral level III and IV dissections reported much worse scores on average. The addition of postoperative radiation therapy negatively contributed to shoulder dysfunction scores. 14
Some studies provide support for the idea that the lymph nodes of sublevel IIb need not be routinely removed during SND. In these cases, a “super-selective” neck dissection may be justified so that spinal accessory nerve dissection and subsequent dysfunction can be minimized and operative time can be saved. 15
In 2009, Goudakos et al in their systematic review showed that the proportion of occult metastasis varied between 0 and 30%. 16
However, it should be noted that the percentages of subclinical metastases of supraglottic laryngeal carcinoma must be viewed with caution because they are based on the findings from a time when palpation and conventional pathologic analysis were the most widely used means of examination, compared to the current situation, where imaging (ultrasound, CT, or MRI) and molecular analysis in the pathologic staging are broadly available and more accurate.
The currently available preoperative clinical or imaging techniques were noneffective in predicting the lymph node status. Furthermore, the histopathological analysis was unable to detect occult metastasis, as even neck nodes that are reported as pathologically disease free may harbor tumor cells.
The introduction of more sensitive techniques, such as immunochemical technique and molecular analysis, has improved the possibility of isolating subclinical metastasis, but haematoxylin and eosin-stained sections still remain the most widely used modalities. 17
In this study, among the 25 patients, eight patients who were diagnosed preoperatively as N0 were pathologically upstaged as they have positive lymph node metastasis by but haematoxylin and eosin staining and two patients were upstaged as they have positive nodes after CK staining.
Conclusions
Selective neck dissection of sublevel IIb in cases of supraglottic laryngeal cancer is not required as metastasis does not occur at this level primarily, it takes a long time intraoperatively to dissect it, and high morbidity of the patient due to close proximity with spinal accessory nerves.
Super selective neck dissection of sublevel IIa and level III is much easier, takes less time, and has less morbidity. Dissection of level IV is not required in the cases of supraglottic laryngeal cancer. Routine histopathological examination may not be sensitive in the cases of N0 neck, and further examination with special stains, such as CK, may be required.
The sample size in this study should be encouraging for further studies with more number of patients to have more statistically significant data regarding the effectiveness of selective neck dissection of sublevel IIa and level III in the cases of glottis and supraglottic laryngeal carcinoma in the absence of lymph node metastasis and to indicate the need for removal of sublevel IIb or level IV in these cases.
Author Contributions
Analyzed the data: MAAH, HMA. Wrote the first draft of the manuscript: MAAH, LSE, HMA. Contributed to the writing of the manuscript: IZ, MFE, AAH. Agree with manuscript results and conclusions: MAAH, HMA, LSE, MFE. Jointly developed the structure and arguments for the paper: AAH, IZ. Made critical revisions and approved final version: IZ, AAH, HMA, MAAH. All authors reviewed and approved of the final manuscript.