
Abstract
The Bonebridge (BB) was the first active transcutaneous implantation system for bone conduction. The main indications are conductive or mixed hearing loss and single-sided deafness. Treacher-Collins syndrome (TCS) is a rare genetic disease that affects craniofacial development. The disorder results in deformations of facial structure including ear malformations, especially microtia and ear canal atresia. These patients suffer from conductive hearing loss. CT scans often show unfavorable temporal bone anatomy making placement of an implant difficult. For implantable hearing rehabilitation, patients may decide for conduction implants, such as a BAHA, a Ponto, a Vibrant Soundbridge, or a Bonebridge. In this case report, we present 2 patients with TCS implanted with the Bonebridge system, their audiological results, and quality of life.
Keywords
Introduction
Treacher-Collins syndrome is an autosomal dominant disorder that affects the first and second branchial arches.1,2 The estimated incidence is 1/50 000 live births. 3 Deformation of facial structures produces a characteristic appearance that includes malar and maxillomandibular hypoplasia, downward-slant of palpebral fissure, frequently with colobomas of the lower eyelids and ear anomalies. Malformations of the ear include abnormalities of the external ears, atresia of external auditory canals, and malformation of the middle ear ossicles which result in conductive hearing loss. 4
The Bonebridge ((BB) MED-EL Innsbruck, Austria) is one of the options for hearing rehabilitation of conductive hearing loss, leaving the skin intact. This hearing implant directly transfers sound to the inner ear through the bones of the skull, enabling, natural “appearing hearing.” Bonebridge is available for adults and children from 5 years of age. Even though, a recent study showed the possibility of early implantation as young as two years with beneficial results in a bilateral atresia child.
5
Suitable anatomical predisposition is a prerequisite for successful operation. The patients with TCS are often shown to have different temporal bone anatomy on CT scans. The 2nd generation Bonebridge, the Bone Conduction Implant 602 (BCI 602) (Figure 1A and B) was engineered from the ground up to deliver optimal surgical handling and reliable implant fixation. With the new size and shape, the BCI 602 can be used in patients previously excluded due to insufficient anatomical conditions, especially in patients with congenital defects of the outer and middle ear, such as those associated with Treacher-Collins syndrome.
6
The BCI602 implant system (left) picture of implant and the externally worn Audio processor (A) and (right) picture of implant from top and side view to show the positioning/tilting options in degrees, respectively (B). (Implant pictures courtesy of MED-EL).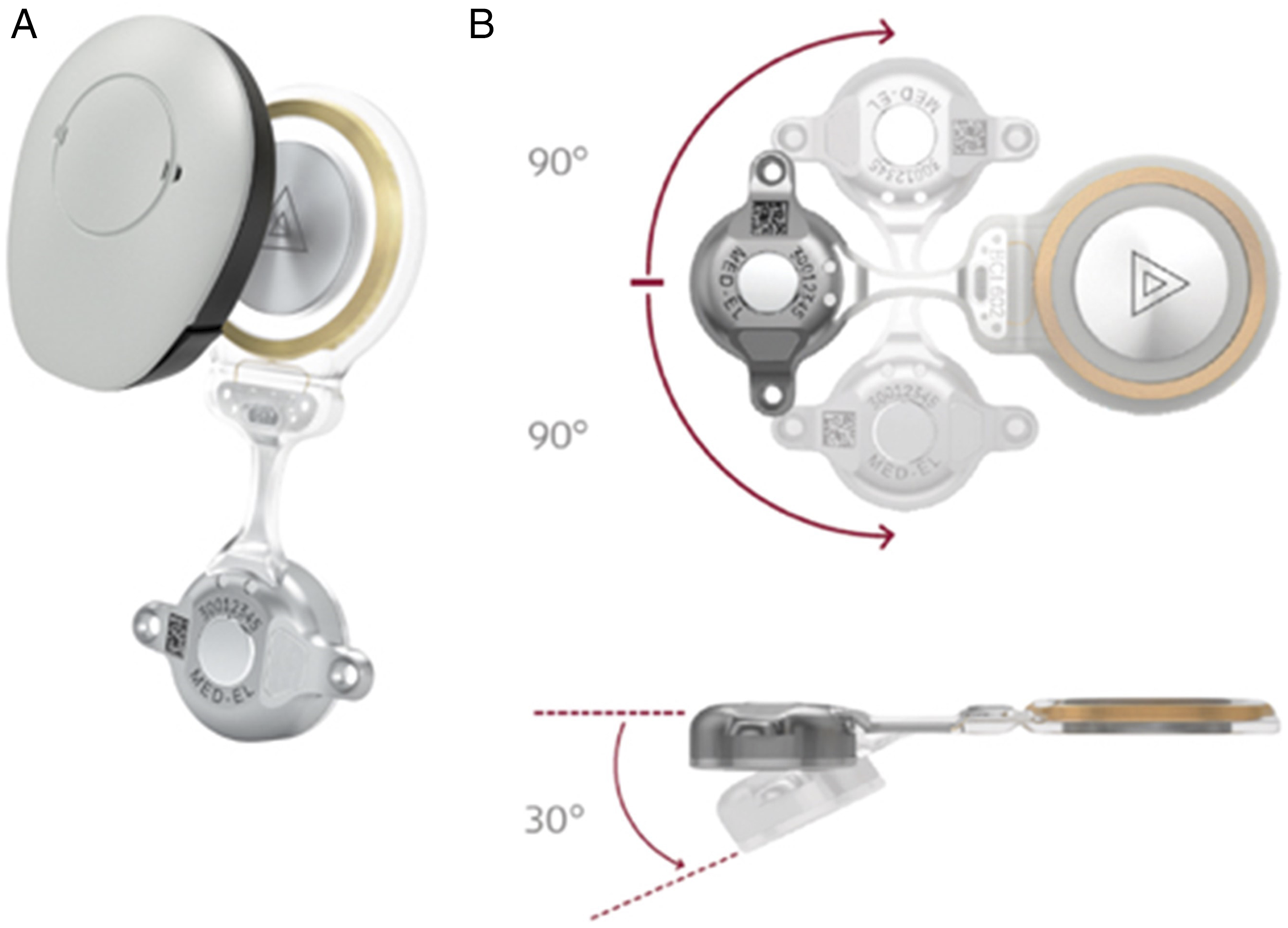
Methods
Patient demographics, etiology, otologic history, and surgical approaches.
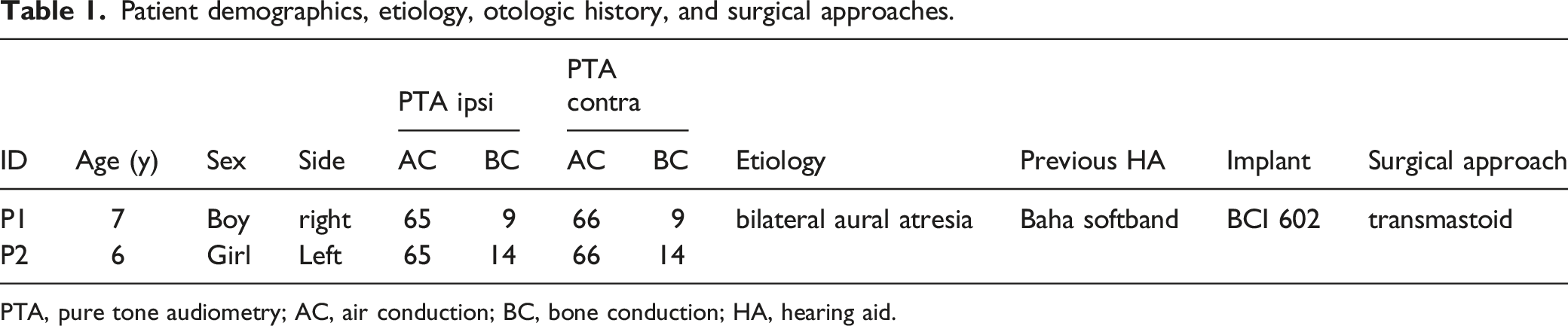
PTA, pure tone audiometry; AC, air conduction; BC, bone conduction; HA, hearing aid.
Statistics
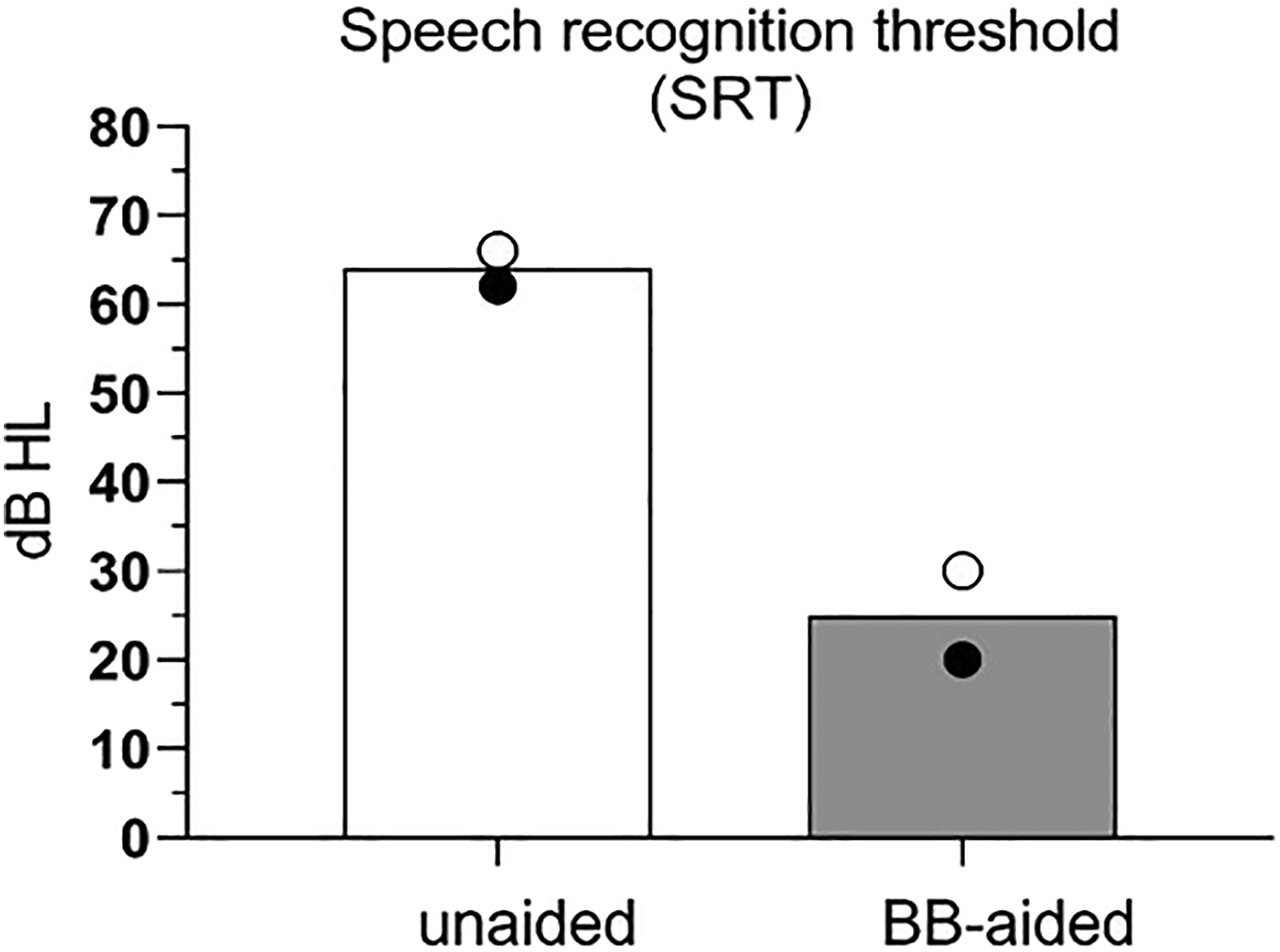
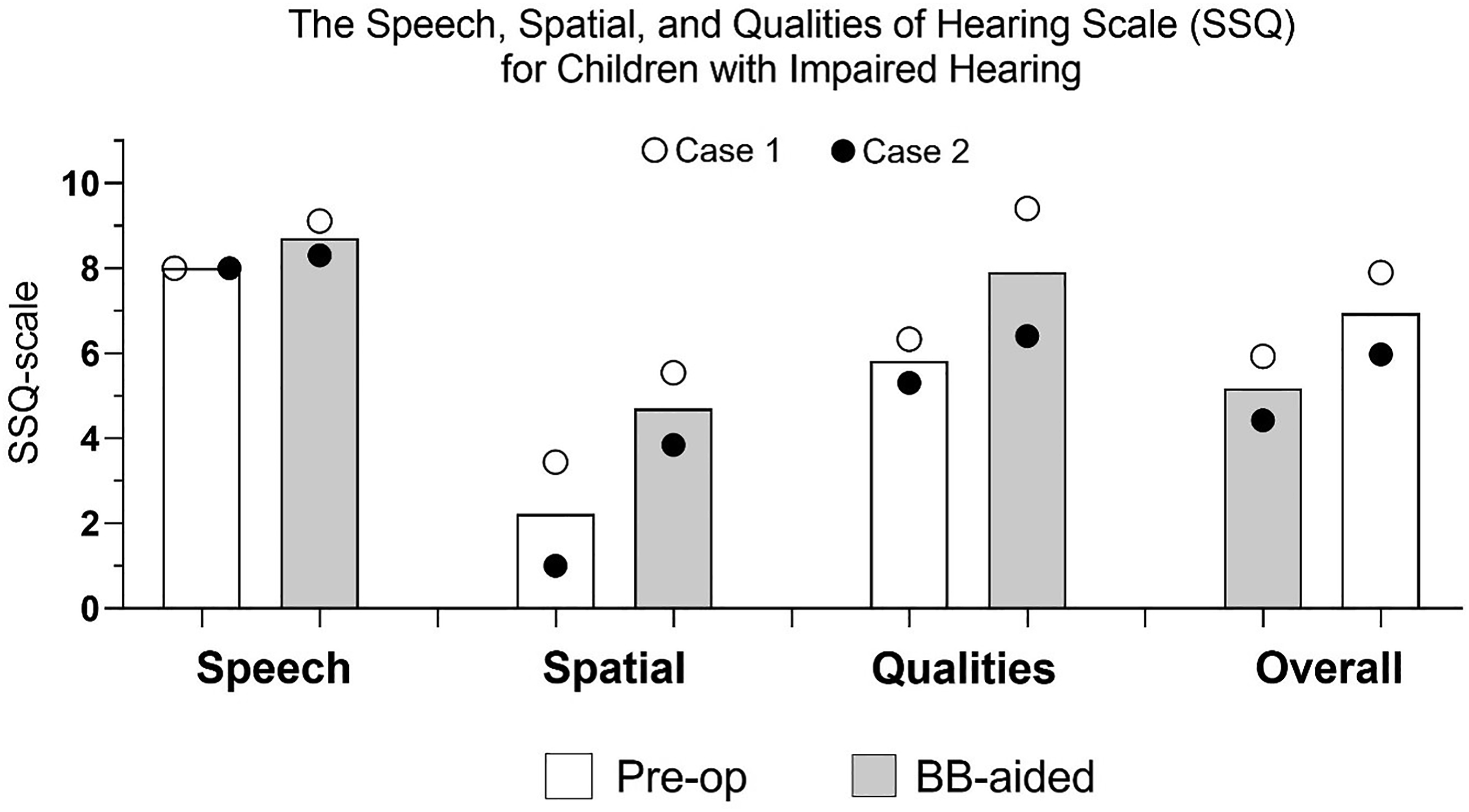
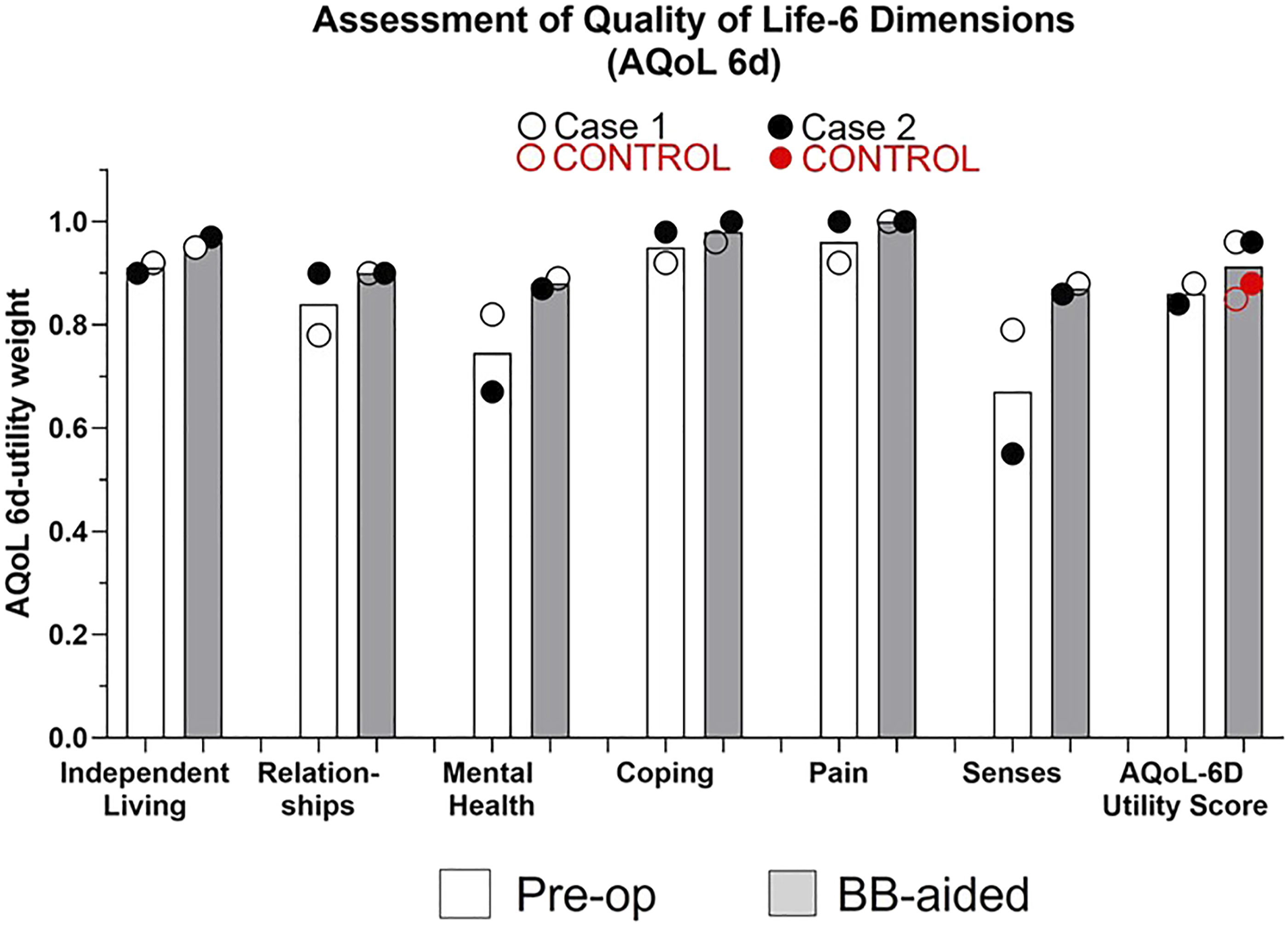
No statistical analysis was performed due to the low sample number of n = 2. Scatter dot plots for better visualization of the outcomes were generated. Audiological results are presented in Figures 2 and 3 and AQoL Questionnaire outcomes are shown in Figure 4 and 5. Soundfield audiometry (left) graph shows case 1 and (right) graph case 2 over the frequencies of 500, 1000, 2000, and 4000 Hz. Symbols and lines indicate the unaided situation, previous Hearing Aid (HA), and post-operative bonebridge-aided situation, respectively. Speech recognition threshold in dB HL for the unaided, pre-operative condition, and the improvement in the bondebridge-aided condition. Circles show the two individual cases separated. Speech, spatial qualities of hearing (SSQ). Subscores of speech, spatial hearing and perceptive qualities as well as the total score comparing unaided (white bar) to Bonebridge-aided (grey bar) results. There was improvement in each subscore. Circles show the two individual cases separated. Assessment of quality of life-6 dimensions (AQoL 6d). Subscores of independent living, relationships, mental health, coping, pain, senses as well as the total utility score comparing pre-operative (pre-op) (white bar) to Bonebridge-aided (grey bar) results. There was improvement in each subscore and outcomes of the two cases exhibited better results than their normal hearing, age, and sex matched controls (red circles). Circles show the two individual cases.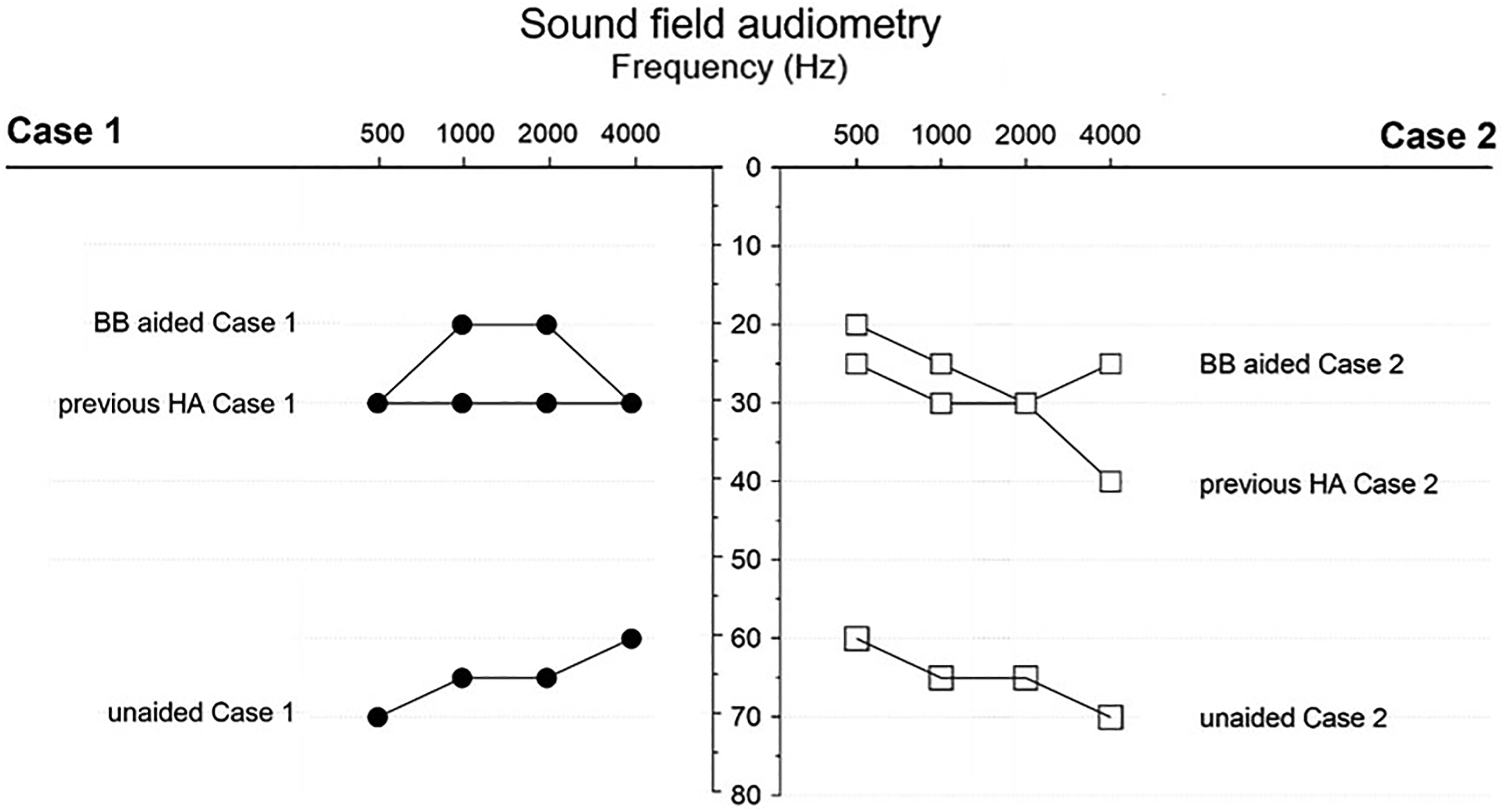
Age appropriate audiological examinations were performed, including two questionnaires before and after surgery. All audiological examinations were performed with and without the Bonebridge as well as with hearing aid used before implantation (Baha Softband). Soundfield audiometry was performed using a narrow band masking noise. All examinations were performed using Interacoustics AC 40 audiometer (Denmark, 2019).
The audiological results.
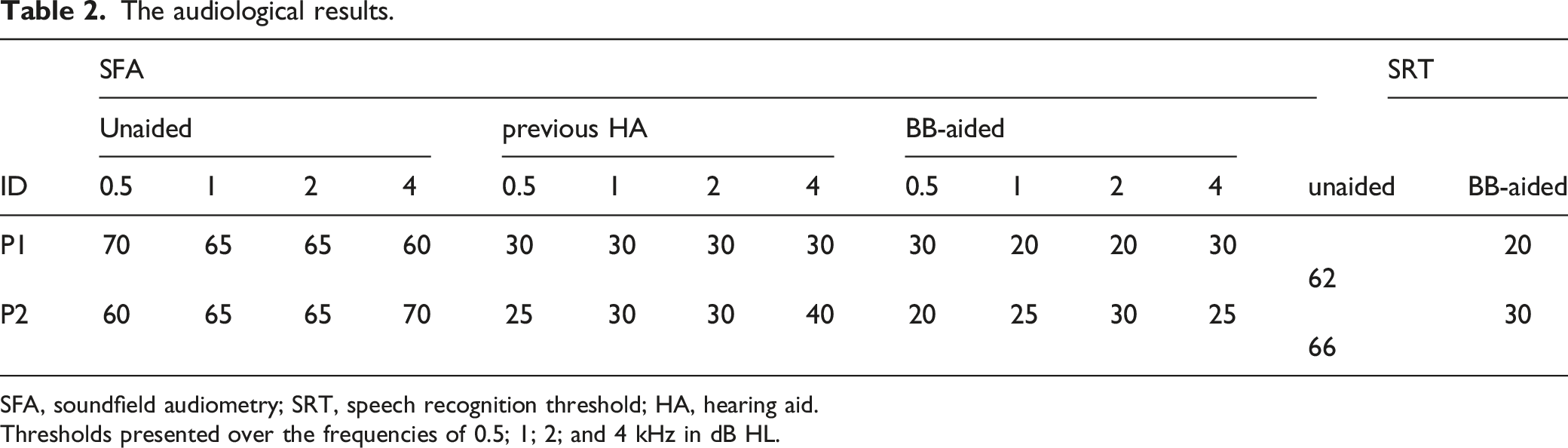
SFA, soundfield audiometry; SRT, speech recognition threshold; HA, hearing aid.
Thresholds presented over the frequencies of 0.5; 1; 2; and 4 kHz in dB HL.
The Speech, Spatial, and Qualities of Hearing Scale (SSQ) results.

Quality of Life-6 Dimensions (AQoL-6D) results.
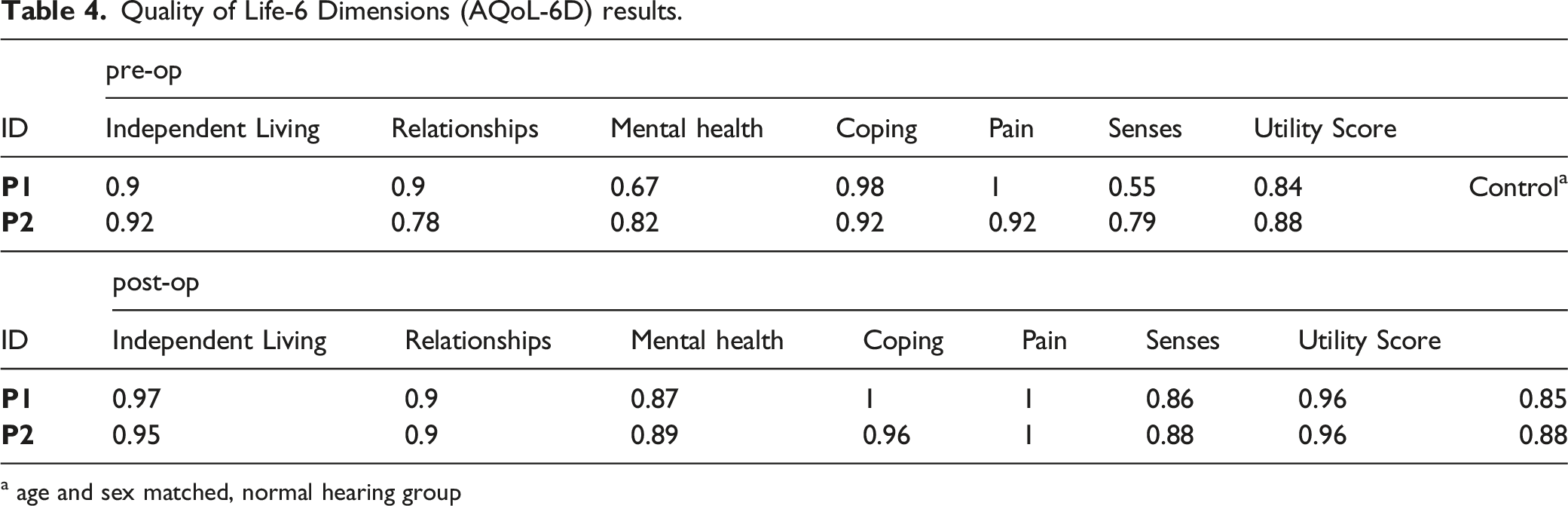
a age and sex matched, normal hearing group
Results
This case report presents two children with TCS implanted with the Bonebridge, a 7-year-old boy and a 6-year-old girl. Both children with auricular microtia and atresia of the ear canal suffered from bilateral conductive hearing loss. As a previous hearing aid, both trialed Baha Softband (Cochlear) with a positive audiological benefit in the test set-up (Figure 2) but some restrictions and draw-backs in wearing comfort in daily life.
Both surgeries went uneventful. The boy was implanted on the right side in 2021 and the girl was implanted on the left side in 2022. Both children were implanted with Bonebridge model BCI 602. The transmastoideal approach was carried out. 9 A modified retroauricular incision was performed, uncovering of the planum mastoideum, shaping of the socket, and placement of the BC-FMT with fixation and suture of the periosteum, subdermis, and skin. The two standard screws were used for fixation of the implant. In the female patient, the dura mater was exposed and compressed about 2 mm with the BC-FMT. The operations were completed without complications, and none occurred during the post-operative period.
Soundfield audiometry revealed in both cases significant conductive hearing loss, which improved when wearing the hearing aid and even further improved after Bonebridge implantations, individual details summarized in Table 2 and can be seen in Figure 2 and 3. The resulting mean PTA4 in the unaided condition was 65 ± 3.54 dB HL and improved with the HA to 30.5 ± 2.94 dB HL and improved further to 25 ± 4.27 dB HL after Bonebridge implantation (Table 2 and Figure 2). The speech recognition thresholds improved from the mean unaided condition of 64 ± 2 to 25 ± 5 in the Bonebridge-aided condition (Table 2 and Figure 3). The analysis of the SSQ questionnaire revealed for the four dimensions of Speech, Spatial and Qualities of Hearing as well as for the overall score a mean improvement from 8.15 ± 0.15 to 8.56 ± 0.56; from 2.42 ± 1.42 to 4.49 ± 1.05; from 5.85 ± 0.55 to 7.87 ± 1.53; and from 5.20 ± 0.77 to 6.91 ± 0.99, respectively. Individual outcomes can be seen in Table 3 and Figure 4. The analysis of the AQoL 6d questionnaire revealed for the 6 dimensions of Independent Living, Relationships, Mental Health, Coping, Pain, Senses as well as the total Utility Score a mean improvement from 0.91 ± 0.01 to 0.96 ± 0.01; from 0.84 ± 0.09 to 0.90 ± 0.00; from 0.75 ± 0.11 to 0.88 ± 0.01; from 0.95 ± 0.04 to 0.98 ± 0.03; from 0.96 ± 0.06 to 1.00 ± 0.00; from 0.67 ± 0.17 to 0.87 ± 0.01; and from 0.96 ± 0.01 to 0.96 ± 0.00, respectively. The utility score for the Bonebridge-aided condition (0.96 ± 0.00) was better, when compared to their age and sex matched normal hearing control with 0.87 ± 0.02. Individual outcomes can be seen in Table 4 and Figure 5.
Discussion
The Bonebridge implant is an active transcutaneous bone conduction system based on the concept of fully integrating the vibrating element into the bone under the skin. The implant composed of an external audio processor and a bone conduction floating mass transducer (BC-FMT) placed into the temporal bone with closed skin. It constitutes a modern and very effective treatment, eliminating certain deficiencies of previous BAHD (Bone Anchored Hearing Devices) passive systems.10,11 Maresella et al. reported an overall percentage of patients experiencing at least one post-operative complication of 34% in the course of the 24 months follow-up in their BAHD-implanted cohort. 12 Those complications included the typically BAHD associated problems including skin hyperemia/granulation around the implant. The advantages of Bonebridge system are especially beneficial to patients for whom it is necessary to have a transcutaneous system with no pressure on the skin, in cases such as the here presented, were the bones of the skull and skin covering are not sufficiently strong and cranial malformations and unfavorable temporal bone anatomy makes placement difficult. The 2nd generation BCI 602 offers the same level of beneficial hearing performance and surgical flexibility due to the reduced size of the implant accompanied with low complication rates. With a reduced drilling depth and small implant footprint, the BCI 602 can be flexibly placed in many positions on the temporal bone. It can bend up to 90 degrees in either lateral direction between receiver coil and BC-FMT. The transition can also bend medially up to 30 degrees in either lateral direction (Figure 1B). This gives an incredible flexibility in placing the implant, enabling optimal outcomes across a wide range of anatomies. This also reduces the risk of dura or other structure exposure and it helps broaden the range of suitable anatomies, making it especially suitable for younger children. 6
Children with Treacher-Collins syndrome suffer from the premature joining of certain bones of the skull during embryonic development, which also affects the hearing ability. The hearing impairment is one of the most limiting factors for social development in children. TCS management is a multidisciplinary affair, as interventions range from reconstructive to psychosocial interventions. People with TCS do not usually have associated intellectual disabilities and intelligence remains preserved, but developmental delays depend on the degree of hearing impairment and the ability to communicate and learn normally. 13 The two TCS cases implanted with the Bonebridge BCI 602 show, that it is a suitable and effective treatment for auditory rehabilitation, providing optimal surgical manipulation and reliable implant fixation, especially in difficult mastoid anatomy cases.
In general, very few Treacher-Collins cases have been reported in the literature and these have consisted primarily in BAHD implantations associated with complications due to skin reactions.10,12,14 Whereas Bonebridge implanted individuals suffering from malformations reported low complications. 15 Post-operative pain related to Bonebridge Implantation has also been evaluated as relatively low. 16 Treacher-Collins syndrome has a wide variation of clinical presentation which affect patient-rated quality of life. Studies on the quality of life in children with and without craniofacial anomalies have considered children from five years of age eligible to respond to instruments that measured the quality of life. It has even been described that children from this age on can be self-critical and therefore, the use of a validated instruments are reliable indicators for AQoL in this pediatric cohort.17-20 De Oliveira et al. reported outcomes utilizing the World Health Organization Quality of Life (WHOQOL-100) questionnaire and concluded that best-performing Treacher-Collins syndrome patients under multidisciplinary treatment presented intermediate and satisfactory quality of life, consistent with quality of life scores of unaffected controls. 20 Among our patients, satisfaction with the audiological benefit, comfort and aesthetics of the BONDEBRIDGE is very high. 21 Those beneficial results were also seen in the two here presented Treacher-Collins Syndrome subjects, applying for audiological benefit, patient satisfaction, hearing quality, and quality of life which corresponds with what is reported in the literature.15,22-24
Conclusion
Treacher-Collins syndrome is an autosomal dominant disorder that manifests as abnormal development of facial bones and tissues. These malformations have a negative impact on the individual's visual and auditory perception. People with TCS suffer from mild to severe conductive hearing loss. The hearing impairment is compensated by hearing aids or implants for bone conduction. The Bonebridge BCI 602 is especially for these unfavorable anatomical conditions of temporal bone in TCS patients a suitable and effective treatment option. Our two implanted children report very good results in communication and using the audio processor on a day-to-day basis, while parents especially appreciate the improvement in social interactions and speech development.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ministry of Health, Czech Republic, Conceptual Development of Research Organization (FNBr, 65269705) and Masaryk University in Brno (MUNI/A/1365/2022).
Ethical Statement
The study protocol was approved by the ethics committee of University Hospital (No. 03-041120) and informed consent of the parents/legal guardian was given prior surgical intervention.
Data Availability Statements
All data are available from corresponding author.