
Abstract
Patients with severe coronavirus disease 2019 (COVID-19) may have endothelial inflammation, pseudoaneurysm, and an increasing risk of bleeding, especially during surgical procedures. In this article, we reported 2 cases of COVID-19 patients with neck vascular lesions. The first patient had pseudoaneurysm of the cricothyroid artery, which was treated by percutaneous glue injection through ultrasonography guidance. The second patient presented lateral neck hematoma in front of the left superior thyroid artery, which was managed by coil endovascular embolization. In the context of pandemic, the management of vascular lesions may be performed through interventional radiological procedures that may reduce the risk of virus aerosolization and health care provider contamination.
Introduction
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) may be associated with endothelial inflammation and an increasing risk of hemorrhage. 1 Because the infection is associated with a high risk of aerosolization and related health care provider contamination, the treatment of vascular lesions has to be as conservative as possible. 2 From March 1, 2020, to May 28, 2020, 74 patients with severe coronavirus disease 2019 (COVID-19) were hospitalized in our intensive care unit (ICU) and 35 (47%) patients benefited from surgical tracheotomy. The tracheotomy made sense in a context of pandemic and ICU saturation because tracheotomy allowed the reduction in the duration of mechanical ventilation, leading to a faster discharge of patients from the ICU. 2 Among them, 3 (8.5%) individuals developed severe bleeding from the superior thyroid artery. Two patients benefited from interventional radiological procedures and a patient had surgical exploration and ligation of the right superior thyroid artery. In this article, we report the history and the conservative management of the 2 COVID-19 patients who had vascular lesion.
Case 1
Patient History
A 50-year-old male were hospitalized in ICU for a critical COVID-19 infection. The patient required curative anticoagulant therapy for a right internal jugular thrombosis and were tracheotomized 7 days (d7) after its admission to be weaned from the mechanical ventilation. Patient was discharged from the ICU at 2 weeks (d14) and he was transferred into the internal medicine department. Seven days after the ICU discharge (d21), patient reported neck discomfort and bleeding around the tracheotomy tube. The neck CT scan revealed a pseudoaneurysm of the cricothyroid artery, which was close to the tracheotomy tube (Figure 1A and B). The pseudoaneurysm was attributed to the vessel abrasion by the tracheotomy tube. According to the comorbidities of patient and the risk of aerosolization, an experimental percutaneous endovascular intervention was performed.
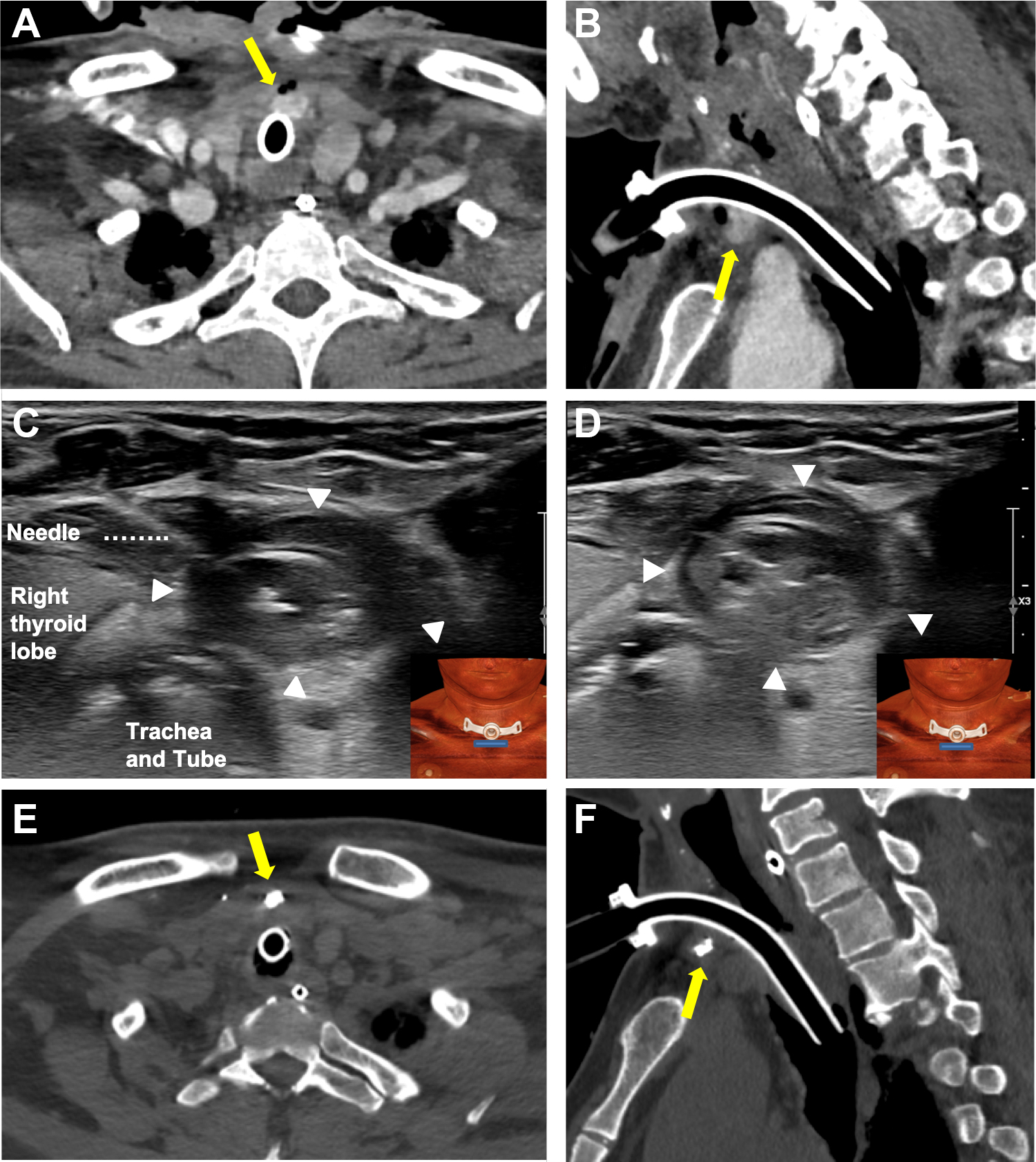
Findings of patient with pseudoaneurysm. Pre-embolization angio-CT scan in axial (A) and sagittal (B) views reported pseudoaneurysm close to the tracheotomy tube. The percutaneous embolization procedure was performed through a fine needle that was introduced until the center of the pseudoaneurysm and the radiologist injected emulsion material (Glue + LUF) (C). The pseudoaneurysm was occluded with the emulsion material (D). Immediate postembolization neck CT scan in axial (E) and sagittal (F) views showed a spot of the emulsion material (Glue + LUF) within the pseudoaneurysm (arrow).
Pseudoaneurysm Embolization
The pseudoaneurysm was located with neck Doppler ultrasonography using a linear probe.
After local anaesthesia (Lidocaine hydrochloride 10 mg/mL, Aguettant), a fine needle (Spinocan, 0.90 × 88 mm, 20G, B. Braun Medical) was inserted until the middle of the pseudoaneurysm and radiologist injected an emulsion of Lipiodol Ultra Fluid (LUF, 1 mL; Guerbet) and Glubran2 (GEM) in a volume ratio of 1 to 1 pushed by 1 mL of Glucose serum (Figure 1C and D).
The post-embolization tomodensitometry confirmed the emulsion deposit within the pseudoaneurysm (Figure 1E and F). There was no further bleeding and patient was discharged a few days later.
Case 2
Patient History
A 76-year-old COVID-19 male with history of coronary disease, diabetes, hypertension, and heart arrhythmia was admitted in the ICU for respiratory distress requiring mechanical ventilation. The patient underwent surgical tracheotomy 7 days after its ICU admission. Surgical tracheotomy was performed without difficulty. Forty-eight hours after the tracheotomy (d9), patient underwent neck CT scan for bleeding around the tracheotomy tube. The tomodensitometry confirmed lateral neck hematoma in front of the left superior thyroid artery (Figure 2A and B). According to the bleeding risk and the clinical state of the patient, physicians proposed a conservative management of the hemorrhage.
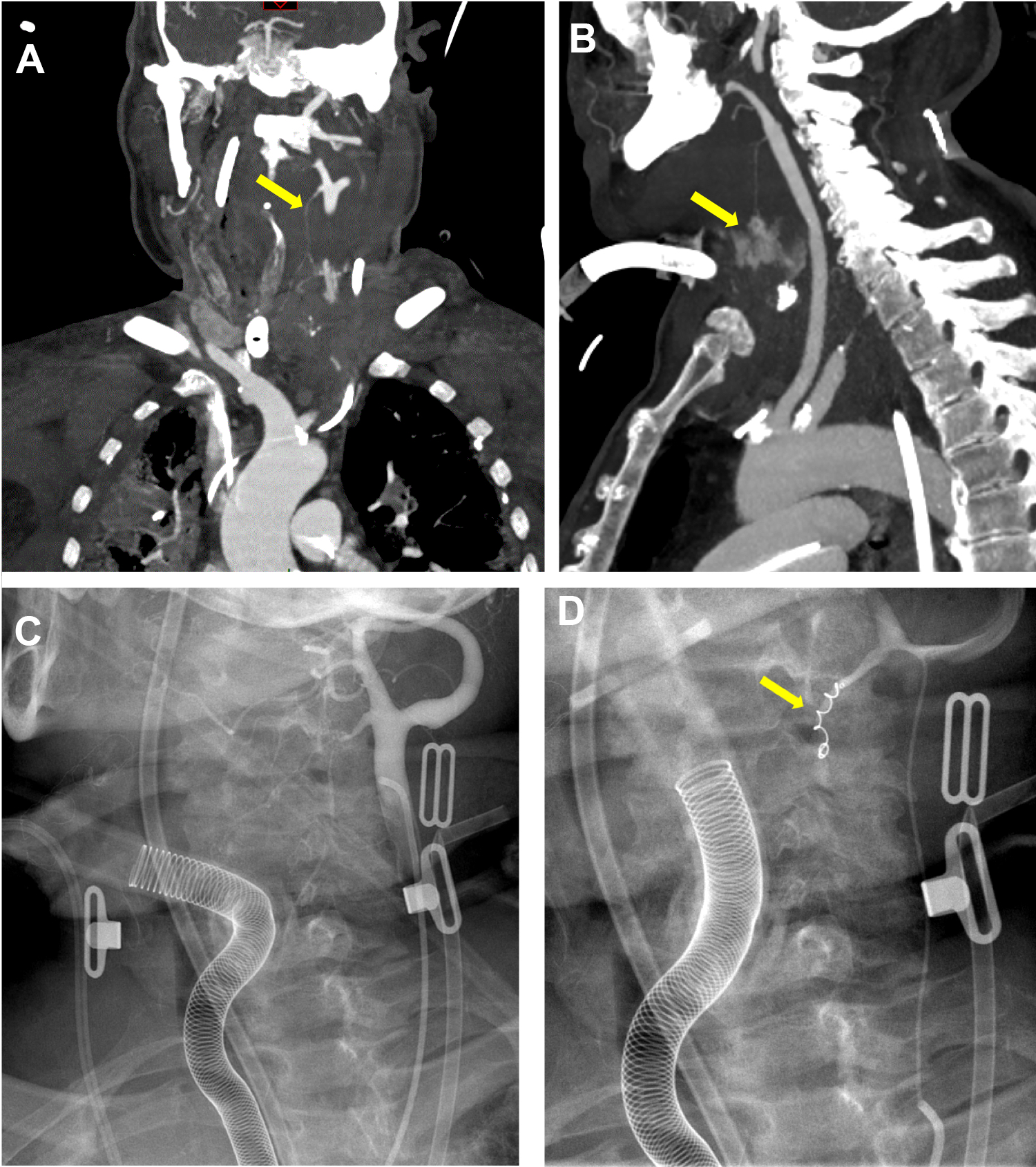
Findings of patient with neck hemorrhage. Pre-embolization angio-CT in frontal (A) and sagittal (B) views revealed a massive deep neck leakage of contrast material from the left superior thyroid artery (arrows). The imaging of embolization procedure showed left common carotid angiogram (C) and microcatheterization and coiling of the left superior thyroid artery (D, arrow).
Hemorrhage Management
Patient was transferred in the radiology department. The procedure was performed through a fluoroscopy system (Multidiagnost Eleva, Philips Medical System).
Radiologist identified the left external carotid artery through right groin site puncture.
The culprit left superior thyroid artery was cannulated with a 0.018-inch microcatheter (Maestro 2.4 French; Merit Medical). Angiogram demonstrated an irregular vessel.
The vessel was occluded with a coil (MicroNester 0.2 × 3 cm; Cook Medical; Figure 2C and D).
The bleeding subsequently resolved. There was no recurrence of the hemorrhage. Five days after the procedure (d14), the patient had multivisceral organ failure and septic collapse and died.
Discussion
The surgical management of vascular complications of COVID-19 patients is challenging regarding the critical clinical condition of many COVID-19 patients and the high risk of aerosolization and health care provider contamination. In this technical paper, we reported 2 original findings.
First, the occurrence of head and neck vascular complications in ICU patients, which were poorly referenced in the literature. Severe acute respiratory syndrome coronavirus 2 is known to be associated with endothelial inflammation and vascular wall impairment. 1 In the first case, it seems conceivable that the tracheotomy tube had weaken the cricoarytenoid artery through a friction mechanism. This kind of complication was poorly reported in the literature, 3 which strengthens the need to monitor patients with severe COVID-19 and tracheotomy. In the second case, the vascular lesion was relatively far from the surgical site of tracheotomy that was performed in front of the third tracheal ring. Thus, we believe that the hemorrhage of the second patient was not associated with the tracheotomy procedure. The hemorrhage was probably due to the SARS-CoV-2 endothelial impairment, which was favored by the patient comorbidities and the use of preventive anticoagulant therapy.
Second, the rational to perform conservative treatment in COVID-19 patients was based on the critical clinical condition of patients, the high risk of aerosolization 2,4 and the related risk of health care provider contamination, especially otolaryngologists. 5 In this article, we reported 2 original interventional radiological approaches for the treatment of vascular lesions of the head and neck region. To the best of our knowledge, there was no similar paper in the literature, which reported percutaneous and endovascular approaches in the context of the COVID-19 pandemic. On the one hand, these approaches avoid the risk of aerosolization during the surgery revision where otolaryngologists mobilize the tracheotomy tube. On the other hand, general anesthesia is not required that may be valuable for patients who are more vulnerable. Notwithstanding the COVID-19 situation, interventional radiological management of bleeding from superior and inferior thyroid arteries was rarely reported. 3 This approach is safe, fast, and easy to perform. 6
Conclusion
COVID-19 patients may have a higher risk of vascular impairments, leading to pseudoaneurysm or head and neck hemorrhage. According to the risk of aerosolization during head and neck surgical approaches, physicians may propose conservative endovascular treatment that are rapidly performed by interventional radiologists and associated with adequate outcomes.
Footnotes
Authors’ Note
The authors thank B. Johnson for the proofreading of the paper. This article does not contain any studies with human participants or animals performed by any of the authors. IRB approved the study (CHUSP, 2020-01). Consent was obtained.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.