
Abstract
The larynx is an uncommon location for live foreign bodies. The leech can reach the glottis during consumption of contaminated water but is usually expelled by an effective cough reflex. Patients present with hoarseness and dysphagia and occasionally with dyspnea or hemoptysis. Endoscopically, a mobile mass is usually noted in the supraglottic area. We present a rare case of a laryngeal leech in a 62-year-old-male farmer who lives in a rural area. The leech was removed successfully with direct laryngoscopy under general anesthesia.
Case Description
A 62-year-old male was referred to our ear, nose, and throat (ENT) department with a 7-day history of hemoptysis, hoarseness, and sore throat. He received antibiotics on a presumptive diagnosis of acute laryngitis by his general practitioner without improvement. His past medical history was otherwise unremarkable. The patient was a farmer in rural area and he admitted to drinking water from a local stream regularly.
Flexible fiberoptic endoscopy revealed a moving dark-colored foreign body on the supraglottic area in the vicinity of the anterior commissure (Figure 1). Signs of inflammation were also noted in the area. Vocal folds mobility was normal. A full ENT examination did not reveal any abnormal findings. The possibility of a laryngeal leech was raised and the patient was taken to theater for direct laryngoscopy under general anesthesia.
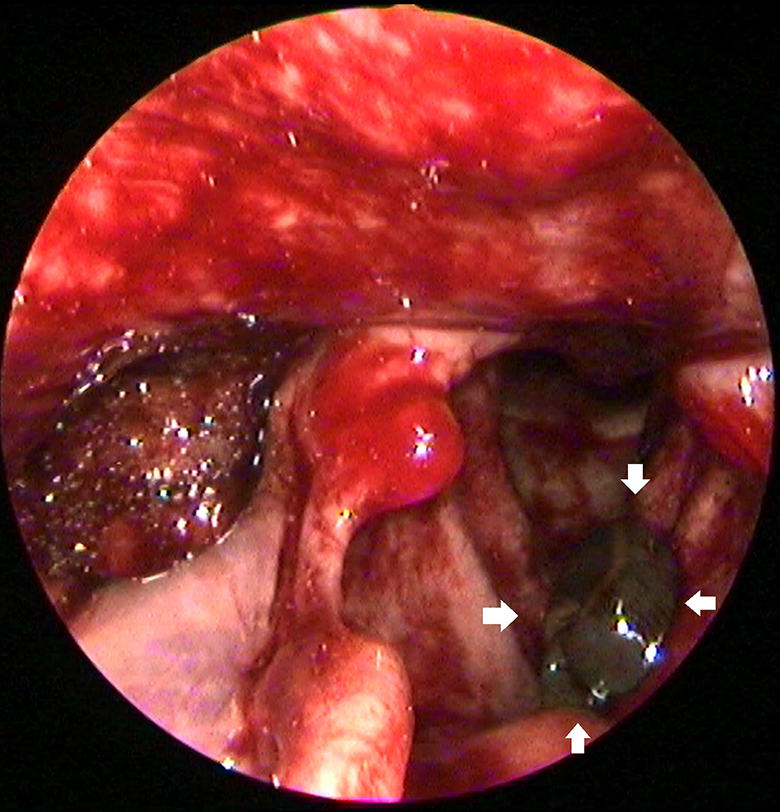
Laryngoscopic view of a dark-colored worm-like foreign body in the supraglottic area (white arrows). Intraoperatively, the leech moved and so our clinical suspicion was confirmed. Diffuse hyperemia of the larynx is also noted.
Our initial suspicion was, indeed, confirmed. The leech was fairly unresponsive to touch but still alive (Figure 1). We presumed this to be the result of sevoflurane inhalation by the leech, and therefore, we did not use any cautery to kill it. The 4-cm-long leech was grasped with forceps and removed in its entirety (Figure 2). Meticulous inspection of the entire laryngeal area did not reveal any abnormal findings. The patient had an uneventful recovery and was discharged the next day (Figure 3). He was advised to abstain from drinking natural stream water.

The extracted leech is still alive.
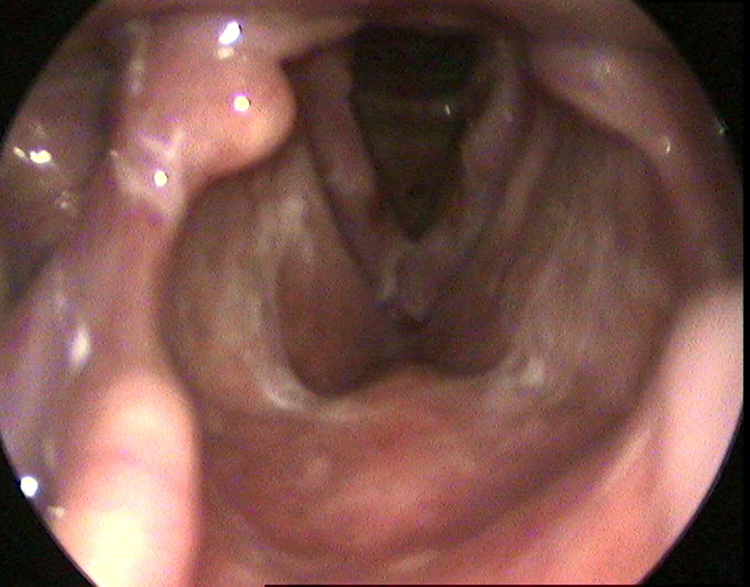
Postoperative laryngoscopic view with no evidence of foreign body or edema. Hyperemia has fully regressed.
Discussion
Leeches are endoparasites living in contaminated waters feed by sucking blood from the skin and mucosal surface of mammalian species. The most common infection route is the consumption of contaminated water either by voluntarily ingestion or unintentionally, during swimming in contaminated water in rural areas.1-3 Leeches adhere to the host’s mucosa and suck large quantities of blood. 2 The process does not cause any pain to the host as a result of the anesthetic properties of the leeches’ own saliva, rendering hosts unaware of their presence. 4
The location and duration of leeches
The treatment of choice for laryngeal leeches is removal under general anesthesia with sevoflurane for induction. It is crucial to remove the parasite in a single piece. If the head of the leech remains in the mucosa, hirudin enzyme may still be active leading to blood loss and subsequent anemia. To that end, the leech is first anesthetized with sevoflurane and then removed gently from a hypopharyngeal or laryngeal location avoiding trauma or mucosal edema. Lidocaine can also be used to relax the head suckers and substantially facilitates removal.9-11 The last maneuver of the procedure should be a meticulous inspection of the entire laryngeal region.
In certain rural areas, habitants still consume water from springs despite full access to safe drinking water. Therefore, a leech infection should be considered in cases of unexplained anemia, hemoptysis, or hoarseness. Direct laryngoscopy under general anesthesia is warranted to remove the parasite safely.
Footnotes
Authors’ Note
The authors declare that written informed consent for patient information and images to be published was provided by the patient.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.