
Abstract
Bonebridge (BB) is the first active implantation system for bone conduction that is placed fully under the skin. Experience suggests that BB is characterized by low incidence of postoperative complications. This case report presents a rare case of a 16-year-old girl with incidence of emphysema occurring over the implant 1 year after operation. We performed a computed tomography scan that showed pockets of gas above the floating mass transducer so we provided the revision surgery and sealed the artificial opening with fat from the earlobe and fibrin glue. Since that time, no air has collected in the retroauricular area and the implant has been fully functional.
Introduction
Bonebridge (BB; MED-EL) is an implantation system for bone conduction enabling direct transfer of sound to the inner ear through the bones of the skull. It is composed of an external audio processor worn behind the ear and an implant bone conduction-floating mass transducer (BC-FMT) placed under the skin into the bone behind the ear. The 2 parts are connected by a magnet. The audio processor converts sound to electrical signals that are transformed into mechanical vibrations by the implant and transferred through the bone to the inner ear. Bonebridge is available for adults and children from 5 years of age. The main indications are conductive or mixed hearing impairment and one-sided deafness. Suitable anatomic predisposition is a prerequisite for successful operation. Prior to implantation, the patient should have worn another hearing aid with positive effect. For children, informed consent from a legal guardian is also required. 1,2
The first BB implantation was done in 2011 by Dr Georg Mathias Sprinzl at the ORL clinic in Sankt Pölten, Austria. 1 In general, very few post-implantation complications are known and these have consisted primarily in minimal incidence of skin reactions. Users also report not having problems with pain caused by pressure. The BB gives patients good hearing results and improved quality of life. 3 -7
Case Report
A 16-year-old girl with congenital microtia and atresia of the outer right ear canal was admitted to our clinic for implantation of the BB system. The patient was of a slender build with a rather low weight of 44 kg (body mass index [BMI]: 16.7). She had been monitored since childhood for conductive hearing impairment of the right ear. Before BB implantation, sound-field audiometry was conducted at 35, 35, 55, 55, and 55 dB (at frequencies of 0.5, 1, 2, 3, and 4 Hz) and speech audiometry with an SRT (speech reception threshold) of 52 dB with the masking of healthy ear. The girl previously had used no hearing aid. At 16 years of age, she was offered through our speech therapy department to try an ADHEAR bone conduction system (MedEl). She was very satisfied with this hearing aid. The aid gave her subjectively better intelligibility in noise and directional listening, as had been demonstrated also by various studies. 8 Sound field audiometry with the ADHEAR was conducted at 20, 5, 15, 25, and 35 dB and speech audiometry with an SRT of 20 dB with the masking of healthy ear. Having fulfilled all indication criteria, the girl was selected by the indication commission as a suitable candidate for allocation of a BB active bone conduction system.
The operation was completed without complications. We performed a modified retroauricular incision, uncovering of the planum mastoideum, shaping of the socket, and placement of the BC-FMT with fixation and suture of the periosteum, subdermis, and skin. The scar behind the right ear healed well. The girl was discharged to home care on the sixth day after operation and advised to rest and prevent exposing the incision to water. The girl exhibited no issues during an outpatient checkup 14 days after operation, and the processor was successfully connected and paired with the bone conduction implant 1 month after operation. Sound field audiometry was conducted with the BB at 15, 20, 30, 32, and 25 dB and speech audiometry with an SRT of 18 dB with the masking of healthy ear. At another checkup after 6 months, the girl was overall very satisfied with both her single-sided hearing and verbal audiometry.
One year after the operation, the girl came to the department complaining of a soft resistance behind her right ear (Figure 1), increasing during the Valsalva maneuver, and especially when blowing her nose. Communication through the aditus ad antrum and mastoid around the BC-FMT to the subcutis was suspected. We performed a computed tomography scan that showed pockets of gas above the BC-FMT suspected to communicate with one another (Figures 2 and 3). We then conducted a surgical examination. We first removed air bubbles from the pocket by suction and then made a retroauricular incision to expose the implant. An interstice between the BC-FMT and bone socket was apparent around the full circumference (Figure 4). We sealed the artificial opening with fat from the earlobe and fibrin glue. The fat was pushed to covering the interstice between the BC-FMT and bone socket and into the mastoid air cells through the interstice. Postoperative healing was slightly complicated due to a small, painful hematoma behind the ear with seepage around the wound. Antibiotics (second generation cephalosporins, 500 mg in a dosage of 1 tablet every 12 hours) were therefore administered. We instructed the patient not to blowing her nose and to prohibit Valsalva maneuver. The girl was released on the sixth day after operation. The cut healed without complications (Figure 5). Since that time, no air has collected in the retroauricular area and the implant has been fully functional (the follow-up period now is one year after revision surgery).
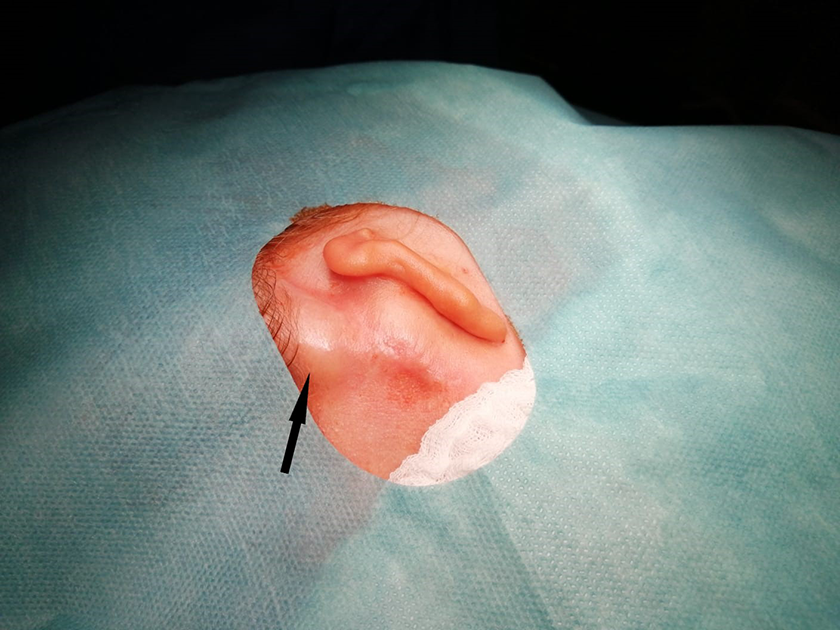
Retroauricular emphysema behind the right ear before revision surgery.
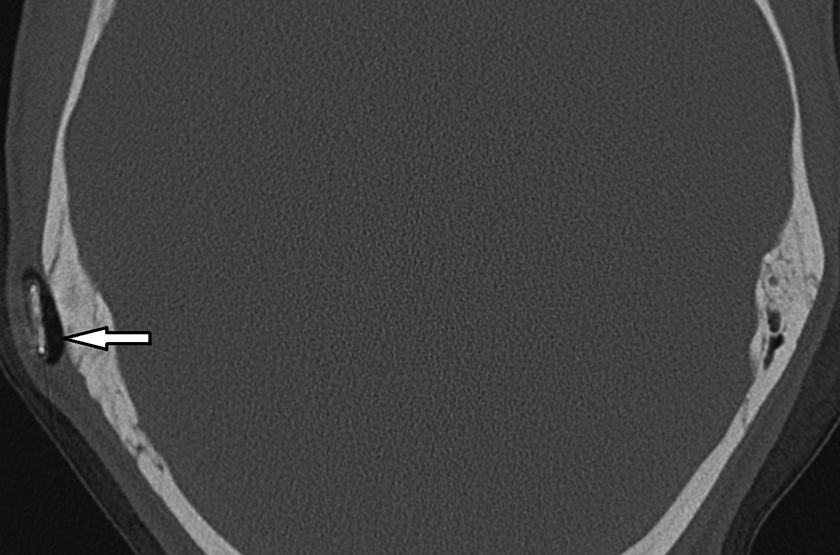
Retroauricular emphysema on the computed tomography (CT) scan, axial projection.
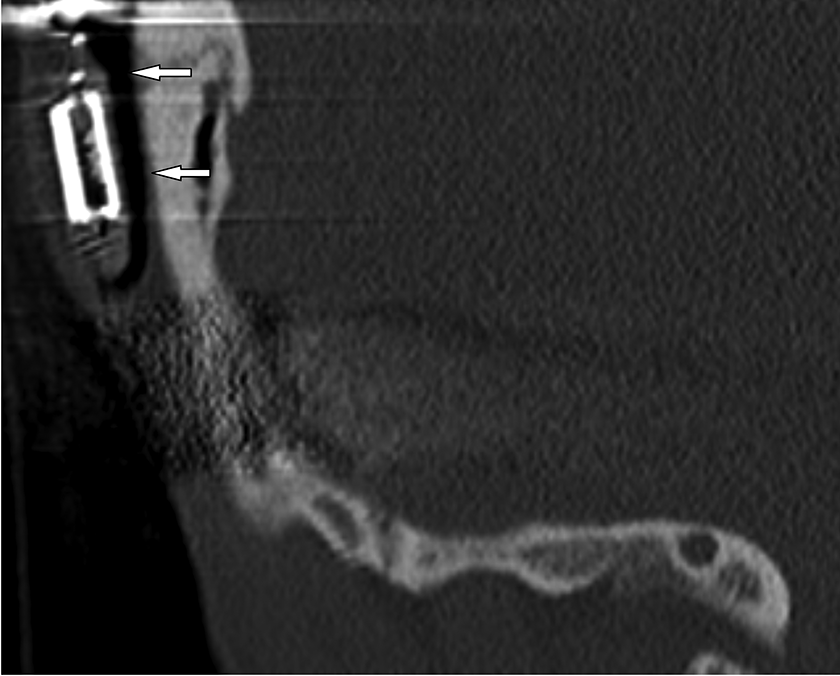
Retroauricular emphysema on the computed tomography (CT) scan, sagittal projection.
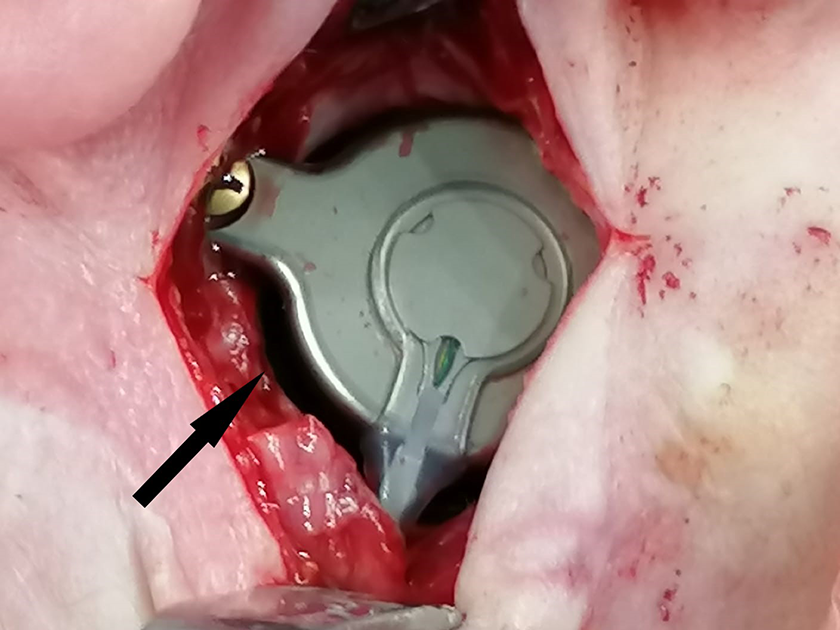
Interstice between bone conduction-floating mass transducer (BC-FMT) and bone pocket.

Retroauricular area after revision surgery.
Discussion
The BB implant is an active system for bone conduction based on the concept of fully integrating the vibrating element into the bone under the skin. It constitutes a modern and very effective treatment, eliminating certain deficiencies of previous BAHD (bone-anchored hearing device) passive systems. 9,10 The advantages of the BB system are especially beneficial to patients for whom it is necessary to avoid having an opening in the skin or higher pressure on the skin (due to immunodeficiencies, severe psoriasis, work with a risk of infection, fragile skin with postoperative changes, and the like), as well as for child patients, in whose case the bones of the skull and skin covering are not sufficiently strong. 7,9 The BB has demonstrated lower incidence of skin complications in comparison with other BAHDs. 9,10 Postoperative pain also has been evaluated as relatively low. 11 Among our patients, satisfaction with the audiological benefit, comfort, and aesthetics of the BB is high and that corresponds with what is seen in the literature. 3 -7 The system also is well regarded for its low profile and aesthetic appearance of the processor, which is greatly appreciated especially by child patients. Most children also report very good results in communication and using the audio processor on a day-to-day basis, while parents especially appreciate the improvement in their children’s social interactions and speech development. 3,6,9
Despite the high levels of satisfaction among BB users, certain complications can occur. A study conducted at the ORL clinic in Vienna during 2012 to 2018 examined 64 patients and found that 6 (9.4%) had postoperative complications requiring examination. Explantation was performed for 5 of those patients (83.3%; for 3 patients due to inflammatory complications for embedding the implant into the radical cavity, which was created for the patient’s unsuitable anatomic proportions; for 1 patient due to dehiscence in the operation incision in connection with a previous BAHA implant; and for 1 patient due to unsatisfactory benefit attributed to implantation despite incomplete fulfillment of the indication criteria). The remaining 1 (16.6%) patient underwent reimplantation due to repeated head trauma that had damaged the implant. The results of the study thus indicate that complications occur primarily with patients who do not fulfill the anatomical or other implantation criteria or in the case of damage to the implant due to head injury. 12
For the sake of comparison, a study from Freiburg in 2013 reported no complications among the first 3 child patients to receive the implant, 3 and a study from Malaysia found no serious complications among 20 implant patients monitored during the period 2012 to 2016. 13
Our case highlights a rare complication occurring 1 year after operation. Given the incidence of an air sac above the implant, possible communication of the middle ear with the subdermis via the aditus ad antrum and mastoid must be considered. Our case shows that in the case of BB direct osteointegration of the FMT into the bone does not occur (as is generally known) and it is therefore necessary that the socket for the FMT not be too large. In our patient’s case, there was a clear connection between the occurrence of emphysema during the Valsalva maneuver and the dysfunctioning of the Eustachian tube, which was confirmed by an inflation–deflation test. Considering the patient’s very low body weight and BMI, we suppose that she experienced significant regression of the Ostmann’s pad of fat and developed a permanently patulous Eustachian tube (PET). Classical findings in PET are for example breath-synchronous movement of the tympanic membrane (in a patient with atresia not visible of course) or autophonia, which was not present in our patient (and there is no craniomandibular malformation). Air was thus able to reach the middle ear in a larger quantity through the constantly open auditory tube and from there to pass through the mastoid around the BC-FMT and into the subdermis. In case of such complication, differential diagnostics with subsequent revision should be performed by imaging method (for children, under full anesthesia). In our case, the complication was solved by forming a seal using autologous fatty tissue from the earlobe and fibrin glue. The solution has so far proven successful. If the effect were insufficient and the intermittent emphysema were to recur, we would then consider extracting the implant, cleaning the socket of fibrous tissue, and inserting a new implant with a bone paté lining and bone cement. We should note here the fact that it is expedient during implantation to collect bone paté resulting from drilling and then to use the grit to plug open mastoid cells at the base of the socket cut for the BC-FMT. Such procedure would restrict possible air flow from the mastoid to the subdermis.
Conclusion
The BB offers safe and effective long-term hearing rehabilitation. The BB is an active bone conduction system placed fully under the skin and is characterized by very low incidence of postoperative complications.
Those complications that do occur are not serious, and postoperative revisions are infrequent. Cases where the implant itself has failed have been reported in the event of head trauma. Careful selection of patients, especially with a view to comorbidity, fulfillment of the indication criteria, and proper surgical techniques are regarded as the most important factors for limiting postoperative complications. Among other factors, individual anatomical proportions, especially for child patients, and anamnesis of chronic middle ear inflammation must always be taken into consideration when planning implantation of the BB system. Although occurrence of emphysema around the implant is a possible complication, it is one that can be successfully resolved.
Footnotes
Declaration of Conflicting Interests
The author(s) declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for the research, authorship, and/or publication of this article was provided by the Masaryk University in Brno under grant MUNI/A/1118/2020.