
Abstract
This study investigated the etiology and treatment outcome in sudden sensorineural hearing loss (SSHL) patients following dental procedure. During the past 2 decades, only 6 patients with SSHL following dental procedure were experienced including tooth extraction in 5 and endodontic treatment in 1. Three were males and 3 were females, with ages ranging from 10 to 75 years (median, 47 years). All patients underwent an inner ear test battery. Types of audiogram consisted of total deafness in 3 ears, flat-type loss in 2 ears, and high-tone loss in 1 ear. The pretreatment mean hearing level from 4 frequencies was 76 ± 37 dB for the lesion ears, significantly higher than 23 ± 15 dB for the opposite healthy ears. The treatment outcome is unsatisfactory. Five patients remained hearing unchanged 3 months after treatment. Only 1 (17%) patient had hearing improvement who was proved as having reactivation of the varicella-zoster virus. In conclusion, reactivation of the varicella-zoster virus may be one of the etiologies for SSHL patients following dental procedure. Serological assay coupled with MR imaging may help identify the etiology, determine the medication, and predict the outcome.
Keywords
Introduction
Sudden sensorineural hearing loss (SSHL), also termed sudden deafness (SD), is a syndrome that comprises various entities and results from a variety of etiologies of either primary or secondary origin. 1 -3 Proposed etiologies of primary SD comprised viral infection, vascular insufficiency, autoimmune disorder and stress theory, while causes of secondary SSHL include neoplasm, stroke, and irradiation. 4 -8 Farrell et al 9 first reported 4 cases of SSHL after dental surgery. Thereafter, sporadic SSHL cases related to dental procedures, that is, tooth extraction, endodontic treatment, anesthetic reagents, and so on, have been reported in the literature. 10 -12 Many hypotheses have thus been proposed, namely, infection, anesthetic reagents, vasospasm of internal auditory artery from autonomic dysfunction, or wide opening of the jaw results in stretching/crushing the vertebral artery that releases microemboli. 13 Nevertheless, lack of solid evidence remains most concern, likely because such cases are occasionally encountered at an otolaryngological clinic. Tracing back to the past 2 decades at our university hospital, only 6 cases of SSHL after dental procedure were experienced. Hence, detailed history taking coupled with a battery of testing in individual cases may help unravel the mystery of SSHL following dental procedure.
Methods
During the past 2 decades from 2000 to 2020, totaling 951 SSHL patients visited the otolaryngological clinic of the university hospital. Of them, 6 (0.6%) patients with unilateral SSHL following dental procedures were enrolled in this study, including tooth extraction in 5 patients and endodontic treatment in 1 patient. The SSHL is defined as a rapid decline (<3 days) of more than 30 dB sensorineural hearing loss in at least 3 contiguous frequencies without identifiable cause. 3
Three were males and 3 were females, with ages ranging from 10 to 75 years (median, 47 years). Right and left ears were equally affected (Table 1). The interval between dental procedure and onset of SSHL ranged 0 to 3 days (mean, 1 day), while that between onset of SSHL and treatment was within 7 days. Those with middle/inner ear anomaly or infection, ototoxicity, bilateral SSHL, and posterior fossa tumor/stroke were excluded.
Clinical Information of 6 Patients With Sudden Sensorineural Hearing Loss After Dental Procedure.

Each patient received otoscopic examination, blood examination, image study, audiometry, and caloric test. Cervical and ocular vestibular-evoked myogenic potential (cVEMP and oVEMP) tests were added to the test battery after 2000 and 2008, respectively.
Ethics Statement
This study was approved by the institutional review board of the university hospital, and each patient signed the informed consent to participate.
Audiometry
The mean hearing level (MHL) was defined as averaged hearing threshold at 4 frequencies of 500, 1000, 2000, and 3000 Hz. Mean hearing gain measures the difference between the pretreatment MHL and posttreatment MHL after 3-month treatment. Outcome of the treatment was defined as: complete recovery (MHL within 20 dB), improvement (mean hearing gain >10 dB), and unchanged (mean hearing gain ≤10 dB). Improved rate consisted of those with complete recovery and improvement.
Vestibular Test Battery
Bithermal caloric test was conducted with an electronystagmographic recorder. Canal paresis is defined when mean slow phase velocity (SPV) of caloric nystagmus in the lesion ear is <7 °/s, or as a greater than 25% difference between maximum SPV measurements for each ear, when compared with the sum of SPVs from each ear.
For the oVEMP and cVEMP tests, the detailed procedure was described elsewhere. 14 Briefly, the operator held a vibrator by hand with the initial peak driving voltage about 144 dB force level and delivered repeatable taps on the forehead to elicit oVEMP. For the cVEMP test, the operator delivered repeatable taps on the occiput via the same vibrator. The supine subject elevated the head to keep a background muscle activity at 50 to 200 µV. A total of 50 responses were averaged and recorded bilaterally.
Results
Clinical manifestation comprised hearing loss and tinnitus in all 6 patients, followed by vertigo in 3, nausea/vomiting in 3, and fullness sensation in 1 (Table 1). Types of audiogram consisted of total deafness in 3 ears, flat-type loss in 2 ears, and high-tone loss in 1 ear (Table 2). The pretreatment MHL from 4 frequencies was 76 ± 37 dB for the lesion ears, significantly higher than 23 ± 15 dB for the opposite healthy ears (P < .05, paired t test). Since the cVEMP and oVEMP tests were added to the test battery after 2000 and 2008, respectively, the cVEMP, oVEMP, and caloric tests in some patients revealed 67% (2/3), 67% (2/3), and 75% (3/4) abnormality rates, respectively (Table 2). Serological assay was performed in 3 patients and 1 patient showed increased IgM antibody titer of varicella-zoster virus (Table 1). After 3-month treatment, posttreatment MHL (67 ± 38 dB) did not significantly differ from pretreatment one (P > .05, Table 2), indicating that the treatment outcome is unsatisfactory. Five patients remained hearing unchanged, and only 1 (17%) patient had hearing improvement. Herein, we present this case.
Audiovestibular Testing of 6 Patients With Sudden Sensorineural Hearing Loss After Dental Procedure.a
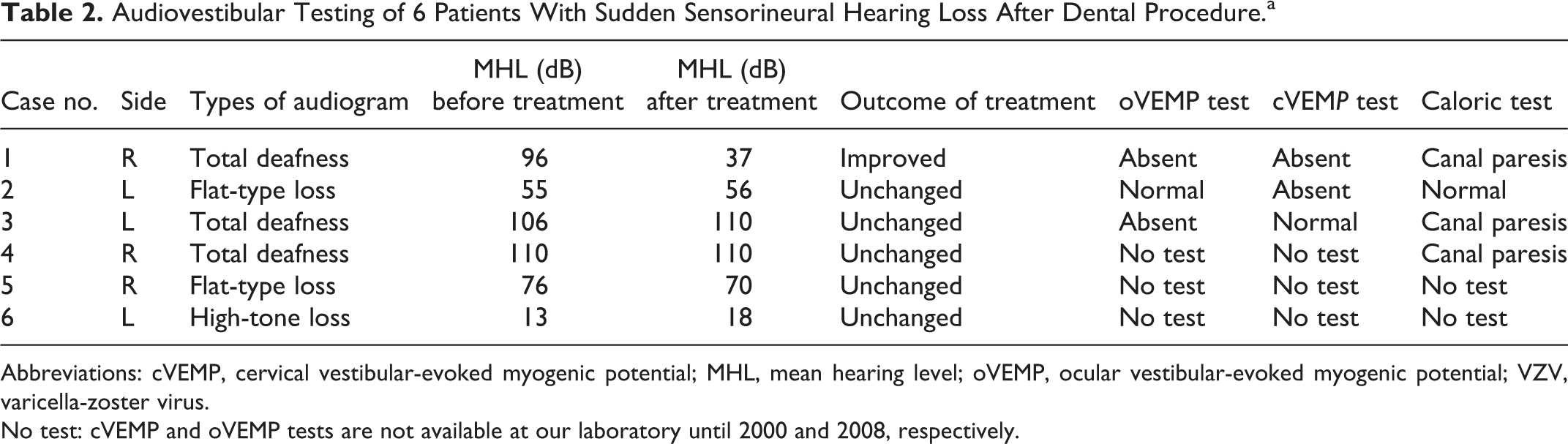
Abbreviations: cVEMP, cervical vestibular-evoked myogenic potential; MHL, mean hearing level; oVEMP, ocular vestibular-evoked myogenic potential; VZV, varicella-zoster virus.
No test: cVEMP and oVEMP tests are not available at our laboratory until 2000 and 2008, respectively.
Case Presentation (Case No. 1)
A 31-year-old female had intractable periodontal disease for 1 year. She received endodontic treatment for 12 teeth including right and left, upper and lower molar teeth on June 28, 2020. Unfortunately, severe vertigo with nausea and vomiting occurred on the next morning, and she was sent to the emergent service, where hearing impairment on her right ear was noted. She was then referred to our hospital.
At admission, the patient was in ill appearance with spontaneous nystagmus beating toward the left side. She denied any ear disorder previously. Neither systemic disease, that is, hypertension, diabetes mellitus, or coronary artery disease, nor autoimmune disorder was experienced. Local checkup of the ears, nose, and throat did not identify any eruption or vesicle formation. Facial nerve function is essentially normal. Audiometry showed profound deafness with MHL of 96 dB on the right ear (Figure 1), while normal hearing on the left ear. For the vestibular test battery comprising cVEMP, oVEMP, and caloric tests, all revealed absent responses on the right ear (Figure 2) and normal responses on the left ear.
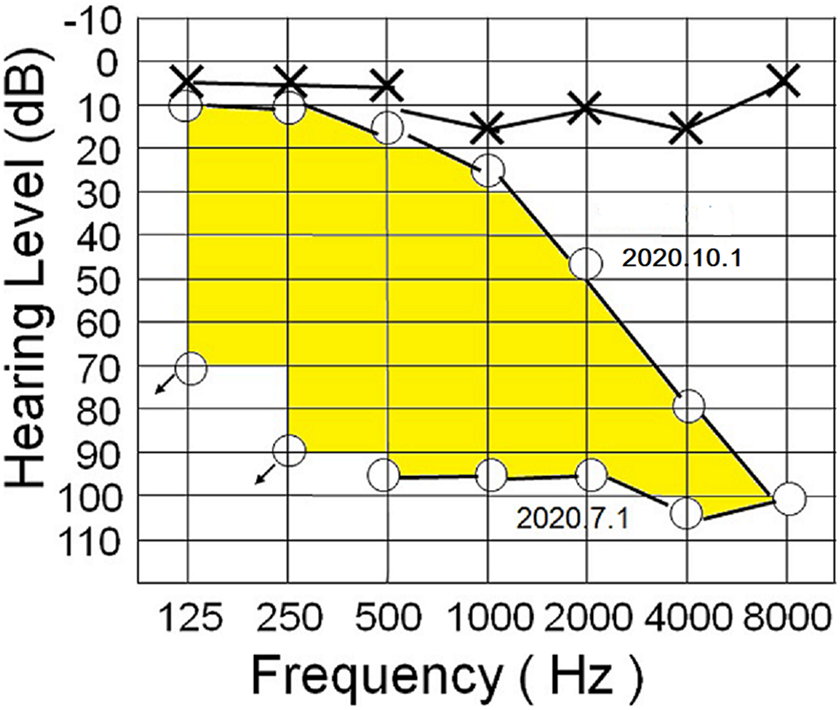
Female aged 31 years, case no. 1. Audiometry reveals profound sensorineural hearing loss on the right ear, with mean hearing level of 96 dB. Three months after treatment, marked improvement of the hearing (shaded area) is identified, with mean hearing level of 37dB.
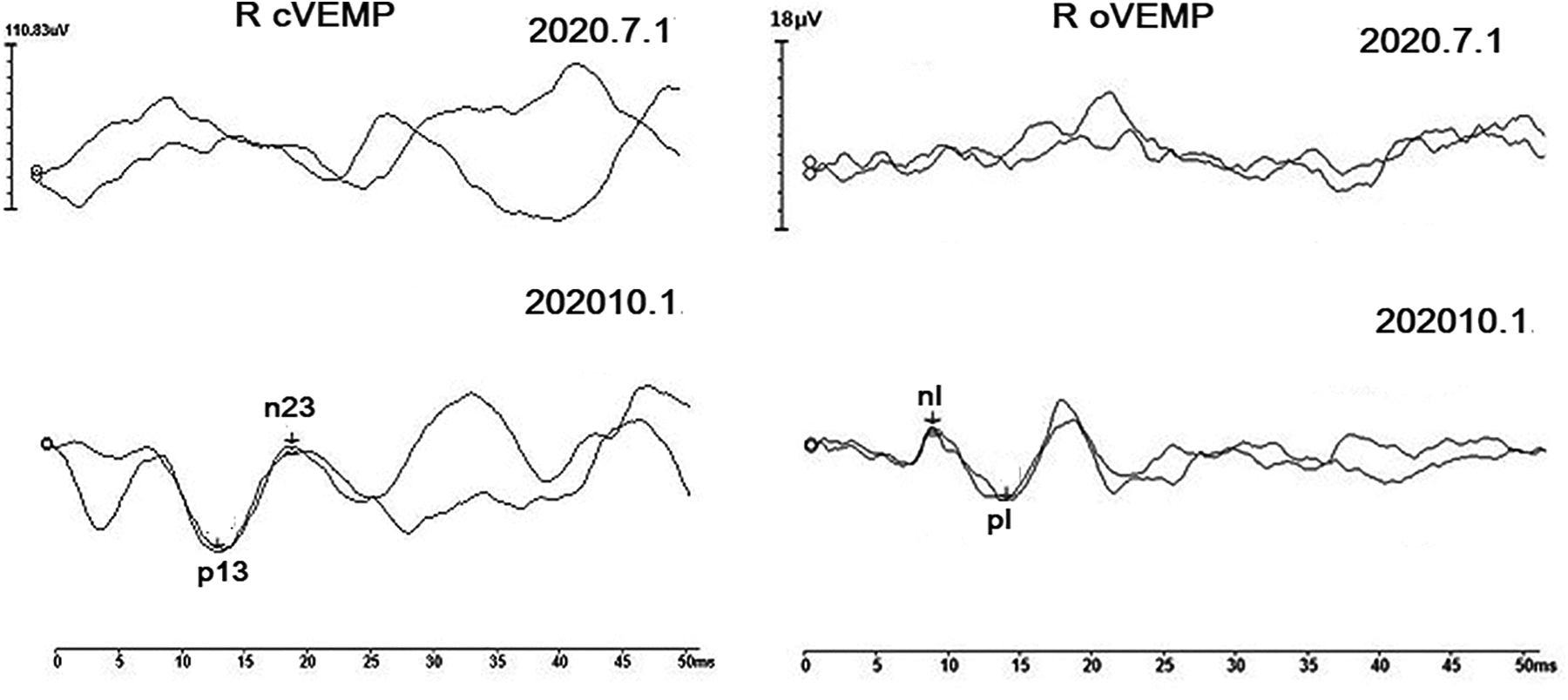
Case no. 1. Right ear. Absent cVEMP and oVEMP responses before treatment (July 1, 2020) have resolved and returned to normal cVEMP and oVEMP responses 3 months after treatment (October 1, 2020). cVEMP indicates cervical vestibular-evoked myogenic potential; oVEMP, ocular vestibular-evoked myogenic potential.
Subsequently, serological assay identified increased IgM antibody titer of varicella-zoster virus. However, MR imaging with gadolinium enhancement (Figure 3A) failed to demonstrate any obvious abnormality in the internal auditory canal (IAC). She was then treated with antiviral agent (valacyclovir 1 g, twice daily for 1 week) coupled with oral prednisolone (60 mg daily for 1 week then tapered in 1 week), followed by antioxidant (acetylcysteine 600 mg, bid) for 8 weeks. 15
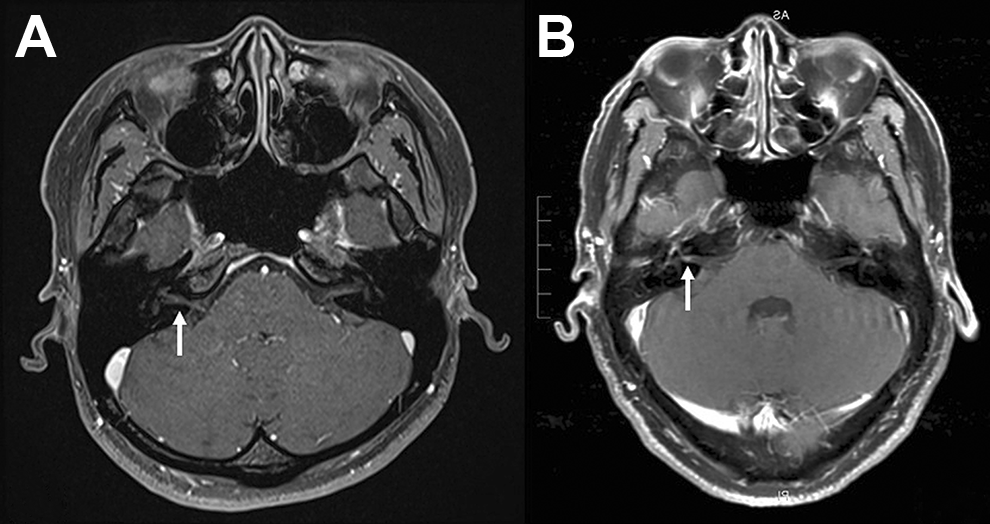
A, Case no. 1. MR image with gadolinium enhancement demonstrates no obvious abnormality in the internal auditory canal of the right ear (arrow). B, MR imaging in a 43-year-old male with herpes zoster oticus of the right ear. A linear gadolinium-enhanced lesion in the internal auditory canal (arrow) is demonstrated.
Three months after treatment, follow-up audiometry showed marked improvement of hearing, with the MHL of 37 dB on the right ear (Figure 1). Additionally, all absent responses of the cVEMP, oVEMP, and caloric tests on the lesion ear have resolved and returned to normal responses (Figure 2).
Discussion
In the presented case, profound deafness on the right ear accompanied by spontaneous nystagmus beating to the left side favors a diagnosis of SSHL rather than Meniere disease since the latter rarely exhibits profound deafness at an initial stage. An inner ear test battery including audiometry, cVEMP, oVEMP, and caloric tests, revealed abnormal responses on the lesion ear (Figures 1 and 2), indicating that the respective inner ear end organs, that is, cochlea, saccule, utricle, and semicircular canals were substantially affected. 16 Since vascular insufficiency and autoimmune disease are less relevant in young adults, viral infection may play a dominant role for precipitating SSHL in young adults after dental procedure. Serological assay identified increased varicella-zoster virus IgM antibody titers, further confirmed that SSHL following dental procedure in this young adult is caused by reactivation of the varicella-zoster virus.
Molecular temporal bone histopathological study suggested that latent varicella-zoster virus is located in the geniculate ganglion and may be present in the spiral and/or Scarpa ganglia. 17,18 It is reasonable to presume that SSHL in case no. 1 arises from reactivation of latent varicella-zoster virus in the spiral and/or Scarpa ganglia, rather than the geniculate ganglion, in view of the presence of deafness and vertigo without facial paresis.
However, MR imaging failed to demonstrate any obvious enhancement in the IAC. Neither increased permeability of contrast media nor inflammatory nerve edema in the IAC was demonstrated (Figure 3A), which is opposed to the concept that the varicella-zoster virus may break down the blood-labyrinth barrier and increase the permeability of contrast media. 19,20
To verify the concept, another 43-year-old male patient with herpes zoster oticus, manifested by eruption, facial paresis, and hearing loss on the right ear, was adopted for comparison. 16 Serological assay confirmed the reactivation of varicella-zoster virus, and MR imaging demonstrated a linear gadolinium-enhanced lesion in the IAC of the right ear (Figure 3B). Although recovery of facial nerve function was identified, hearing loss on the right ear remained unchanged despite treatment. One possible reason is that virulence of the varicella-zoster virus in case no. 1 is not so great enough to break down the blood-labyrinth barrier, thus contrast leakage is not identified in MR imaging. Restated, lack of contrast enhancement in the IAC of an SSHL patient from varicella-zoster virus infection may imply a fair outcome of hearing, as evidenced by marked improvement of the hearing (Figure 1) and recovery of vestibular function (Figure 2) after treatment.
Conclusion
Reactivation of the varicella-zoster virus may be one of the etiologies for SSHL patients following dental procedure. Serological assay coupled with MR imaging may help identify the etiology, determine the medication, and predict the outcome.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Science Council, Taiwan (Grant no. Most 109-2314-B-002-265) and Good Liver Foundation (Grant no. 109-039).