
Abstract
Objective:
The aim of this study was to assess the long-term effectiveness of quantic molecular resonance (QMR) in the treatment of inferior turbinate hypertrophy (ITH) in allergic and nonallergic rhinitis refractory to medical therapy.
Methods:
This study enrolled 281 patients, 160 males (56.9%) and 121 females (43.1%), mean age 37.8 ± 4.1 years, range 18 to 71. Fifty-four patients have been lost to follow up and have been therefore excluded from the final analysis. Based on skin prick test results, 69 patients were considered allergic (group A) and 158 nonallergic (group B). All subjects underwent before surgery (T0) and 3 (T1), 12 (T2), 24 (T3), and 36 months (T4) after QMR treatment to: 4-phase rhinomanometric examination, nasal endoscopy evaluation, and visual analogue scale to quantify the subjective feelings about nasal obstruction.
Results:
Subjective and objective parameters showed statistically significant improvement in both groups. Group B parameters not changed during follow-up, while group A showed significant worsening between T1 and subsequent assessments. T4 outcome indicates a better result in nonallergic patients.
Conclusions:
In accordance with the literature, our preliminary data validate QMR treatment as a successful therapeutic option for nasal obstruction due to ITH. Nonallergic patients had a very good T4 outcome. Allergic patients showed a worsening trend after 1 year probably due to other causes.
Keywords
Introduction
inferior turbinate hypertrophy (ITH) is one of the most common causes of nasal obstruction; this condition is due to persistent inflammation with edema and prolapse of the mucosa of inferior turbinates. 1
Allergic rhinitis (AR) is one of the most common cause of ITH. Several studies revealed that a fourth of the population has allergy-related ITH. In some patients, the vascular dilatation leads to a prolapse of the submucosal venous sinusoids, which no longer responds to the sympathetic system and to medical treatment. 2
When medical treatments (antihistamines, steroids, and specific immunotherapy) are inadequate to solve the obstructive symptom, a surgical approach to improve the nasal airflow is often necessary. 3 The gold standard for surgical ITH treatment includes successful volumetric tissue’s reduction with preservation of inferior turbinate mucosa. Numerous surgical techniques (total or partial turbinectomy, turbinoplasty, thermal techniques, and laser surgery) have been proposed for the treatment of ITH, and their main purpose is to increase nasal airflow while maintaining physiological mucosal functioning. 4 Many of these techniques are highly destructive, this could cause loss of nasal sensitivity and the formation of the so-called “empty nose” syndrome with the formation of crusts, bleeding, and synechia with negative impact on the quality of life (QoL) of the patients. 5 The aim of this study was to assess the long-term effectiveness of quantic molecular resonance (QMR) in the treatment of ITH in allergic and non-AR refractory to medical therapy.
Materials and Methods
This study enrolled 281 patients with chronic nasal airway obstruction caused by ITH, without septal deviations or with minor deviations, who had been admitted to the ENT Department of Cardarelli Hospital in Naples between February 2014 and January 2017. All patients underwent inferior turbinate’s volumetric tissue reduction for ITH. Surgery was performed using Vesalius Quantum (Quantum Molecular Resonance Turbinoplasty).
All procedures performed in studies involving human participation were in accordance with the ethical standards of the institutional research committee of the Cardarelli Hospital of Naples and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study. Moderate-to-severe septal deviation, infectious rhinitis, systemic diseases, allergy, nasal polyps, acetylsalicylic acid sensitivity, cystic fibrosis, primitive ciliary dyskinesia, and history of previous nasal surgery were considered as exclusion criteria.
Skin prick test (SPT) was performed using a standard allergen extract panel (Stallergenes-Greer Company). Positive (histamine) and negative (distilled water) controls were also performed. We tested the following aeroallergens: house dust mite, pollens, alternaria, aspergillus, cladosporium, grasses, weeds, wheat, and cockroach 6 ;
All subjects underwent before surgery (T0) and 3 (T1), 12 (T2), 24 (T3), and 36 months (T4) after surgery to: four-phase rhinomanometric examination allowed the objective assessment of the airflow and its resistances through the nasal pits. Therefore, the results have been classified in relation to the values of resistance to airflow in low, medium, and high resistance
7,8
; nasal endoscopy evaluation was performed at baseline before surgery (T0) and 4 times after surgery: at 3 (T1), 12 (T2), 24 (T3), and 36 months (T4). It was performed without decongestant or local anesthesia using a 3-mm 0-degree rigid fiberoptic endoscope (Karl Storz) and scored as previously described by Lund and Kennedy (LK score).
9
The videos were further scored using a Modified Lund-Kennedy (MLK) endoscopic scoring system, which retains the LK edema subscores for the inferior turbinates only
10
; the visual analogue scale (VAS) was used to quantify the subjective feelings through questions about nasal obstruction (obstruction-VAS [O-VAS]). Patients were asked to position a cross on a line, ranging from 0 (no obstruction) to 10 (complete obstruction), corresponding to their own perception of nasal obstruction. The disease was divided into mild, moderate, and severe based on O-VAS scores (mild, 0-3; moderate, 4-7; and severe, 8-10).
11
Garzaro et al indicated that an O-VAS score >5 negatively impacts on patient’s QoL.
12
Patients were divided into 2 groups following the results of SPT allergy tests: Group A: allergic patients Group B: nonallergic patients
All patients underwent QMR treatment on inferior turbinates. We started a contact local anesthesia applying a cotton wool soaked in lidocaine on the medial and inferior faces of inferior turbinates 10 minutes before surgery.
The submucosal decongestion of the turbinate was performed through insertion of a needle-shaped handpiece, activated by a QMR machine, the so-called Quantum (Telea), with an intensity force of 5.0 for 20 to 30 seconds. This allowed an immediate shrinkage of the mucosa and a reduction in the prolapse of the mucosal hypertrophy. A 3-mm 0-degree nasal fiberoptic endoscope (Karl Storz) was used to give a clear view on the nasal cavity and the wand was inserted in the anterior portion of the inferior turbinate. We performed the treatment pricking the lateral face of the turbinates 3 times in 3 different parts: head, body, and tail. Because of its physiological key role, we have been careful to avoid mucosal damage of the turbinates. All subjects received topical therapy with sodium chloride 0.9% nasal spray (2 puffs for each naris 5 times a day for 21 days). The procedure did not cause bleeding and did not require insertion of nasal tampons in any patients.
MedCalc Statistical Software version 19.1.7 (MedCalc Software bvba; https://www.medcalc.org) was used to perform statistical analysis. Our data were tested with the Student t test. P < .05 was considered statistically significant.
Results
This study enrolled 281 patients, 160 (56.9%) males and 121 (43.1%) females, mean age 37.8 ± 4.1 years, range 18 to 71. Fifty-four patients were lost during follow-up and therefore were excluded from final analysis. Thus, our study population counted 227 patients.
Based on SPT results, 69 patients were considered allergic (group A) and 158 nonallergic (group B). The O-VAS data are shown in Table 1, while Figure 1 shows the temporal trend and 2 groups final outcome.
O-VAS Score of Group A Patients.a
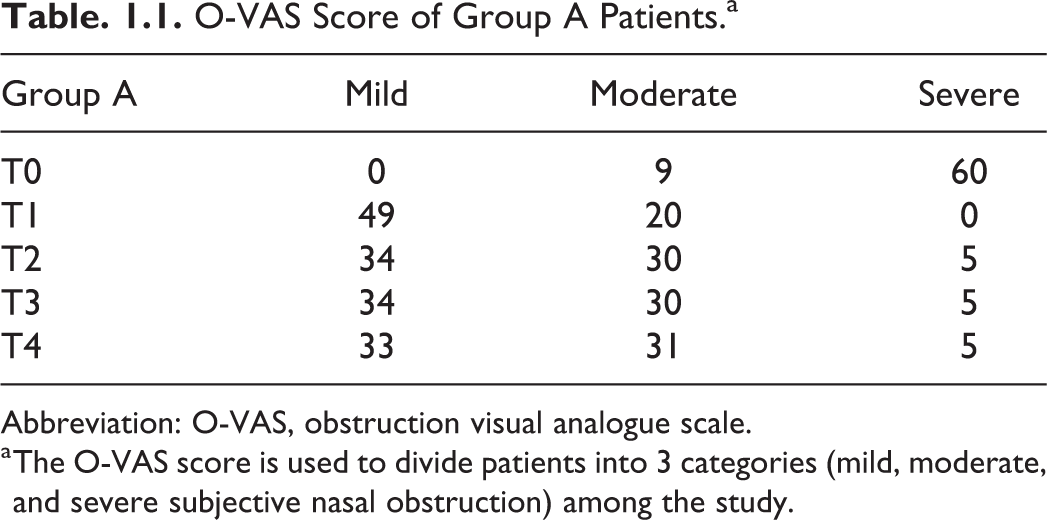
Abbreviation: O-VAS, obstruction visual analogue scale.
a The O-VAS score is used to divide patients into 3 categories (mild, moderate, and severe subjective nasal obstruction) among the study.
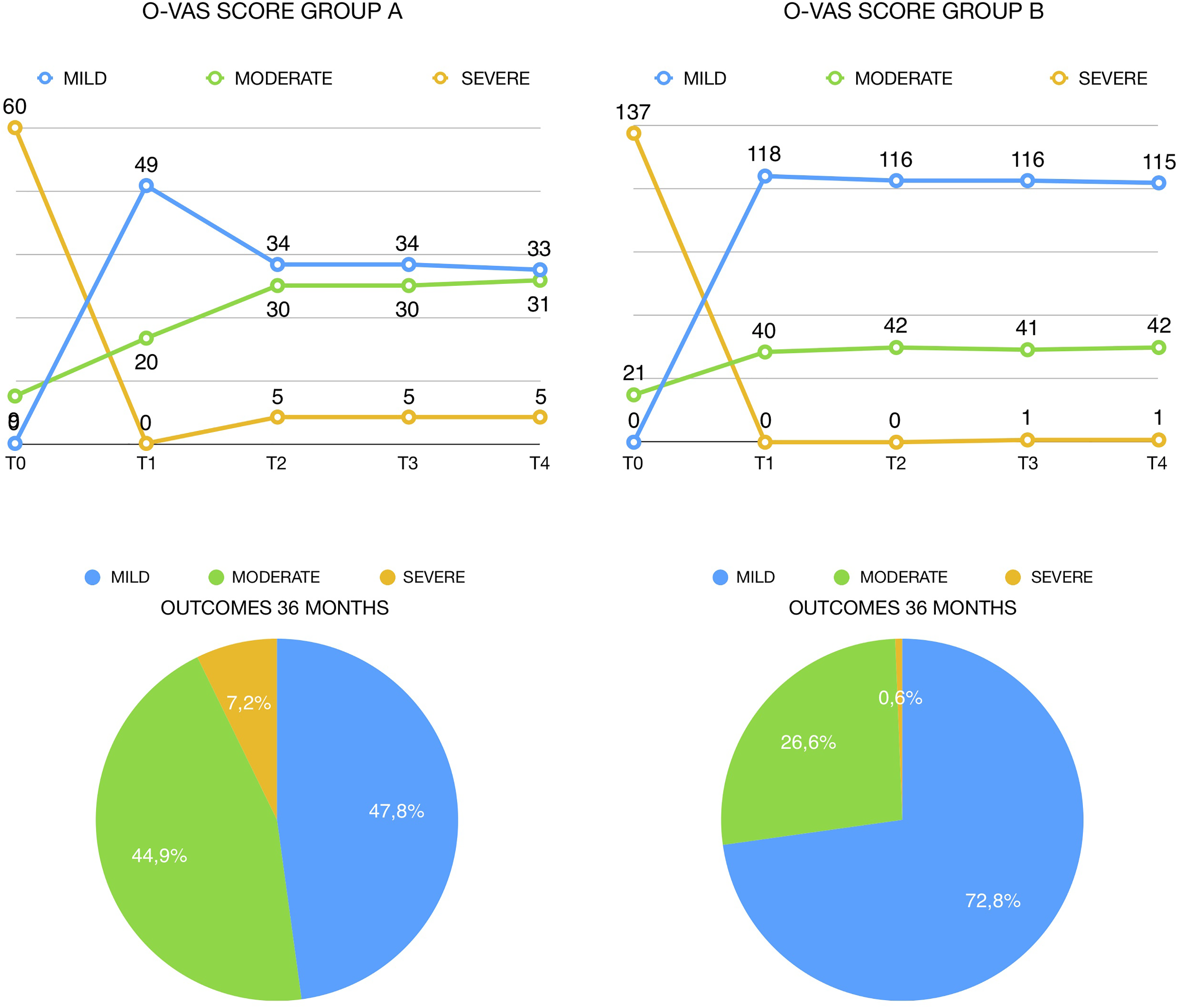
Graphical representation of Table 1.1 and Table 1.2. Diagram in Figure 1.1 shows a worsening of O-VAS score between T1 and T2 in allergic patients. The outcome (T4 = 36 months after treatment) of both groups is represented at bottom, and nonallergic group shows a better outcome. O-VAS indicates obstruction visual analogue scale.
Before surgery, group A showed severe nasal obstruction in 60 (86.96%) patients and moderate obstruction in 9 (13.04%) patients (Table 1.1). The O-VAS score of group B showed severe nasal obstruction in 137 (86.71%) patients and moderate obstruction in 21 (13.29%) patients (Table 1.2). No patients met criteria for mild nasal obstruction.
O-VAS Score of Group B Patients.a
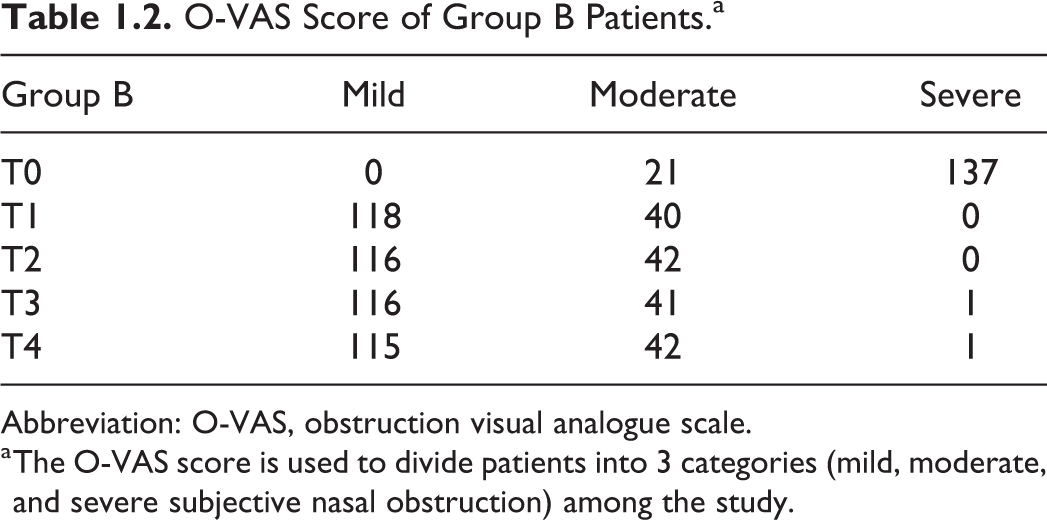
Abbreviation: O-VAS, obstruction visual analogue scale.
a The O-VAS score is used to divide patients into 3 categories (mild, moderate, and severe subjective nasal obstruction) among the study.
Three months after QMR treatment (T1), no patients met criteria for severe nasal obstruction in both groups. Forty-nine patients of group A (71.01%) and 118 (74.68%) of group B met criteria for mild nasal obstruction, while 20 (28.99%) patients of the group A and 40 (25.32%) patients of the group B reported moderate nasal obstruction.
Analyzing data of group A 12 months after QMR treatment (T2), 5 (7.25%) patients met criteria for severe nasal obstruction, 30 (43.48%) for moderate nasal obstruction, and 34 (49.28%) for mild nasal obstruction. At T3 (24 months), our sample showed the same distribution, and at T4, only a slight difference could be observed. Group A showed a significative, good, short-time outcome after QMR treatment (T0-T1: P < .05), a slight worsening of results at T2, which is confirmed in subsequent follow-up evaluations.
Group B showed a significative, good outcome at T1 (T0-T1: P < .05), which did not show statistically significative differences in subsequent follow-up evaluations. The 36-month (T4) outcome of group B could be predicted from the 3-month (T1) evaluation, and group A showed substantial differences between T1 and subsequent follow-up evaluations, while group B showed better outcome (Figure 1).
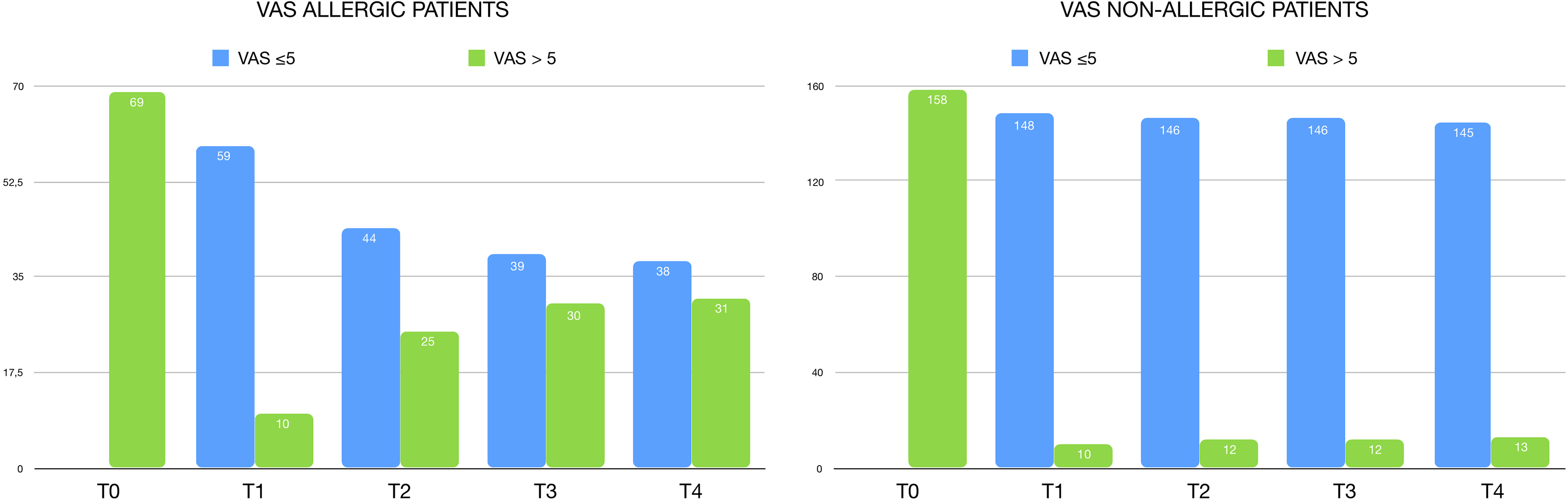
A brief analysis of the impact of nasal obstruction on QoL is shown in Figure 2.1 and Figure 2.2, and numerical values are shown in Table 2.1 and Table 2.2. Before surgery, all patients had a VAS score >5.
Quality of Life of Group A Patients.a
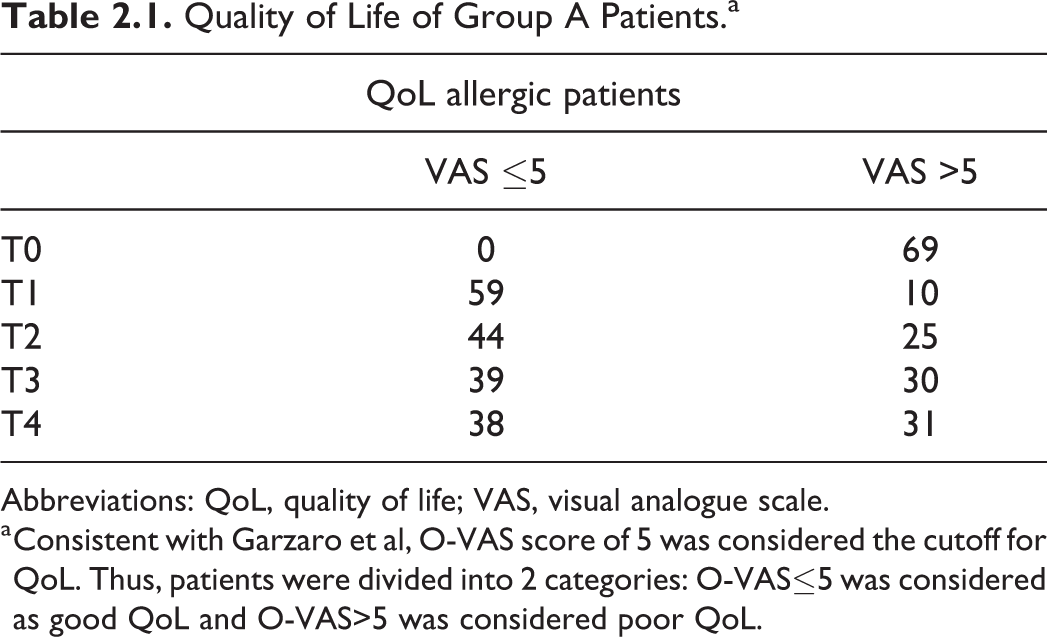
Abbreviations: QoL, quality of life; VAS, visual analogue scale.
a Consistent with Garzaro et al, O-VAS score of 5 was considered the cutoff for QoL. Thus, patients were divided into 2 categories: O-VAS≤5 was considered as good QoL and O-VAS>5 was considered poor QoL.
Quality of Life of Group B Patients.a
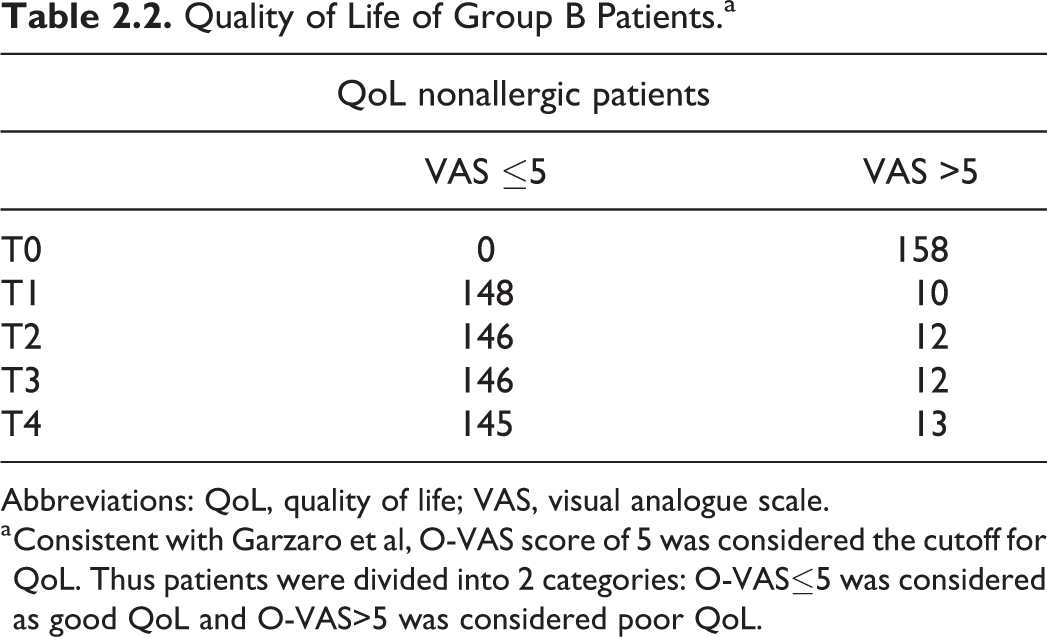
Abbreviations: QoL, quality of life; VAS, visual analogue scale.
a Consistent with Garzaro et al, O-VAS score of 5 was considered the cutoff for QoL. Thus patients were divided into 2 categories: O-VAS≤5 was considered as good QoL and O-VAS>5 was considered poor QoL.
At T1, 59 (85.51%) allergic patients of the group A showed a significative positive impact on QoL, while 10 (14.49%) still had a poor QoL. Among the following evaluation, the percentage of patients complaining a poor QoL tends to grow up to 44.93%. Group B showed a significative positive impact on QoL at T1, which is confirmed in subsequent follow-up evaluations.
Table 3.1 shows that the majority of Group A had an MLK score of 3 at baseline (T0), 17 had MLK score 2, and no one had MLK score 1. The first postsurgical evaluation (T1) showed a significative improvement: 49 patients scored 1, 20 scored 2, and no one scored 3. At T2, 33 patients scored MLK 1, 31 scored MLK 2, and 5 scored MLK 3. Later, follow-up evaluations did not show substantial changes in group A.
Modified Lund-Kennedy Score of Group A Patients.a
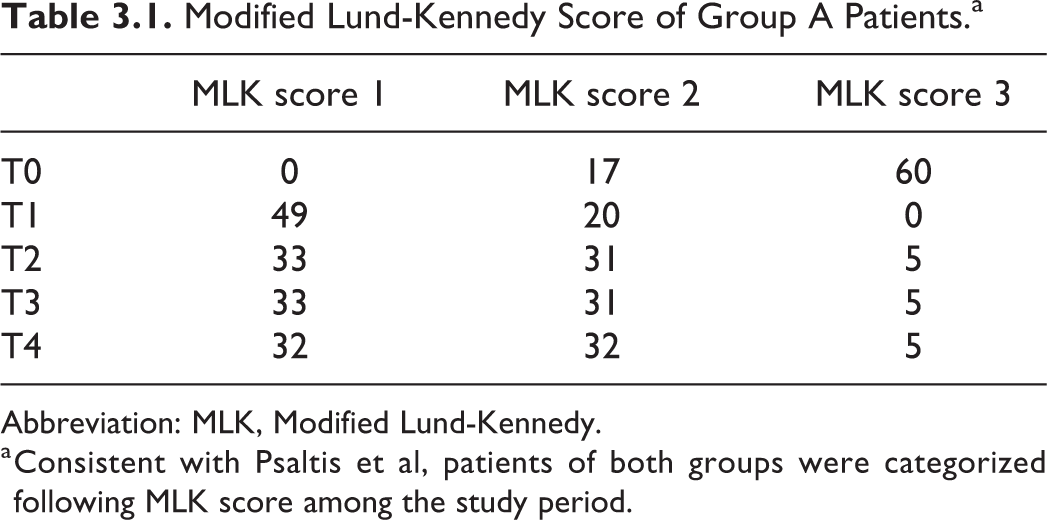
Abbreviation: MLK, Modified Lund-Kennedy.
a Consistent with Psaltis et al, patients of both groups were categorized following MLK score among the study period.
Twenty-eight patients of the group B scored MLK 3, 130 scored MLK 2, and no patients scored MLK 1. This group had a significative improvement at T1: 120 patients scored MLK 1, 38 scored MLK 2, and no one scored MLK 3. Later, follow-up evaluations did not show any significative change.
The temporal trend of MLK’s analysis in both groups is represented in Figures 3.1 and 3.2: Groups A and B showed a significative improvement between T0 and T1. Both groups showed no significative differences between T2 and T3 and between T3 and T4. Group A showed a worsening of MLK score between T1 and T2, while group B did not show any difference between T1 and T2.
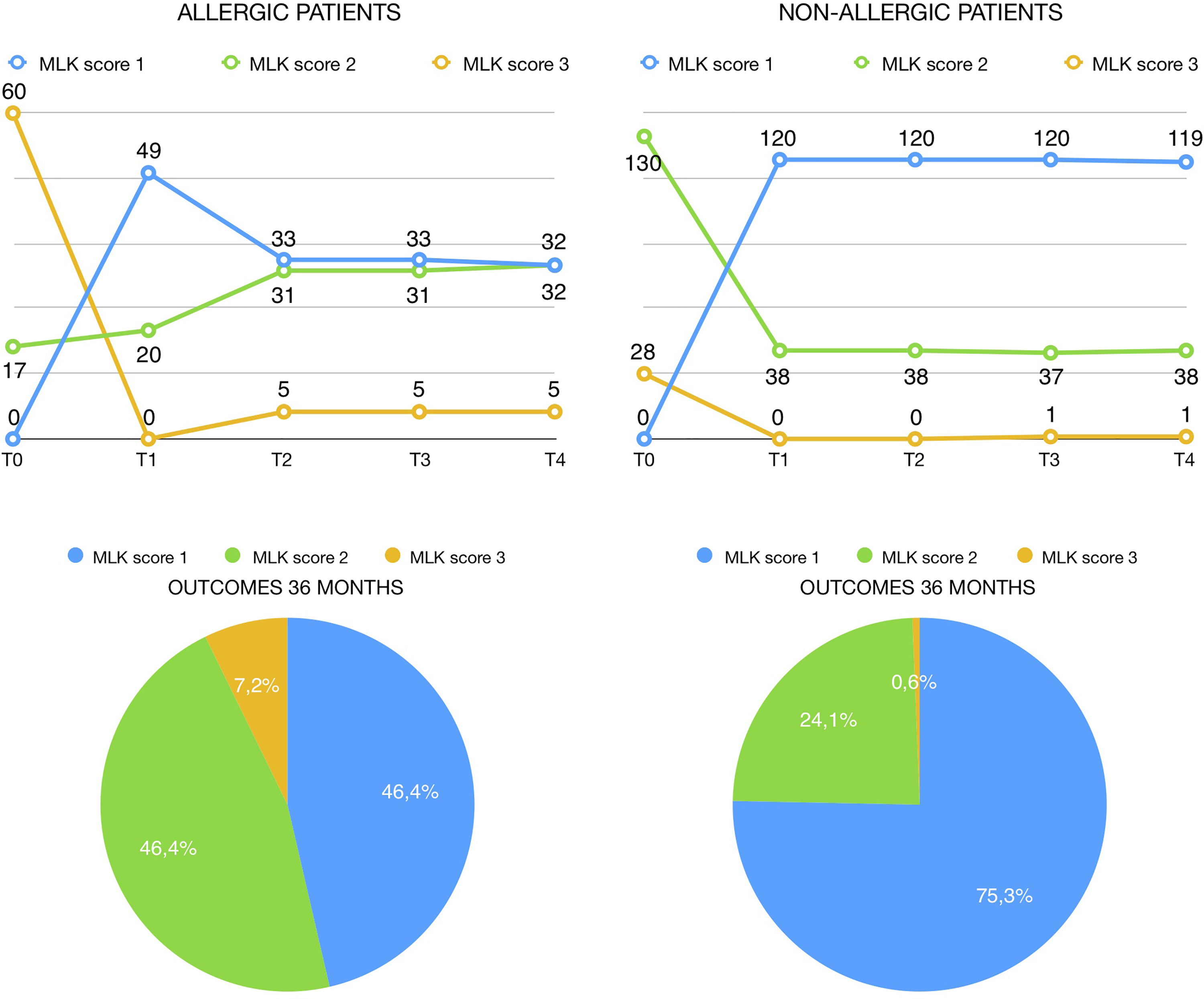
Graphical representation of Table 3.1 and Table 3.2. Diagram in Figure 3.1 shows a worsening of MLK score between T1 and T2 in allergic patients. The outcome (T4 = 36 months after treatment) of both groups is represented at bottom, and nonallergic group shows a better outcome. MLK indicates Modified Lund-Kennedy.
Modified Lund-Kennedy Score of Group B Patients.a
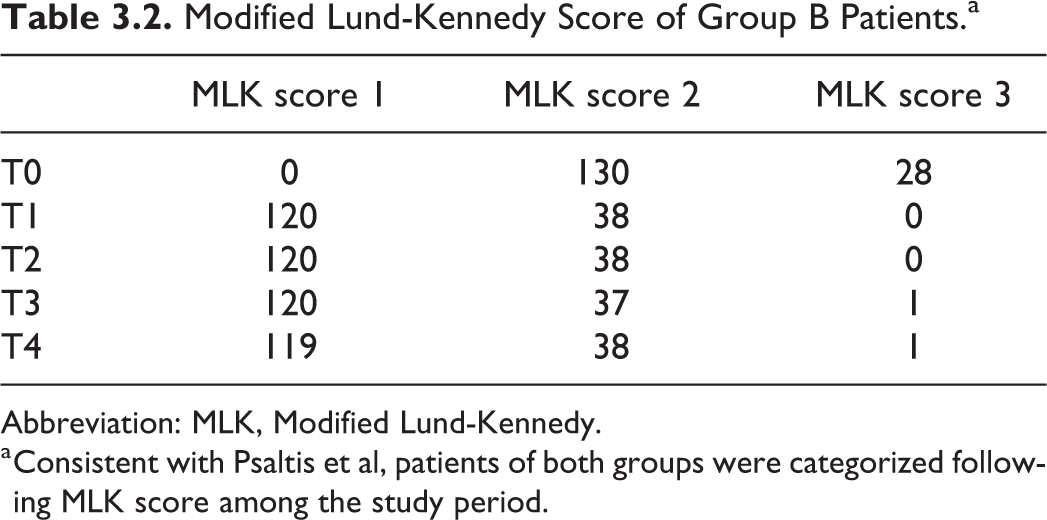
Abbreviation: MLK, Modified Lund-Kennedy.
a Consistent with Psaltis et al, patients of both groups were categorized following MLK score among the study period.
Final outcome (T4) showed a better result in nonallergic patients: 75.3% had MLK 1, 24.1% had MLK 2, and only 0.6% had MLK 3 (Figure 3.2). Group A had a worse final outcome: 46.4% had MLK 1, 46.4% had MLK 2, and 7.2% had MLK 3 (Figure 3.1).
Before surgery, the rhinomanometric analysis of airflow resistances showed high resistance in 23 (33.33%) patients and medium resistance in 46 (66.67%) patients from group A (Table 4.1).
Rhinomanometric Evaluation of Group A Patients.a
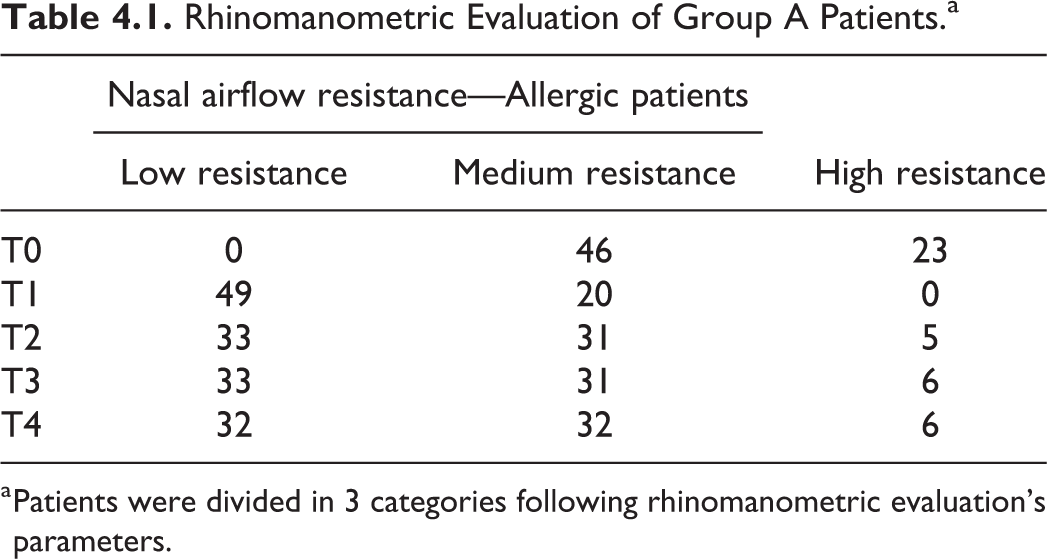
a Patients were divided in 3 categories following rhinomanometric evaluation’s parameters.
Group B showed high airflow resistances in 50 (31.65%) patients and medium resistances in 108 (68.35%) patients. Nobody showed low airflow resistance. Forty-nine of the group A (71.01%) showed low resistance at T1, and 20 (28.99%) showed medium resistance. No one showed high airflow resistance.
High airflow resistances at T2 follow-up evaluation were detected in 5 (7.25%) patients in group A, medium resistances in 31 (44.93%) patients, and low resistances in 33 patients (47.83%). T3 and T4 outcomes showed substantially similar results.
Group B patients showed low airflow resistances in 119 (75.32%) patients and medium resistances in 39 (24.68%) patients at T1; subsequent follow-up evaluations did not show any significative difference. Figure 4.1 and Figure 4.2 represent the temporal trend of nasal airflow measurement across the follow-up window and the final outcome at T4, which is better in nonallergic group.
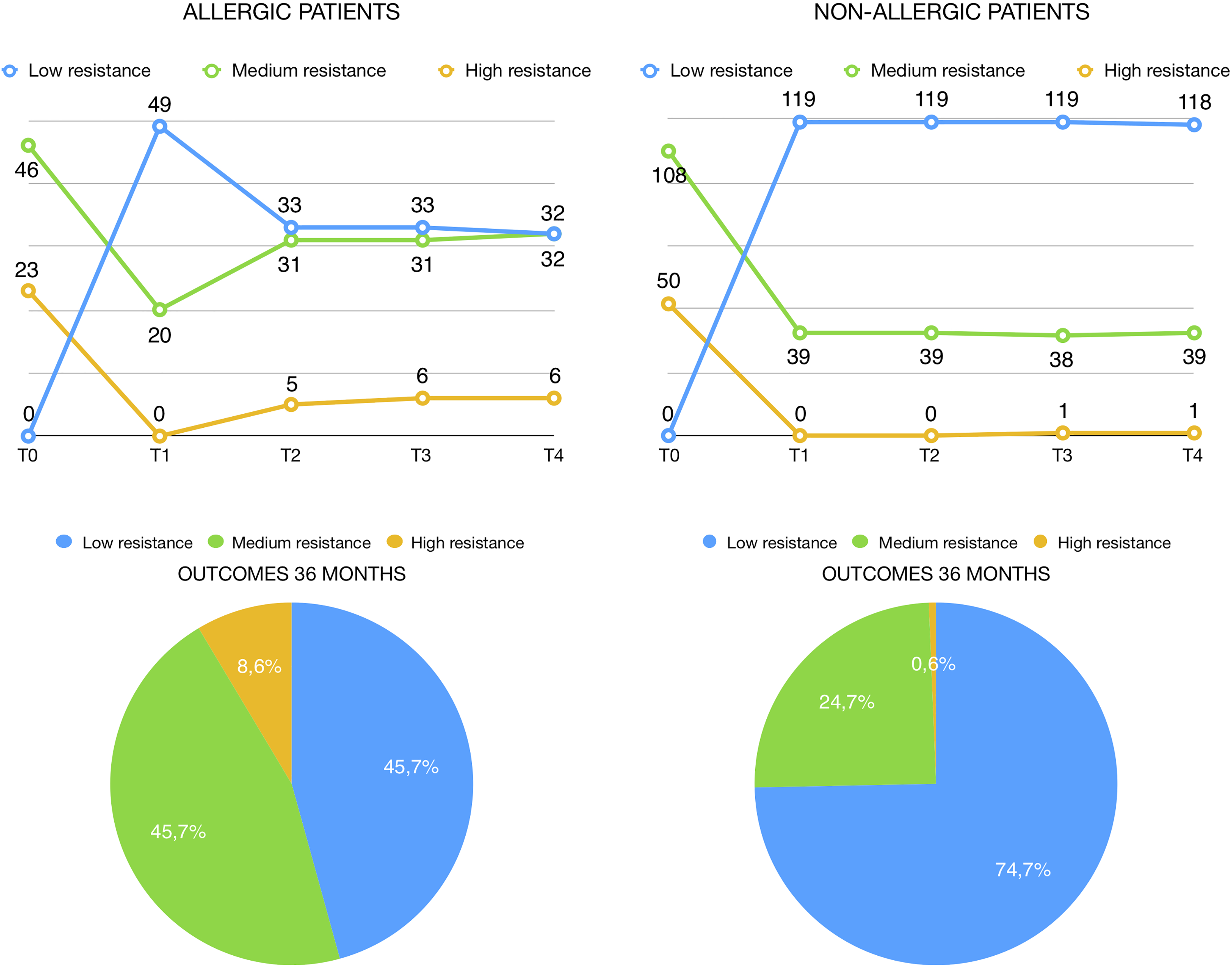
Graphical representation of Table 4.1 and Table 4.2. Diagram in Figure 4.1 shows a worsening of rhinomanometric parameters between T1 and T2 in allergic patients. The outcome (T4 = 36 months after treatment) of both groups is represented at bottom, and nonallergic group shows a better outcome.
Rhinomanometric Evaluation of Group B Patients.a
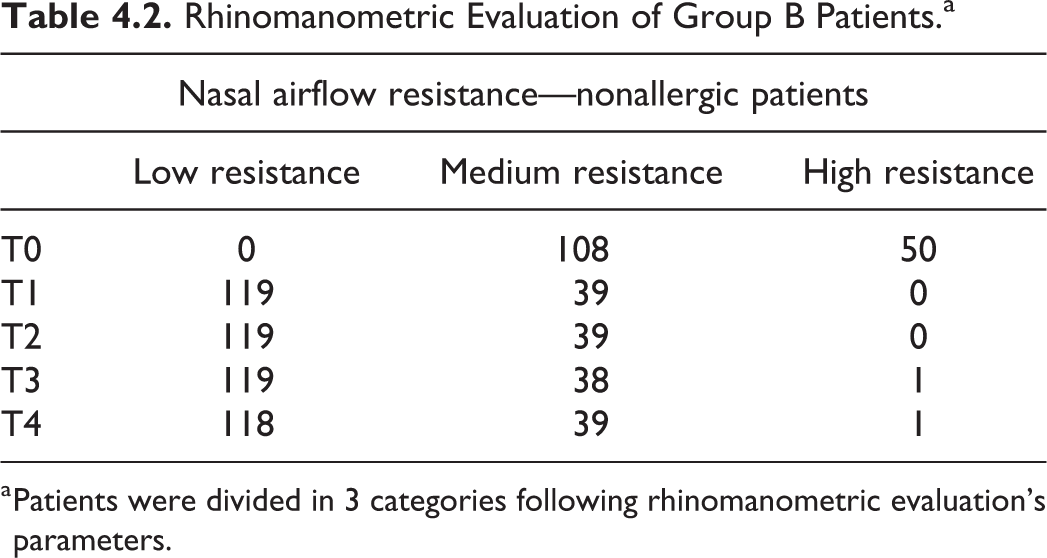
a Patients were divided in 3 categories following rhinomanometric evaluation’s parameters.
We observed adverse reactions like a slight crust formation, which not required any treatment and was spontaneously cleared up in about 7 days in 39 (17.2%) patients and turbinoseptal synechiae in 3 (1.3%) patients. Two (0.9%) patients needed nasal tamponade, and 12 (5.3%) patients had intraoperative vagal syndrome. In both cases, a suspension of surgery was not needed. Nine (8.7%) patients needed to take analgesics (paracetamol 1 g twice a day) for 2 days after surgery.
In group A, we observed a statistically significative (P < .05) improvement of QoL at T1, and the treatment’s efficacy on the QoL tends to decrease within 1 year. According to the literature, our data showed that the mucosal inflammation has a very important role in the pathogenesis of the swelling of nasal mucosa in the allergic patients. 13,14
Therefore, QMR treatment for allergic ITH should be associated with local and systemic medical treatment. 15,16 Long-term evaluation showed that QMR treatment for ITH provides decrease in nasal airflow resistance and has subjective benefits that still persist 36 months after the procedure. We demonstrated that QMR treatment for HIT in allergic patients provides an improvement in nasal airflow with a reduction in nasal obstructive symptoms, but its efficacy tends to decrease within 12 months.
Discussion
Various surgical techniques are described for the treatment of ITH including total or partial turbinectomy, turbinoplasty (outfracture, submucous resection, microdebrider), thermal techniques (electrocautery, cryotherapy, radiofrequency ablation [RFA]), and laser surgery. Contemporary literature mainly focused on the use of RFA and microdebrider due to their efficacy of preservation of nasal physiology. These techniques aim to protect nasal mucosa preserving nasal physiologic function. 1
Radiofrequency ablation transmits the kinetic energy of radio frequencies to tissues, increasing its temperature to 64 to 80 degrees generating small necrotic areas in the turbinate tissue. De Corso et al evaluated 305 patients in a 5-year follow-up study and showed that RFA can be considered a safe procedure that only slightly alters nasal mucosa, while preserving physiologic function with minor discomfort and a low risk of side effects. Furthermore, their results demonstrated that RFA offers very good results for at least 36 months. They have detected, in the following 2 years, a worse temporal trend in terms of recurrence rates, especially in allergic patients. 17 Long-term evaluation showed that RFA for allergic or nonallergic ITH appeared to provide improvement in olfaction, decrease in nasal resistance, and had subjective benefits that were still maintained 2 years after the procedure. 18 De Corso et al demonstrated that RFA provides an improvement in nasal airflow with a reduction in nasal obstructive symptoms in the short term, but its efficacy tends to decrease within 3 years. 17 Incandela et al suggested that urban residence and AR were significantly associated with lower long-term improvement after RFA. 19
Bipolar microdebrider technique for ITH might have several potential advantages. Neri et al performed this procedure in 13 patients and studied the ultrastructural changes of mucosa taken from the inferior turbinate head after 4-month follow-up. A complete mucosal regeneration was observed, mucociliary transport time returned to normal range in all patients and VAS scale showed improvement. No negative impact on healing time or any adverse postoperative events has been reported. 20
Several studies showed that QMR treatment can be considered a safe and minimally invasive surgical procedure with the lowest mucosal damage, minor discomfort, and a low risk of side effects because it uses lower temperatures minimizing adverse effects. 21 The QMR is based on the fundamental principles of quantum theory: Any form of energy is transmitted from a source to a body in tiny discrete packets of energy that Max Planck called “energy elements” or Quanta. The mechanism of action is based on molecular bounds breaking: QMR generates frequencies that makes bounds resonate and break keeping the surrounding tissues at a low temperature (<45 °C). When a quantum of energy hits a tissue transmitting the same value of tissue’s bond energy, the bond breaks without increase of kinetic energy and therefore without increasing the temperature. QMR generator combines different frequencies, ranging between 4 and 16 MHz, to produce a particular effect: interruption of molecular cell binding resulting in an extremely selective break of the involved tissues which preserves from damage the surrounding healthy tissue. 22 The surgeon inserts a handle in the inferior turbinate through the submucosal tissue and obtains a safe tissue’s volumetric reduction without any burning effect. This leads to a restitutio ad integrum by primary intention, minimizing mucosal edema, and scars. 21
The literature showed conflicting results regarding patient satisfaction and the long-term outcome of the procedure. Currently, there is evidence that patient expectations of treatment outcomes are a crucial element in evaluating therapeutic outcomes and can provide very realistic feedback on the effectiveness of a treatment. For these reasons, our study evaluated treatment outcomes in terms of QoL. 23 -25
In QMR, long-term results were good in nonallergic group patients, while allergic patients showed a worse temporal trend, with evidence of recurrence between 3 and 12 months after treatment. Further studies should assess more precisely the timing of recurrence for allergic patients.
Quantic molecular resonance treatment is an outpatient procedure that can be performed under minimally invasive local anesthesia, and it is a rapid (about 10 minutes of treatment) and accurate technique (the wound is extremely localized with minimal effects on the surrounding tissues). If necessary, this procedure can be repeated, and the rate of postoperative complications such as pain, early and late bleeding, synechiae, scabs, infections, and nasal dryness is substantially minimal.
Limits of This Study
This preliminary study has several limits. The main limitation is that we did not include a control group, and the study did not involve treatment randomization. Secondly, the small cohort of patients enrolled may have influenced the statistical power of our analysis. More research is needed to confirm the effectiveness of QMR in the treatment of ITH in allergic and non-AR refractory to medical therapy.
Conclusions
Our data indicate that QMR treatment is a successful therapeutic option for nasal airway obstruction due to ITH. It offers a very good long-term results in nonallergic group of patients with a substantially minimal rate of postoperative complications. However, larger prospective studies with control arms are needed to validate these preliminary results.
Supplemental Material
Supplemental Material, sj-pdf-1-ear-10.1177_01455613211001599 - The Role of Quantic Molecular Resonance (QMR) in the Treatment of Inferior Turbinate Hypertrophy (ITH): Our Experience With Long-Term Follow-Up in Allergic and Nonallergic Rhinitis Refractory to Medical Therapy. Preliminary Results
Supplemental Material, sj-pdf-1-ear-10.1177_01455613211001599 for The Role of Quantic Molecular Resonance (QMR) in the Treatment of Inferior Turbinate Hypertrophy (ITH): Our Experience With Long-Term Follow-Up in Allergic and Nonallergic Rhinitis Refractory to Medical Therapy. Preliminary Results by Filippo Ricciardiello, Davide Pisani, Pasquale Viola, Raul Pellini, Giuseppe Russo, Giuseppe Longo, Giuseppe Chiarella, Flavia Oliva, Domenico Romano, Gerardo Petruzzi and Salvatore Mazzone in Ear, Nose & Throat Journal
Footnotes
Authors’ Note
The work is compliant with ethical standards and has been ethical approved by the commission of the Hospital AORN Cardarelli.
Acknowledgment
The authors wish to acknowledge the help provided by Maria Concetta Marzullo for translation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.