
Abstract
Introduction
Transoral robotic surgery (TORS) represents a valuable therapeutic modality, albeit not without inherent risks. Among these risks, the most common complication of TORS is postoperative hemorrhage, 1 with an incidence ranging from 1.5% to 13.1%2-11 as documented in the existing literature. In particular, up to 67% of these incidents could necessitate operative interventions, such as localized cauterization. 2 Alarmingly, a subset comprising 33% might require a life-saving intervention. 2 Profuse hemorrhagic events pose a paramount risk, which could culminate in airway compromise, asphyxiation, hemodynamic instability, and eventual mortality, with a reported fatality rate of 0.3%. 12 The seminal classification system for postoperative hemorrhage, as described by Pollei et al, 2 defines major and severe hemorrhage as life-threatening events, managed with a transcervical or transoral ligation, emergent tracheotomy, or blood transfusions. The incidence of major and severe hemorrhage has been reported as high as 2.9%, 12 and certain patient subgroups, such as those receiving antithrombotic medications or those with large tumors, appear to be at an increased risk.2,6,12,13
A variety of biomaterials, including those based on fibrin or thrombin, have been designed to bolster the coagulation cascade following their topical application in the surgical field. These materials have been extensively used in a range of head and neck surgery procedures, where the preservation of effective hemostasis is of the utmost importance. In particular, fibrin sealants appear to be associated to a decrease in postsurgical drainage output following neck dissections and thyroidectomies.14,15 Although there are fewer studies evaluating gelatin-thrombin matrix agents, they also appear to be effective at reducing postsurgical drainage after thyroidectomies. 16
Within the context of TORS, managing the risk of hemorrhage remains a critical concern. Although the use of hemostatic agents during TORS has been described,17-19 their application remains largely empirical, given the scarcity of scientific literature that examines hemostatic options in this setting, beyond external carotid branch ligation. 12 Furthermore, there is a significant gap in the existing body of research concerning the use of topical agents during TORS to decrease the risk of postoperative hemorrhage. This study aims to provide an initial step in filling this gap by examining the frequency and severity of all postoperative hemorrhagic events in a group of patients who underwent TORS while using various topical hemostatic agents. The objective was to determine whether different varieties of gelatin-thrombin matrix agents could decrease the risk of postoperative hemorrhage. These agents have become widely available and have a relatively low cost; thus, it is important to evaluate their dependability. To our knowledge, no other study has thus far addressed the potential of topical hemostatic agents in reducing the risk of postoperative hemorrhage after TORS.
Materials and Methods
This retrospective chart study enrolled a cohort that included all adult patients who underwent TORS from January 1, 2015, to April 1, 2020, in a single institution. All operative procedures were performed in the Department of Otolaryngology—Head and Neck Surgery, Southern Illinois University, by a single surgeon. Subjects were consecutively included from a “Transoral Robotic Surgery” REDCap database hosted at the Southern Illinois University, that had previously been approved for institutional use. Research Electronic Data Capture (REDCap) is an online platform that facilitates data collection for research projects. Patients were excluded if they did not meet the inclusion criteria. This study was approved by the Springfield Committee for Research Involving Human Subjects, and informed consent was waived due to the retrospective nature of the study.
The following variables were collected through the review of electronic medical records: demographic characteristics (age, sex), indications for the procedure, use of antiplatelet medications or anticoagulation agents during the perioperative period, previous medical treatment (chemotherapy, radiation therapy, or both), presence of flap repair, selected hemostatic agents, additional hemostatic techniques, and presence of postoperative hemorrhage. In 2017, bovine gelatin matrix with thrombin (BgMT; FloSeal® Hemostatic Matrix; Baxter Healthcare Corp) was substituted by porcine gelatin matrix with thrombin (PgMT; Surgiflo®; Ethicon, Inc.) for all procedures in the institution, thus allowing for a natural comparison in time. The classification of postoperative hemorrhage in transoral surgery of the oropharynx, as described by Pollei et al, 2 was used to classify postoperative hemorrhage events other than those considered normal postoperative status. The analysis was performed based on the total number of cases, to account for patients who had multiple TORS procedures. The level of significance of postoperative hemorrhage and other variables was calculated using the chi-square test and Fisher’s exact test, as appropriate.
Results
The study cohort included 78 patients (60 males:18 females) who underwent TORS between January 1, 2015, and April 1, 2020. This population included 80 TORS procedures (62 males:18 females), all performed by the senior author. The mean age of the patients at the time of surgery was 58.0 years (range 36-83). The procedures were performed with an oncologic indication in 67 cases (84%) and for nononcologic indications in 13 cases (16%). An exploratory analysis was conducted to determine whether any of the collected variables differed significantly between the two groups; however, no significant differences were found (Table 1). At the time of the procedure, none of the patients were on antiplatelet medications or anticoagulation therapy, as they were required to discontinue these medications 1 week before surgery and to abstain for at least 2 weeks after.
Demographics and Other Characteristics of the Study Population.
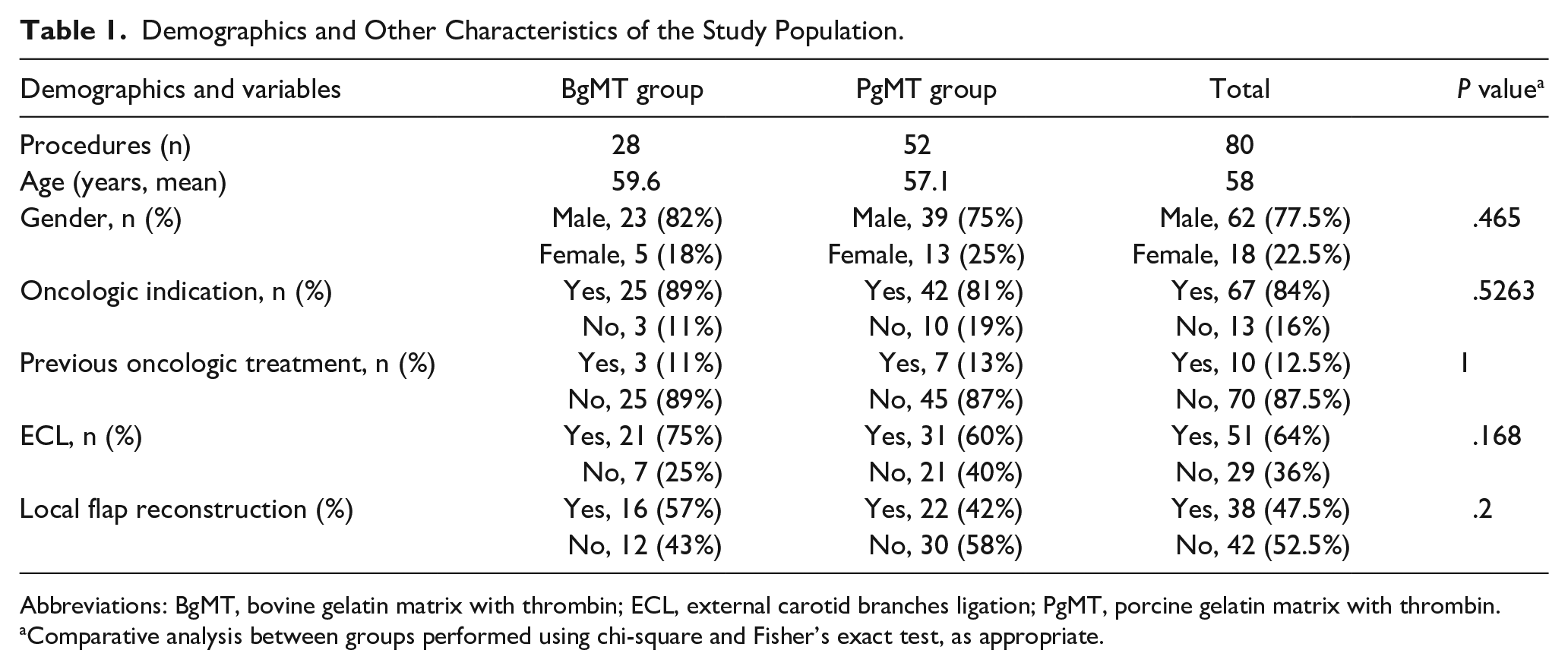
Abbreviations: BgMT, bovine gelatin matrix with thrombin; ECL, external carotid branches ligation; PgMT, porcine gelatin matrix with thrombin.
Comparative analysis between groups performed using chi-square and Fisher’s exact test, as appropriate.
During the span of 17 months, 28 cases were performed using BgMT as a hemostatic agent. This subgroup included 23 men and 5 women, with a mean age of 59.6 years (range 36-81). The primary indication for surgery was oncologic treatment in 25 cases (89%), while nononcologic indications were observed in three patients (11%), including two with severe lingual hypertrophy and one with a vallecular cyst. Three patients (11%) had undergone chemoradiation prior to the surgical procedure, while the majority had not (n = 25, 89%). The most prevalent oncologic indication was oropharyngeal carcinoma, accounting for 68% of cases (17 cases out of 25), followed by metastatic squamous neck cancer with an occult primary in 20% (5 cases). In addition, a case of supraglottic carcinoma in situ, one with oral cavity carcinoma, and an extensive sinonasal carcinoma were also identified. External carotid branches ligation was performed in 75% of cases (n = 21), and local flap reconstruction was performed in 57% (n = 16). Two minor episodes of postoperative hemorrhage were identified, along with a single episode of intermediate severity. Notably, two cases (7%) presented with severe postoperative hemorrhage and respiratory compromise (Table 2).
Postoperative Hemorrhagic Events Observed in Studied Groups.
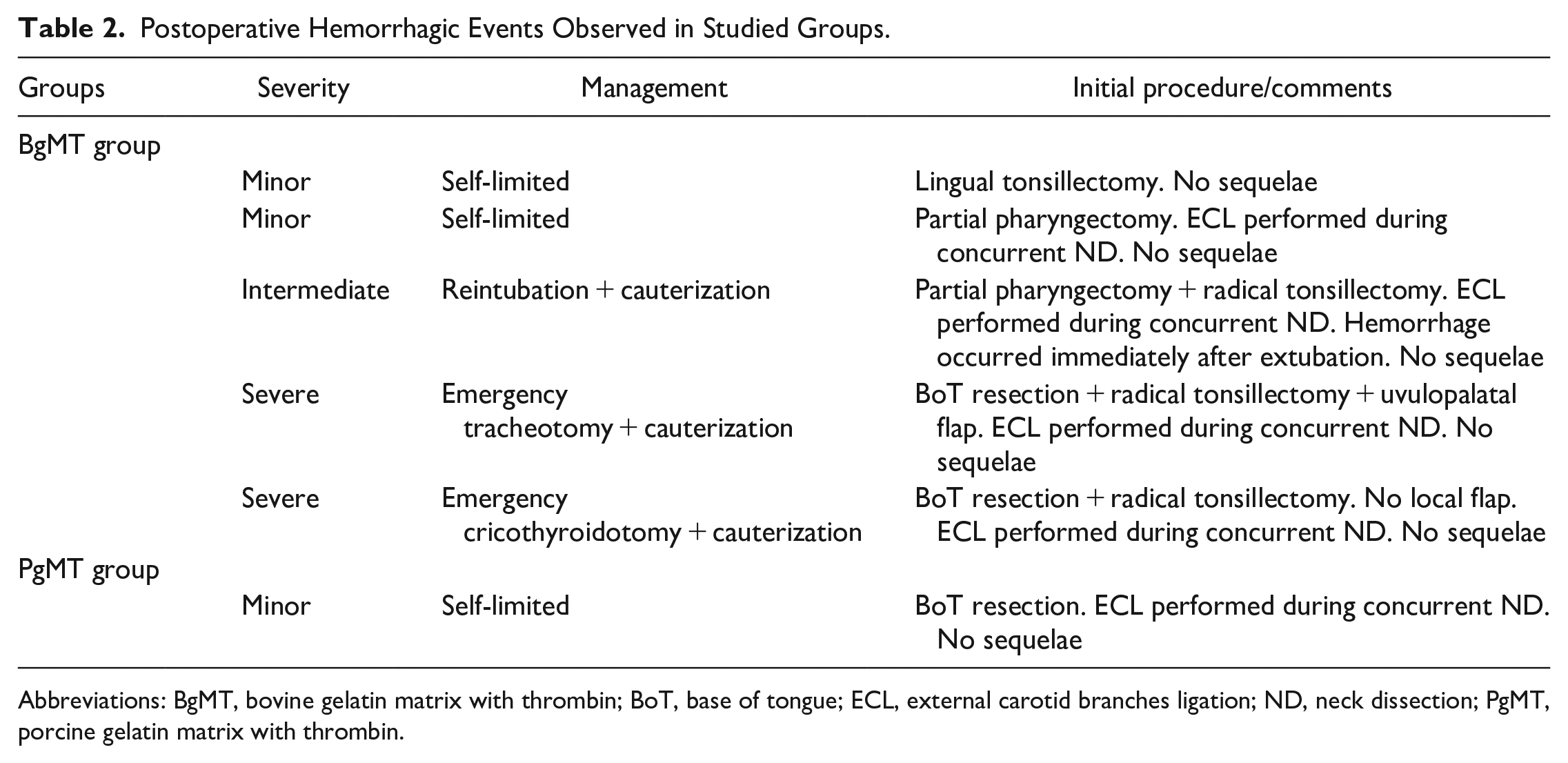
Abbreviations: BgMT, bovine gelatin matrix with thrombin; BoT, base of tongue; ECL, external carotid branches ligation; ND, neck dissection; PgMT, porcine gelatin matrix with thrombin.
After the introduction of PgMT, 52 cases were performed over a period of 34 months. This subgroup consisted of 39 men and 13 women, with a mean age of 57.1 years (range 40-83). The primary indication for surgery was oncologic treatment in 42 cases (80%). Nononcologic indications were observed in 10 patients (20%), including five with benign lesions (two laryngeal cysts, one parapharyngeal pleomorphic adenoma, one retropharyngeal lipoma and one benign retropharyngeal lymphadenopathy), four with severe lingual hypertrophy, and one with Eagle syndrome. The predominant oncologic reason for surgery was oropharyngeal carcinoma, accounting for 65% of cases (27 out of 42), followed by metastatic squamous neck cancer with an occult primary in 26% (11 cases). In addition, two cases of hypopharyngeal carcinoma, one oral cavity carcinoma, and a tonsillar sarcomatoid carcinoma were identified. Within the PgMT group, seven patients (13%) had received radiation before the TORS procedure. External carotid branches ligation was performed in 60% of cases (n = 31) and local reconstruction in 42% (n = 22) cases. A single instance of postoperative hemorrhage of minor severity was identified within this subgroup (Table 2).
The total rate of postoperative hemorrhage in the study population was 7.5% (n = 6), with major and severe hemorrhagic events occurring at a rate of 2.5% (n = 2). BgMT was used in 35% of cases (n = 28), while PgMT was employed in 65% (n = 52) of cases. The BgMT group exhibited a higher incidence of hemorrhagic events (n = 5, 17.8%), compared to PgMT (n = 1, 1.92%) and the difference was statistically significant (P = .0183). Conversely, no difference was observed for major or severe hemorrhagic events between the two groups (P = .1196; Table 3). Due to the limited number of patients experiencing this outcome of interest, performing a multivariate analysis to identify predictors associated with postoperative hemorrhage was not feasible.
Comparative Analysis of Hemorrhage Events Between Groups.
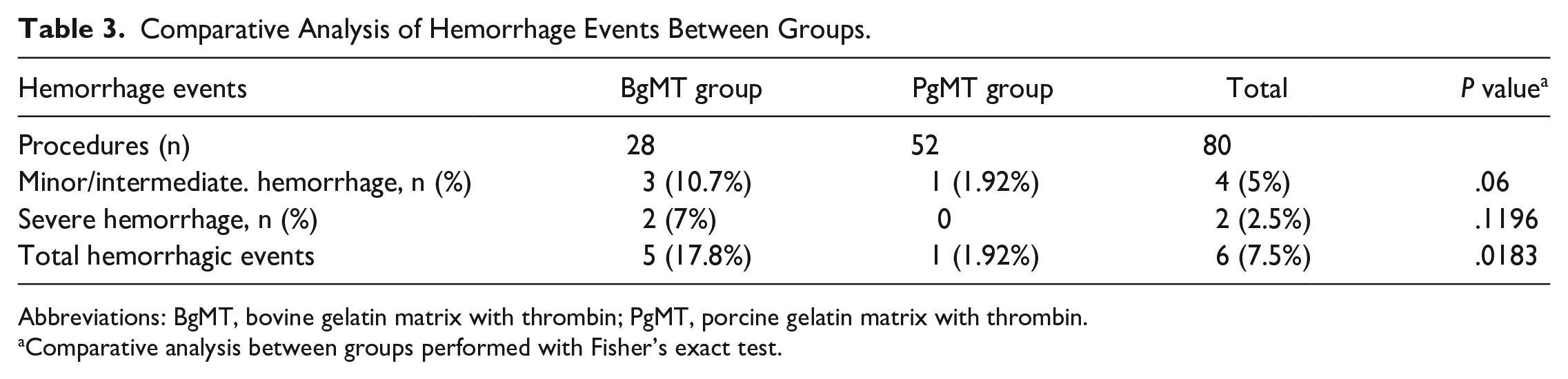
Abbreviations: BgMT, bovine gelatin matrix with thrombin; PgMT, porcine gelatin matrix with thrombin.
Comparative analysis between groups performed with Fisher’s exact test.
Ligation of the external carotid branches was performed in 51 of 80 cases (64%), always in the context of a neck dissection. The combination of facial, lingual, and ascending pharyngeal branches was ligated in at least 27 of these cases (53%), sometimes ligating the superior thyroid artery instead of the ascending pharyngeal. In our study, the two patients who had severe complications, had undergone ligation of external carotid branches during the original surgery (Table 3). One patient of the cohort had two procedures performed using BgMT, while another patient had two procedures performed different hemostatic agents each time. All patients who had received previous oncologic treatment underwent radiation with chemotherapy, except 1 who only underwent radiation.
Discussion
TORS poses a risk of postoperative upper airway hemorrhage, ranging from 1.5% to 13.1%.2-11 Recognizing risk factors for hemorrhage and understanding hemostatic techniques are complementary to the refinement of surgical techniques and a comprehensive understanding of local “inside-out” anatomy. 20 This integrated approach aims not only to enhance outcomes but also to foster a positive perception of TORS and contribute to its ongoing development.
Current hemostatic methods in TORS encompass the use of adjunct hemostatic agents, cauterization techniques, 21 hemoclips, 22 and preventive ligation of major vessels. Studies evaluating preventive ligation of external carotid branches reveal a lower risk of life-threatening severe or major postoperative hemorrhage, although it might not decrease the incidence of total postoperative bleeding events.2,23,24
Since ancient times, different materials such as wax or herbs have been applied to wounds to aid in the control of hemorrhage. 25 Available topical hemostatic agents can be grossly classified into 2 main groups: physical and biologically active agents. Physical agents provide a mechanical matrix to accelerate clot formation and provide local compression, while biological active agents are generally fibrin or thrombin-based and directly activate the common pathway of the coagulation cascade. 26 Flowable hemostatic agents are formed by a combination of gelatin and thrombin. Gelatin works as a passive hemostat with mechanical properties, while thrombin plays the role of an active hemostat, cleaving fibrinogen to fibrin. 27 There are many reports of their safe use in the oropharynx area, especially during tonsillectomies. 28
The use of both flowable hemostatic agents in TORS has also been described,17-19 but the scientific literature that evaluates their efficacy in reducing the risk of postoperative hemorrhage is lacking. Previous studies have tried to establish a comparison in clinical outcomes between BgMT and PgMT, most of them supporting hemostatic equivalence in spinal surgery and partial nephrectomies.29-31 On the other hand, Slezak et al 32 observed that BgMT was superior to PgMT in a high-volume bleeding porcine model, and adjudicated this difference to a higher dry mass per unit volume and to the smooth structure of the BgMT particles. This configuration potentially allows for increased thrombin retention, compared to the stellate structure of PgMT particles. 32
In a previously reported series of 17 TORS cases using BgMT, a singular case of postoperative hemorrhage was documented. 19 Our study, which included 80 procedures, revealed a reduced incidence of total postoperative hemorrhage after adopting PgMT (n = 1) compared to BgMT (n = 5). Although a statistically significant difference was identified (P = .0183), caution is warranted in interpreting these findings due to the predominantly minor nature of the reported events, which are self-limited by definition, and could be particularly susceptible to underreporting.
The overall rate of severe postoperative hemorrhage (2.5%) in our series aligns with the literature.2,3 BgMT was used in the two cases that presented severe postoperative hemorrhage (Table 2), while no major or severe events were observed in the PgMT group. No significant difference was found for major or severe events between the groups (P = .1196; Table 3).
We observed a significant reduction in total events (P = .0183) after PgMT was introduced, and although no statistical difference was found, there was a trend in the reduction of minor and intermediate events. In general, our findings suggest that topical agents could help reduce the frequency of non-life-threatening hemorrhage events. However, they are possibly equivalent in their ability to prevent severe events, indicating that they are likely inconsequential. It is important to note that topical agents only temporarily remain at the wound site and are eventually swallowed. Thus, their potential benefits might be limited to the first days after surgery when the patient’s swallowing capacity is limited.
This study had several limitations. We did not control for certain variables such as comorbidities, the extent of resection, and some alternative hemostatic techniques such as hemoclips. In addition, there is a potential for underreporting of minor postoperative hemorrhage, given its self-limited nature, which may contribute to the observed disparity between groups. Moreover, the reduced rate of complications observed between the two groups could be attributed to the ascending learning curve of the senior author.
Larger and more controlled studies are needed to assess the impact of these agents on postoperative outcomes. But to our knowledge, no other studies actively compare the efficacy of topical hemostatic agents in TORS procedures. The use of hemostatic agents should also reduce the degree of morbidity associated with cauterization, including postoperative pain, while providing complementary ways to hasten bleeding control. 31 The considerable risk of airway hemorrhage and its high potential for morbidity and mortality more than justify their relatively low cost.
Footnotes
Acknowledgements
The authors thank Kristin Delfino, PhD, and Kristal Adams, BA, CCRP, for their support with the statistical analysis.
Authors’ Note
The current work was presented as a poster at the AHNS 10th International Conference on Head and Neck Cancer; Chicago, IL; June 22 to 25, 2021.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Springfield Committee for Research Involving Human Subjects, with an exemption of informed consent (20-618 on August 11, 2022). No specific consent is required for the statistical analysis of aggregated deidentified data. For this study, the raw data were extracted from Health Information System (HIS), and patient identities were de-identified.