
Abstract
We describe a case of spontaneous nasal septal abscess (NSA) in a 9-year-old child. We also reviewed the literatures in recent years and summarized the characteristics of NSA, such as gender, age, inducement, pathogenic bacteria, treatment, and prognosis. We found that this boy reported by us has the most extensive abscess. May be the delay of treatment was related to the recent fluctuation of COVID-19 epidemic in China. Fortunately, with the help of surgery and anti-infection treatment, the boy was discharged from the hospital without septal perforation or saddle nose.
Case Report
A 9-year-old boy presented to the ENT outpatient department on January 14, 2021, with a 7-day history of nasal pain and bilateral progressive nasal obstruction. He denied any history of trauma, aspirated foreign bodies, nasal surgery, chronic rhinosinusitis, diabetes, tuberculosis, and any other associated diseases. His symptoms always set on without complications such as rhinorrhea, headache, and conscious fever. The only suspected trigger was a habit of nose picking. Rhinoscopy revealed a swollen and mildly erythematous nasal bridge, with bilateral tender and fluctuant masses obstructing the nasal cavity (Figure 1). The surrounding tissue showed no signs of cellulitis. He did not feel fever, but his temperature measured 39.3 °C. The remainder of the physical examination was normal. Given a suspect of nasal septal abscess (NSA), computed tomography (CT), and magnetic resonance imaging (MRI) were urgently ordered. The nasal septum demonstrated a patchy low-density shadow in CT, and slightly hypointense T1 signals and iso T2 signals in MRI (Figure 2). There was no evidence of paranasal sinuses or intracranial extension.
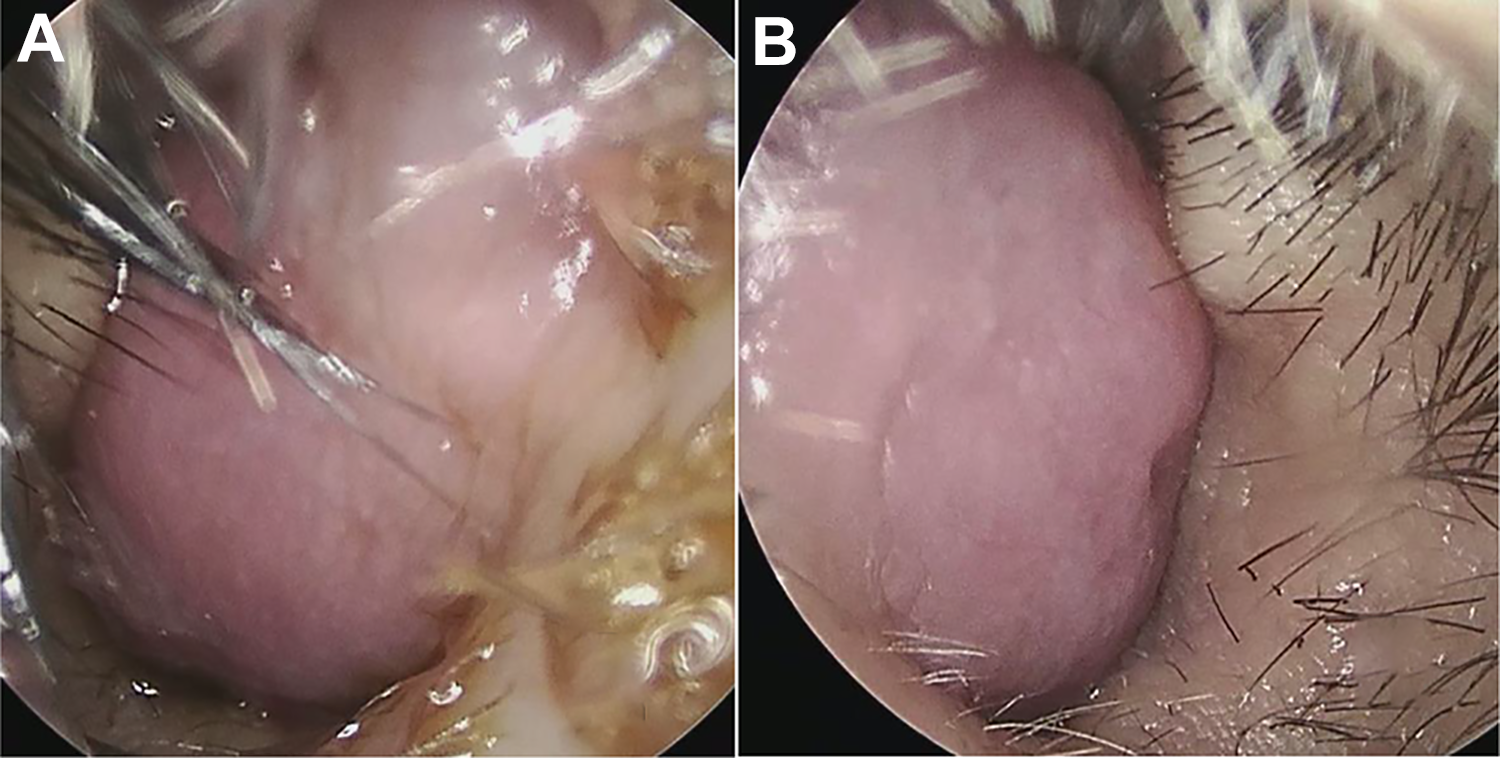
Rhinoscopy revealed a swollen, mildly erythematous nasal bridge with bilateral masses obstructing the nasal cavity. A, Right cavity. B, Left cavity.
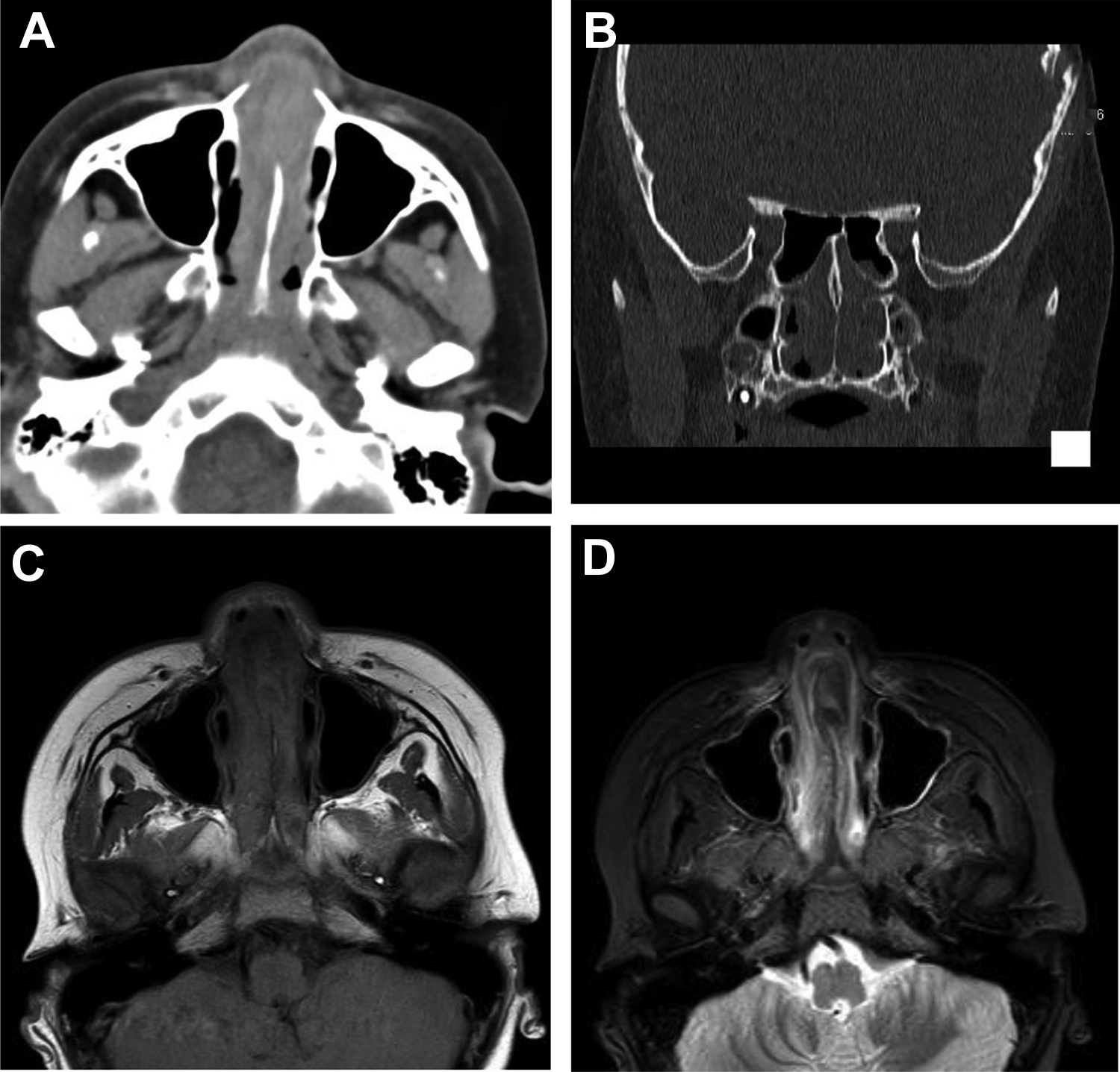
The nasal septum demonstrated a patchy low-density shadow in computed tomography (CT) (A, B), and slightly hypointense T1 signals (C) and iso T2 signals (D) in magnetic resonance imaging (MRI).
The patient was admitted to the ENT inpatient department with an initial diagnosis of septal abscess. Before surgery, white blood cell count was 17.41 × 109/L, percentage of neutrophils was 85.6%, C-reactive protein was 123.61 mg/L, heparin-binding protein was 40.96 ng/mL, percentage prothrombin time was 57%, fibrinogen concentration was 5.65 g/L, and electrocardiogram and chest CT were normal. We subsequently performed an incision and drainage of the abscess under general anesthesia at night after admission. A left vertical hemitransfixion incision was made. A lot of purulent fluid was aspirated and sent for microscopy and culture. Intraoperatively, we found blood clots between cartilage and perichondrium, and a wide-range swelling builtup on both sides of the nasal septum, from the columella to the anterior wall of the sphenoid sinus, and from the dorsum to the base of the nose. The wide necrotic nasal septum mucosa and anterior cartilage were completely removed. The abscess cavity was irrigated repeatedly with hydrogen peroxide, iodophor dilution, and physiological brine, then the nasal cavity was filled with NasoPore.
After surgery, anti-infection treatment with cefotaxime sodium was given, and examinations were continued. Some laboratory results were remarkable, including immunoglobulin M (0.28g/L), C4 (0.444g/L), and creatinine (30.7 μmol/L). Although immunoglobulin A, immunoglobulin G, C3, rheumatoid factor, antistreptococcal hemolysin, blood glucose, glycated hemoglobin, hepatitis B, hepatitis C, HIV, and COVID-19 remained normal. The patient’s temperature dropped to 37.5 °C on the first day after surgery and to normal hereafter. Staphylococcus aureus was cultured and the antibiotics was changed to cefazolin. The patient was thus discharged upon 12-day inpatient treatment. The abscess has completely resolved without septal perforation or saddle nose.
Discussion
This is the first childhood spontaneous NSA, an extremely rare disease, encountered in our department in recent years. In this case, the abscess involved a wide range. Nasal septal abscess always develops as hematoma is induced by nasal trauma or septal surgery and becomes infected. 1 Besides, NSA can also appear as a complication of sinusitis, nasal furunculosis, dental infections, amoebiasis, tuberculosis, orbital cellulitis, and even radiofrequency cauterization for epistaxis.2-9 Patients with diabetes, especially poorly controlled diabetes, face a greater risk of NSA after nasal septoplasty. 10 The main clinical manifestations of septal abscess include progressive nasal pain, nasal obstruction, and fever. Once diagnosed, early treatment should be recommended. Any delay may result in septal perforation, saddle nose, or even serious complications, such as meningitis, orbital cellulitis, and thrombophlebitis of cavernous sinus.1,2,4,11 Abscess is mostly caused by infections by Staphylococcus, methicillin-resistant Staphylococcus aureus, Streptococcus vitifolia, Klebsiella pneumococcus, or Haemophilus influenzae, and occasionally by amoeba and other aseptic factors.3,5,12-14 Incision and drainage of abscess are required initially, followed by sensitive antibiotics selected according to the results of bacterial culture. For patients with a large necrotic defect in nasal septum cartilage or the formation of saddle nose, nasal septum should be reconstructed with autogenous tragus cartilage or costal cartilage.7,15
In this case, we suspected that during nose picking, the nasal septum was wounded, coagulation abnormalized, hematoma formed, and infection aggravated. We summarized the data in literature about NSA, such as gender, age, inducements, pathogenic bacteria, treatment, and prognosis (Table 1). We found that NSA can occur in different races and at different ages. Nasal septal abscess displays a male predominance and a good prognosis in children. Adults are prone to saddle nose. By comparison, the extension of abscess in this boy was the largest reported by far. Fortunately, our surgery and anti-infection treatment achieved a recovery without septal perforation or saddle nose.
Summary of Recent Literature on Septal Abscess.
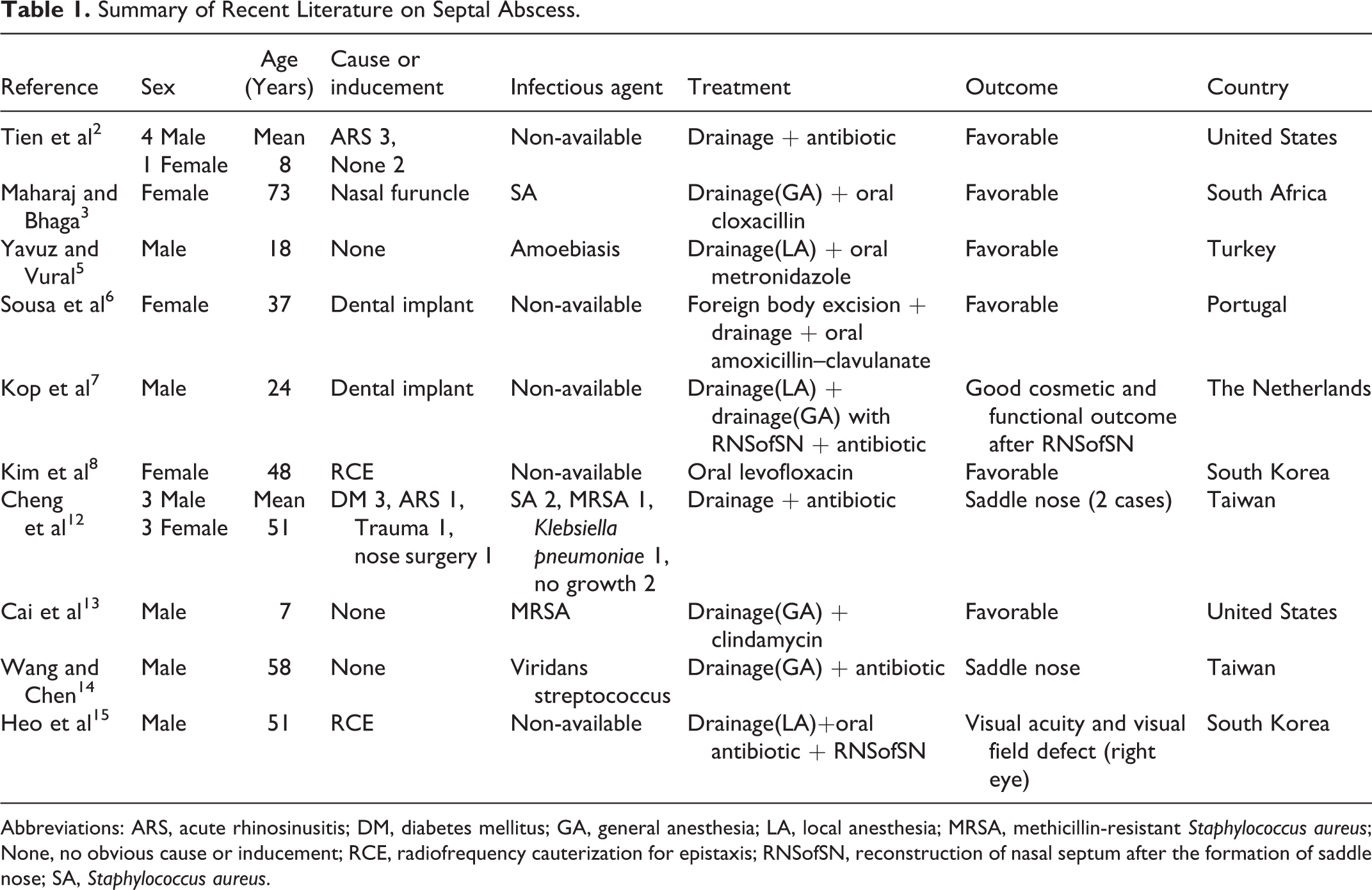
Abbreviations: ARS, acute rhinosinusitis; DM, diabetes mellitus; GA, general anesthesia; LA, local anesthesia; MRSA, methicillin-resistant Staphylococcus aureus; None, no obvious cause or inducement; RCE, radiofrequency cauterization for epistaxis; RNSofSN, reconstruction of nasal septum after the formation of saddle nose; SA, Staphylococcus aureus.
Footnotes
Authors’ Note
J.L. is the first author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.