
Abstract
Desmoid-type fibromatosis (DF) is a rare soft tissue lesion with an annual incidence of 2 to 4 per million population and peak incidence occurring at approximately 4.5 years of age. While benign, the tumor has a locally aggressive infiltrative growth pattern and a high rate of recurrence. Given the functional and aesthetic implications of excision and reconstruction in the facial skeleton, novel medical treatment options are highly desirable. We describe the case of a 3-year-old boy who presented with an enlarging, asymptomatic mass involving the left mandible. Biopsy revealed an immunohistochemical profile consistent with DF. Despite the high likelihood of recurrence, conservative, mandible-sparing en bloc resection and limited mandibulectomy were performed. Pathological and immunohistochemical analysis of the resection specimen revealed DF with grossly positive margins and elevated expression of angiotensin II type 1 receptor. Postoperative medical treatment with the angiotensin receptor blocker losartan was initiated. The patient remains medically stable and disease progression-free on repeat imaging at 20 months post-resection. We describe for the first time the successful use of the angiotensin blocker losartan following conservative surgery for management of DF.
Introduction
Desmoid-type fibromatosis (DF) is a rare soft tissue lesion with an annual incidence of 2 to 4 per million population and a peak incidence in pediatric patients at approximately 4.5 years of age. 1 Histologically, DF is characterized by interlacing fascicles of bland spindle cells within a collagenous stroma lacking evidence of atypia. Immunohistochemical analysis typically demonstrates strong positivity for vimentin and variable staining for smooth muscle actin and nuclear β-catenin. Despite being benign, the tumor has a locally aggressive infiltrative growth pattern and a high rate of recurrence. 2 Treatment strategies include surgical excision, radiotherapy, chemotherapy, and, more recently, noncytotoxic systemic therapies including tyrosine kinase inhibition. 3 Given the functional and aesthetic implications of wide local excision and reconstruction in cases involving the facial skeleton and given the potential long-term side effects associated with radiation and chemotherapy, there remains a need for less morbid treatment strategies.
Case Report
A 3-year old boy was referred to a tertiary paediatric otolaryngology service with a 2-week history of an enlarging, asymptomatic, left-sided neck mass below the angle of the mandible. A working diagnosis of atypical mycobacterial cervical adenitis was made, and clarithromycin and rifampin were prescribed. Due to diagnostic uncertainty, a 2-week reassessment was planned, but the patient failed to return. Three months later, the patient presented with further enlargement of the mass without the violaceous skin discoloration or abscess characteristic of atypical mycobacterial infection.
Computed tomography (CT) revealed a left-sided, 5.2 cm, solitary, nonenhancing, hypodense submandibular neck mass in continuity with the partially eroded inner cortex of the left body of the mandible. No associated cervical lymphadenopathy or bony abnormalities were noted (Figure 1A, C-D). Magnetic resonance imaging (MRI) revealed a heterogeneous T2 signal which was contrast-avid (Figure 1B). The mass appeared to be centered on the mandible with periosteal thinning and elevation, and cortical plate expansion and reaction at both the lingual and buccal surfaces. There was evidence of expansion of the mandibular canal. The medullary canal was spared except at the angle of the mandible where signal changes suggested either bone marrow involvement or edema.
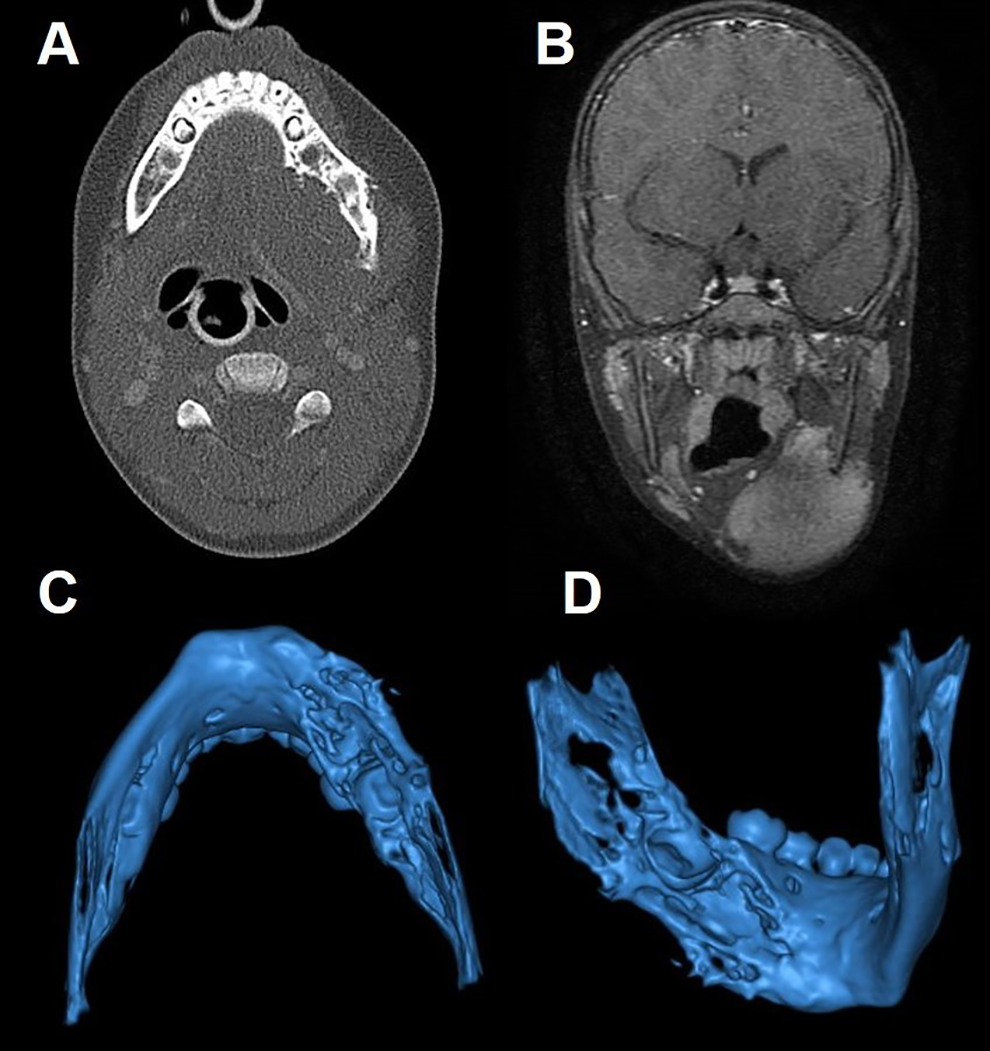
(A) Axial CT and (B) coronal MRI imaging demonstrating mandibular erosion and left neck mass. 3D volume rendered CT reconstruction imaging of (C) inferior view and (D) left inner aspect of mandible demonstrating erosive bone loss. CT indicates computed tomography; MRI, magnetic resonance imaging.
Incisional biopsies revealed fascicles of bland spindle cells within a collagenous matrix. The immunohistochemical profile was consistent with DF based on the presence of β-catenin nuclear positivity and CTNNB1 gene mutation. No evidence of atypia or mitotic activity was observed. Angiotensin II receptor type 1 (AT1 R) status was not assessed prior to resection. The primary consideration in the differential diagnosis, based on the histology and clinical features, was desmoplastic fibroma.
Given the infiltrative nature of DF into surrounding tissues, a recommendation of wide surgical resection was made following discussion at the institutional tumor board. A hemimandibulectomy was considered, but owing to its disfiguring and poor functional outcomes, a conservative resection was favored, despite the high likelihood of recurrence and potential need for further, more aggressive surgery. The conservative intervention included gross en bloc tumor resection with partial mandibular cortex preservation, subsegmental mandibulectomy, and bone curettage. Additionally, an ipsilateral selective neck dissection through levels II to IV was completed with preservation of the surrounding nerves and tooth buds (Figure 2A-D). Pathologic and immunohistochemical analysis of the resection specimen were identical to the biopsy with the additional findings of AT1 R (Figure 3A-B) and nuclear β-catenin (Figure 3C) positivity. All surgical margins were grossly positive.
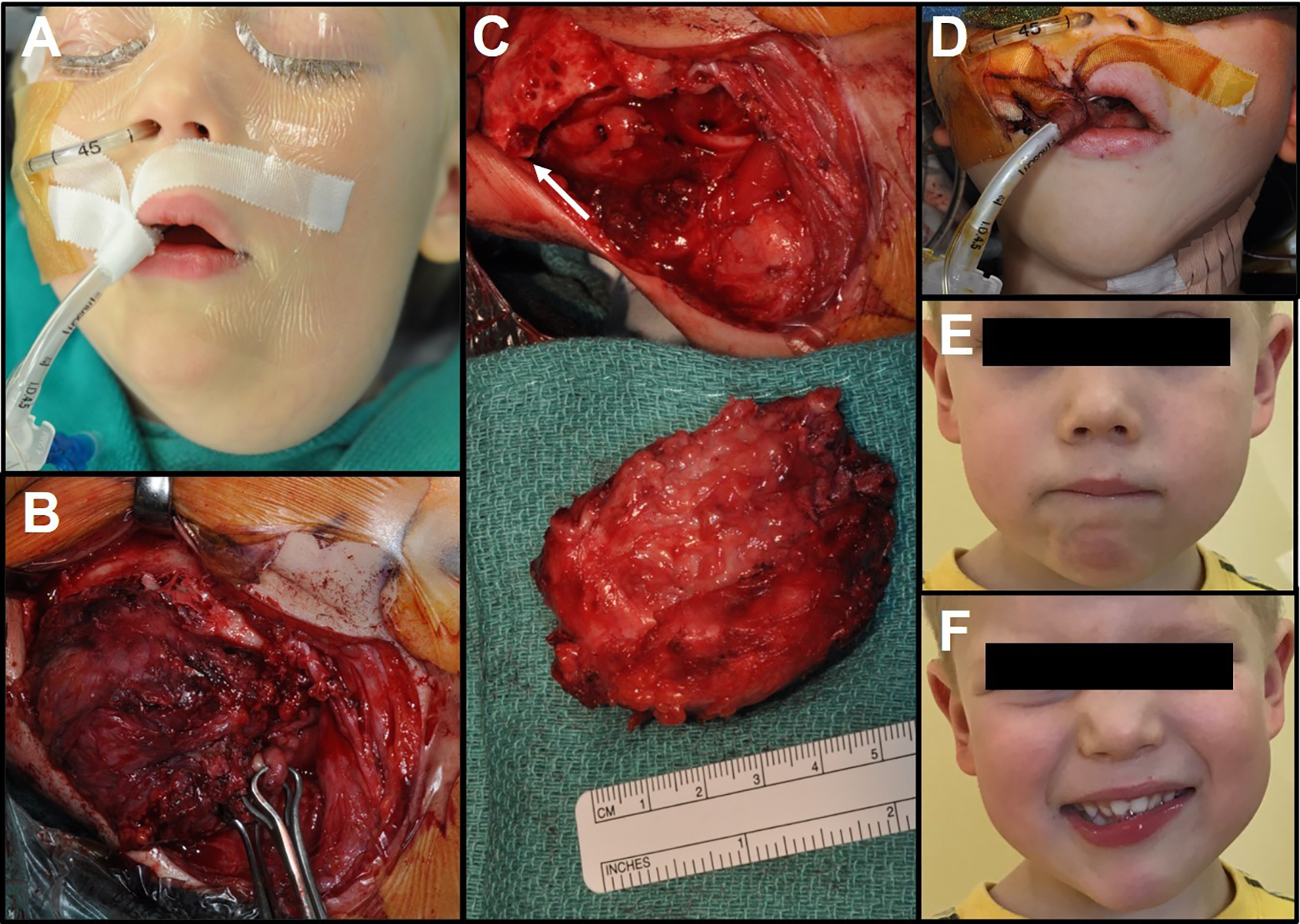
(A) Preoperative view; (B) intraoperative exposure; (C) resected tumor with scalloping of inferior mandibular margin (arrow); (D) immediate postoperative view; (E) resting state and (F) smiling appearance at 16-month postoperative clinic follow-up appointment; normal mandibular contour as well as mild left marginal mandibular nerve palsy are noted.
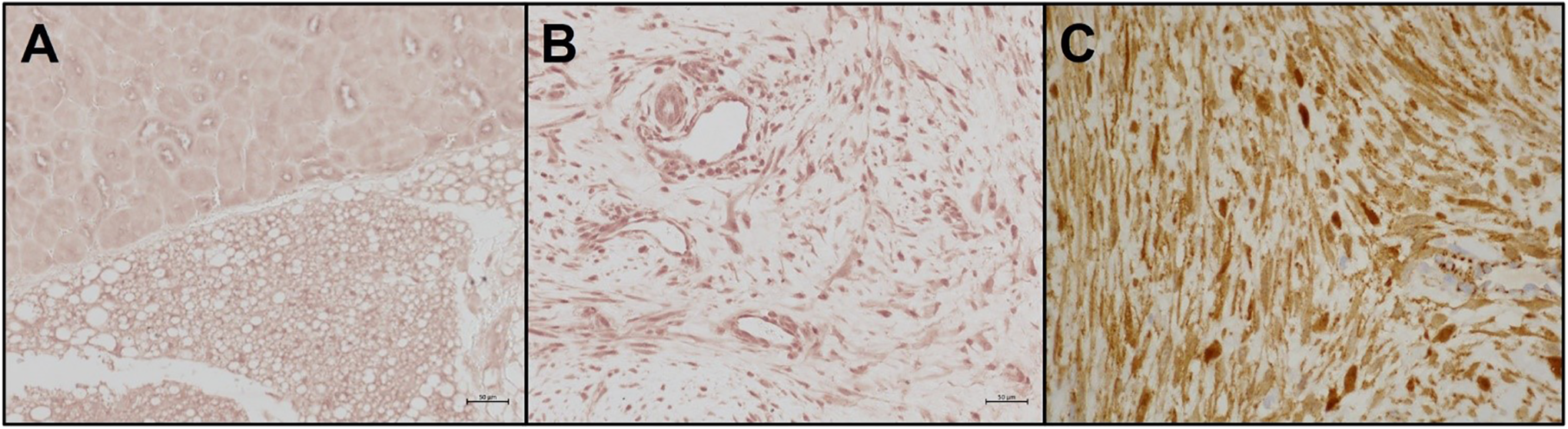
Immunohistochemical staining for angiotensin II type 1 receptor (AT1 R). (A) Kidney (positive control); (B) tumor demonstrating abundant positive staining of fibroblasts; (C) tumor demonstrating positive nuclear staining for β-catenin.
The patient tolerated the procedure well and had an uncomplicated postoperative course aside from mild marginal mandibular nerve weakness which resolved by the most recent follow-up appointment (Figure 2E-F). Considering the high level of AT1 R expression in the surgical specimen, postoperative medical treatment with the selective angiotensin receptor blocker losartan was initiated with ongoing titration to achieve a dose of 1 mg/kg/d. Side effects of angioedema, hyperkalemia, hypotension, and dose intolerance were not apparent at regular 3-month assessments. The patient was medically stable, well, and disease progression-free on repeat MRI at 20 months post-resection.
Discussion
Desmoid-type fibromatosis is a benign, nonmetastasizing, but locally destructive tumor. Management of DF in the facial skeleton can be challenging given that the lesion is difficult to diagnose, involves potentially disfiguring surgery, and has recurrence rates as high as 70% in the context of incomplete excision. 4 There are no pathognomonic clinical or radiological features, and surgical resection margins and reconstruction must weigh aesthetics, function, and craniofacial development in the paediatric patient.
Histologically, DF is not easily distinguished from desmoplastic fibroma, which may be histologically identical. In this case, the presence of CTNNB1 gene mutation favored DF. The expression of AT1 R in these tumors has not previously been described. Considering the high expression of AT1 R, and a reported recurrence rate in grossly positive resection margins in the head and neck of 70%, 4 medical therapy was initiated using losartan.
While other modalities were considered, these were not adopted considering their morbidity. Radiotherapy can be considered in cases where DF is unresectable, but carries well-documented detrimental effects on craniofacial growth in children. Recent consensus guidelines for the management of desmoid tumors highlight systemic treatment options, including low-dose chemotherapeutics, antihormone therapy, tyrosine kinase blockers, and nonsteroidal anti-inflammatory drugs. 5 In general, indications for the use of these medical therapies in pediatric patients remains unclear, owing to the unfavorable side effect profiles of many of these agents. While chemotherapeutics including methotrexate, vinblastine, and anthracycline have demonstrated progression-free survival rates, they are associated with significant toxicity. Despite their more favorable safety profiles, immunomodulatory tyrosine kinase inhibitors such as sorafenib and pazopanib still can require discontinuation or dose reduction due to toxicity. Consensus guidelines do not provide direction on a specific treatment sequence in children owing to a lack of comparative studies. In appropriate cases (depending on progression rate and anatomical location), initial trials with less harsh or toxic therapies are indicated. 5
The antitumor benefits of angiotensin blockade have been reported in other solid cancers in both humans and animal models, with angiotensin II engagement of AT1 R being implicated in cancer-associated fibrosis and desmoplasia. 6 Recent clinical trials have pointed to the potential of losartan as a neoadjuvant pancreatic cancer treatment to reduce desmoplasia and improve chemotherapeutic penetration. 7 In the current case, the high expression of AT1 R on the primary tumor made it an attractive target. Additionally, losartan is known to be well tolerated. We speculate that selective blockade of AT1 R signaling by losartan reduced proliferation of the tumor fibroblasts, leading to the observed progression-free survival at 20 months.
Desmoid-type fibromatosis is an extremely rare and locally aggressive but benign tumor. Wide surgical resection is often warranted but is functionally and aesthetically morbid, particularly in the facial skeleton. Standardized treatment decisions based on surgical margin status are lacking at present, but reports demonstrate a high rate of recurrence in cases with grossly positive margins. This case report describes a novel combined approach of limited mandibulectomy and medical management with an oral angiotensin receptor blocker. Limitations include reliance on a single case; to this end, additional cases are required to assess if this approach can be more widely adopted. Future high-quality studies should focus on an immunohistochemical assessment of additional DF specimens for AT1 R expression. Larger studies may also investigate the degree to which angiotensin blockade may be combined with other medical therapies to potentiate their benefits. While still exploratory, this report points to a novel, less toxic alternative to current medical therapies for desmoid-type fibromatosis.
Footnotes
Authors’ Note
D.E.C. contributed to data collection, literature review, drafted the manuscript, and approved the final manuscript. A.A.A. contributed to literature review and to manuscript preparation and approved the final manuscript. J.T. completed treatment, offered expert opinion, contributed to manuscript preparation, and approved the final manuscript. M.W. completed treatment, offered expert opinion, contributed to manuscript preparation, and approved the final manuscript. P.D.A completed management and treatment, offered expert opinion, contributed to manuscript preparation, and approved the final manuscript. C.M. completed management, offered expert opinion, contributed to manuscript preparation and data collection, and approved the final manuscript. L.B.J. completed management and treatment, offered expert opinion, contributed to manuscript preparation and data collection, and approved the final manuscript. M.B. supervised the report, completed case management and treatment, offered expert opinion, contributed to manuscript preparation and literature review, and approved the final manuscript. The data sets used and/or analyzed during the current study are available from the corresponding author on request. Consent for publication was obtained by this study by the patient’s family in accordance with the institutional research ethics board.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.