
Abstract
Objectives:
We describe our experience with long process incus (LPI) necrosis in revision stapedotomy and discuss the different management methods proposed in the literature to identify surgical techniques that can lead to satisfactory results over time.
Methods:
Twenty-two stapedotomy revisions, in 21 patients with the necrosis of the long process of the incus, are performed from 1997 to 2017. In cases of erosion or minimal necrosis of LPI, a new prosthesis of the same type or an angled prosthesis was applied higher on the residual incus stump. In cases of partial necrosis of LPI, a Donaldson type ventilation tube reshaped and placed on the residual incus stump to stabilize prosthesis, or glass ionomer bone cement was used. In cases of subtotal necrosis of LPI, a cup piston prosthesis in polycel was applied on incus residual stump. Pre- and postoperative (≥1 year) pure tone audiometry was performed for all cases. Air conduction threshold, bone conduction (BC) threshold, and air-bone gap (ABG) were documented according to the American Academy of Otolaryngology Head and Neck Surgery Committee of Hearing and Equilibrium guidelines.
Results:
At 1-year follow-up, postoperative ABG was reduced to ≤10 dB in 13 (59%) cases and ≤20 dB in 19 (86.4%) cases. The mean postoperative ABG significantly decreased in each group. There was no significant change in postoperative BC thresholds, and there were no cases with postoperative SNHL.
Conclusion:
Excellent functional results can also be achieved in cases of long incus process necrosis. The choice of technique should be considered according to the degree of necrosis. Piston replacement with the same type or angled type prosthesis, in cases of erosion or minimal LPI necrosis, and modified Donaldson type ventilation tube, in cases of partial LPI necrosis, provided excellent hearing results.
Introduction
Multiple studies have demonstrated the high success rate of primary stapedectomy for otosclerosis in closing the air-bone gap (ABG) and achieving excellent hearing results.1-9 In a small percentage of cases, hearing may deteriorate over time, necessitating revision surgery.4,10 The literature presents 4 reasons for revision surgery: persistence of an ABG or reopening of this gap, sensations of instability, sound distortions, and neurosensory deafness. 10
Common findings during revision stapedectomy include necrosis of the long process of the incus, prosthesis lateralization or displacement away from the oval window, re-fixation of prosthesis, loosening of the connection between the prosthesis and incus, and closure of the fenestra in the oval window.10-16 The incidence of long process incus (LPI) necrosis in revision stapedectomy ranges from 5% to 49%,5,8,12,15,17-25 and in some studies, it was the first cause of failure.5,25
Hearing results in revision surgery have been poorer than those of primary stapes surgery.4,5,10,15,16,20,26 Several surgical techniques have been proposed for hearing recovery in cases of necrosis of long process of the incus.4,5,10,24,26-30 For cases of erosion and minimal compromise of the long process of the incus, standard primary stapes surgery techniques may be employed.4,5,10-29 Reconstruction of LPI with bone cement for the restoration of natural incus–oval window interface may be useful option for revision surgery.4,5,24,26,28,30 For those cases with a shortened incus, bypass techniques have been described such as bypassing the necrotic incus via either footplate extraction with total ossicular reconstruction prosthesis placement or malleovestibular prosthesis placement.5,9,26,28,29,31,32
We share our experience with LPI necrosis in revision stapedotomy and discuss the different management methods proposed in the literature in order to identify surgical techniques that can lead to satisfactory results over time.
Patients and Methods
This retrospective clinical study included 22 (range 14-64 years, of which 58% women and 42% men) cases of revision stapedotomy, in 21 patients, for LPI necrosis, conducted by Otolaryngologists—Head and Neck surgeons of Vanvitelli University, from 1997 to 2017.
The patients had previously undergone (at least 15 months before) stapedotomy with piston prostheses insertion (platinum fluoroplastic Smith & Nephew Richards inc, in 8 cases; platinum-PTFE Spiggle & Theiss piston prosthesis in 7 cases; Medtronic “big easy piston platinum titanium” in 6 cases; the piston had a diameter of 0.6 mm and a length of 4.5 mm in 17 cases and 4.75 in 4 cases). The closure of the ABG within 10 dB occurred in 95.2% of cases (20 of 21 patients) at 500, 1000, 2000 and 3000 Hz.
Fifteen cases of primary surgeries were performed at our institution, and 6 cases were performed elsewhere. The reappearance of conductive hearing loss (CHL) with ABG >20 dB, after an initial good hearing result, is the main reason for revision (20 cases, 95.2%). Persistent CHL with ABG >20 dB is an indication to the intervention in only one case (4.8%).
Of 22 revision stapes surgeries, 21 were primary revision surgery, 1 was secondary revision surgery, on the same ear. All patients are operated, by the same surgeon, via the transcanal approach under local anesthesia. After exploring the middle ear, the prosthesis was removed.
At this point: in cases of erosion or minimal necrosis of LPI (incus is often still in continuity):
– In 9 cases (group 1), a new prosthesis of the same type was repositioned higher on the residual incus stump;
– in 6 cases (group 2), of which the only second revision case, an angled prosthesis “the big easy piston ear platinum titanium” was applied, left in 5 cases, right in 1 case
in cases of partial necrosis of LPI (there are no objective criteria for defining “partial” necrosis, LPI crosses the margin of the oval window):
– in 3 cases (group 3), a Donaldson type ventilation tube (Xomed-Treace Inc. 1.14 diameter mm, Silicone) was reshaped and placed on the residual incus stump to stabilize prosthesis, according to El Seifi technique (Figure 1);
– in 2 cases (group 4), glass ionomer bone cement was used; the prosthesis (platinum-PTFE Spiggle & Theiss piston prosthesis) was reinserted to the remaining LPI and then fixed to LPI using the cement
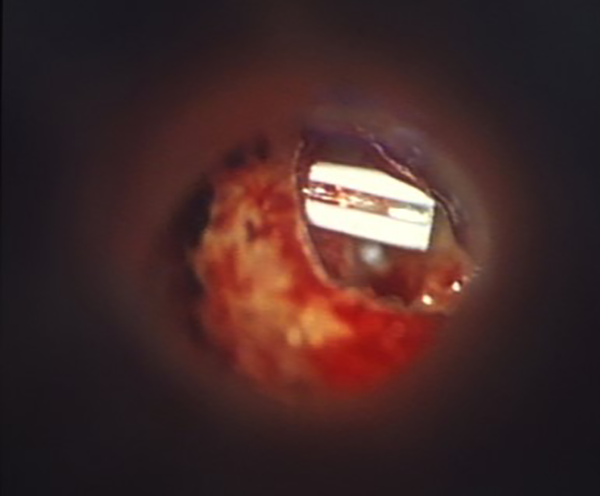
Donaldson type ventilation tube reshaped and placed on the residual incus stump to stabilize prosthesis, according to El Seifi technique.
in 2 cases of subtotal necrosis (the incus stump reaches the margin of the oval window, group 5) of LPI, a cup piston prosthesis in polycel was applied on residual incus stump (Incus necrosis strut-Xomed Treace) after performing a stapedectomy with vein graft to cover the oval window.
Pre- and postoperative (≥1 year) pure tone audiometry was performed for all cases. Air conduction (AC) threshold, bone conduction (BC) threshold, and ABG were documented.
Mean follow-up was 24 months (12-53 months). Hearing results were reported according to the American Academy of Otolaryngology Head and Neck Surgery Committee of Hearing and Equilibrium guidelines for the evaluation of results of CHL treatment. 33 Air-bone gap was analyzed at 0.5, 1, 2, and 3 kHz. Successful hearing was defined as a postoperative ABG ≤20 dB. 33
Statistical Analysis
Student t test was used to compare the means of the pre- and postoperative hearing results. P values of <.05 were considered to be statistically significant.
Results
Postoperative hearing results, at 1-year follow-up, showed:
– In the 22 stapedotomy revision cases, the postoperative ABG reduced to ≤20 dB in 19 cases (86.4%) and to ≤10 dB in 13 cases (59%).
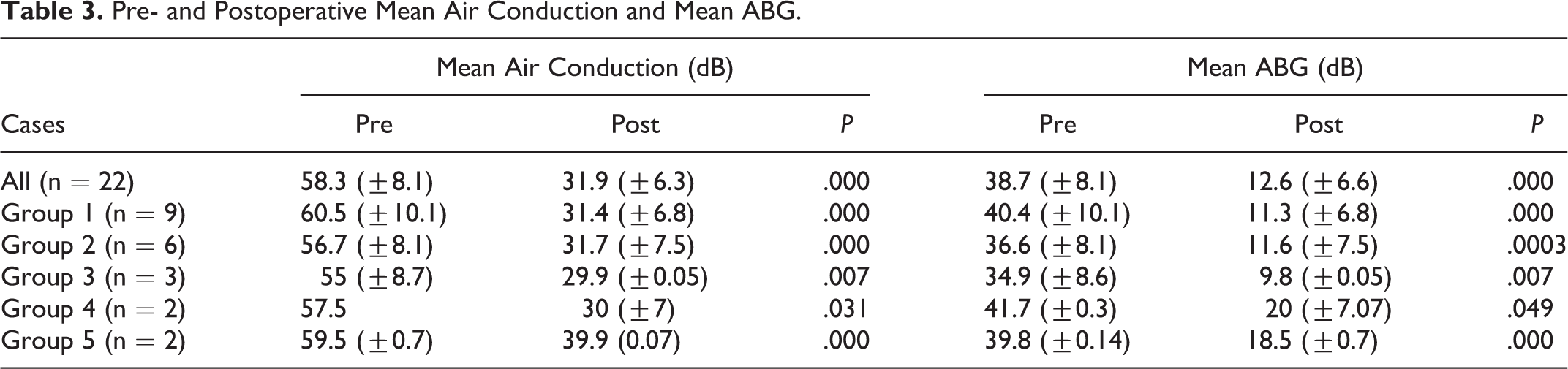
– The mean preoperative AC threshold was 58.8 (±8.1) dB, 60.5 (±10.1) dB, 56.7 (±8.1) dB, 55 (±8.7) dB, 57.5 dB (±0.0), 59.5 (±0.7) dB for all cases, group 1, group 2, group 3, group 4 and group 5, respectively. The mean postoperative AC threshold was 31.9 (±6.3) dB (P < .05), 31.4 (±6.8) dB (P < .05), 31.7 (±7.5) dB (P < .05), 29.9 (±0.05) dB (P < .05), 30 (±7) dB (P < .05), and 39.9 (±0.07) dB (P < 0.05), respectively. There was a significant improvement in the mean postoperative AC threshold of all groups.
– There was no significant change in the mean postoperative BC threshold of all groups.
– In 9 cases with piston prosthesis replacement higher up to the residual incus stump, the ABG closure reduced to ≤10 dB in 6 (66.7% of cases) of 9 patients and to ≤20 dB in 8 of 9 cases (88.9% of cases); in 6 cases with angled titanium prosthesis placement, the ABG closure reduced to ≤10 dB in 66.6% (4/6) of cases and to ≤20 dB in 83.3% (5/6); in 3 cases with piston prosthesis and Donaldson type ventilation tube, the ABG closure reduced to ≤10 dB in 100% of cases; in 2 cases with glass ionomeric cement application, the mean postoperative ABG was ≤20 dB in one case (50%), and >20 dB in the other case (50%), there was no case with ABG ≤10 dB; in 2 cases of cup piston polycel prosthesis, the mean postoperative ABG was ≤20 dB (100%); there was no case with ABG ≤10 dB.
– The repositioning of a new prosthesis higher up on the incus stump (overall, angled, and not) allows an ABG closure within 20 dB in 13 (86.7%) of 15 cases and within 10 dB in 10 (66.7%) of 15 cases with limited LPI necrosis.
– In cases of shortened LPI, ABG closure within 20 dB is obtained in 4 (80% of cases) of 5 patients: in 50% of cases with glass ionomer cement application and in 100% of cases with use of reshaped Donaldson type ventilation tube, an ABG closure within 10 dB is obtained in 3 (60%) of 5 cases, all cases with reshaped Donaldson type ventilation tube application.
– In cases of subtotal LPI necrosis, ABG closure within 20 dB is obtained in 100% of patients (100%); there was no case with ABG ≤10 dB.
– In 3 cases, the mean postoperative ABG was >20 dB (15%): in one case treated by replacement of piston prosthesis and glass ionomeric cement and in one case with repositioning of piston prosthesis with standard technique, and in the same case, but in second revision surgery, with application of angled prosthesis.
– There were no cases with postoperative SNHL.
Hearing results are shown in Tables 1-3.
Pre- and Postoperative ABG.
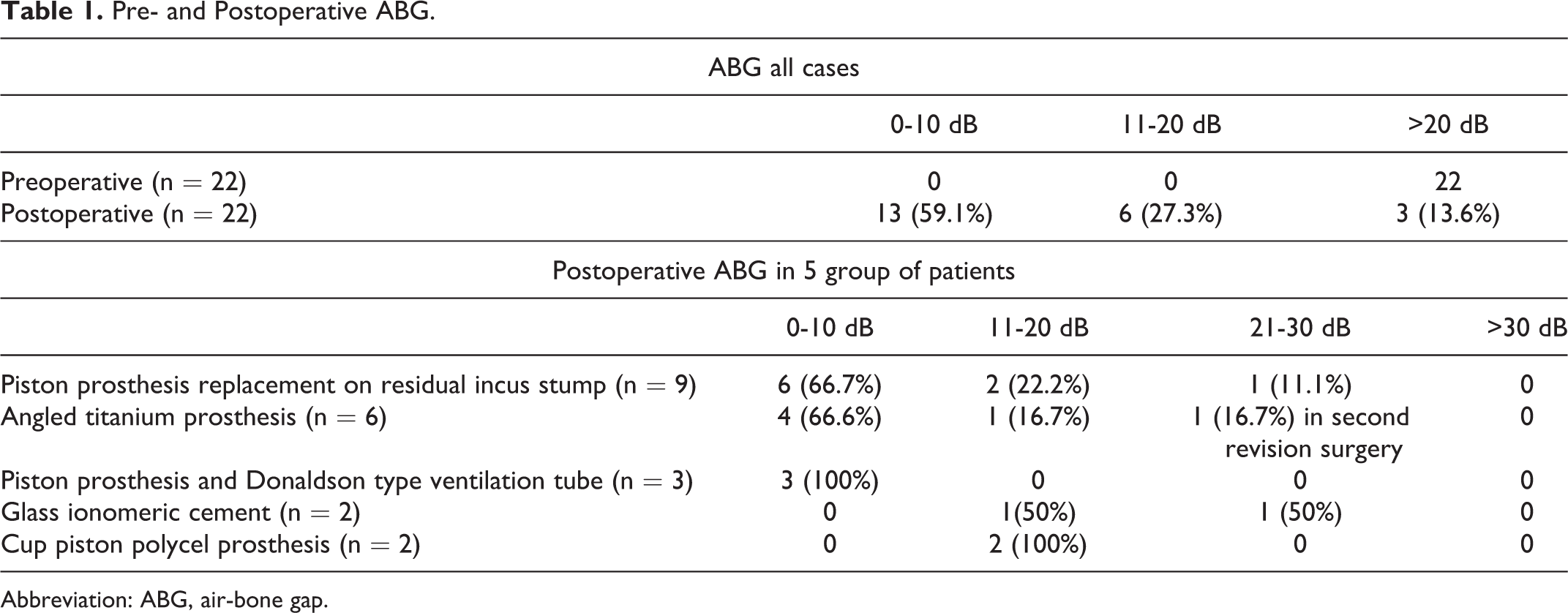
Abbreviation: ABG, air-bone gap.
Air-Bone Gap and Degree of Necrosis.
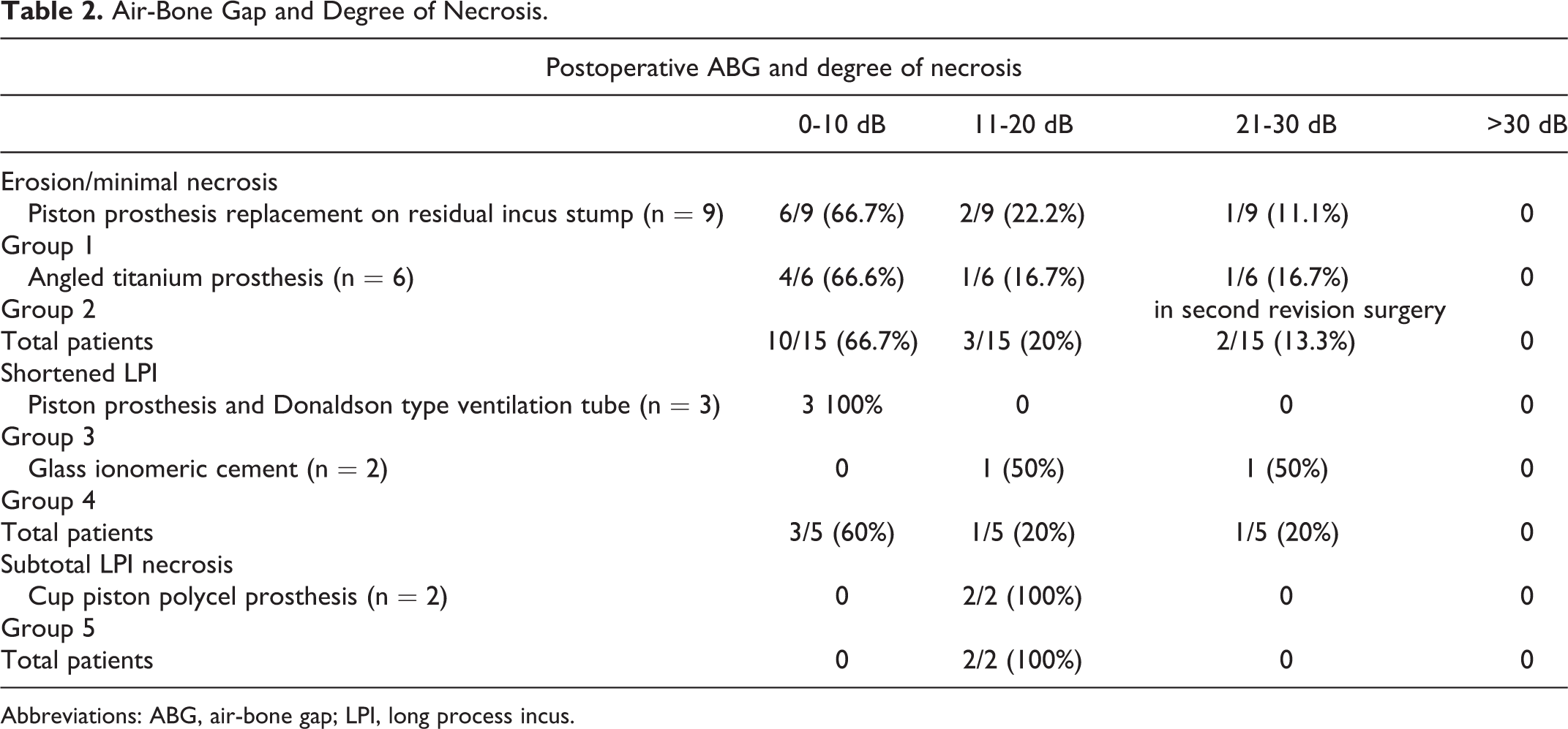
Abbreviations: ABG, air-bone gap; LPI, long process incus.
Pre- and Postoperative Mean Air Conduction and Mean ABG.
No patient experienced tinnitus and persistent postoperative vertigo; there were no complications reported in relation to the use of bone cement as otorrhea or granulations.
Discussion
Over the last 2 decades, the outcomes of stapedectomy revision surgery have improved but continue to be worse than those of primary surgery.4,5,9,10,15,16,20,26 Today, less than 20-dB ABG results are achieved in 64% to 96.3%, and 0% to 2% of patients go on to have profound sensorineural hearing loss, or a dead ear, postoperatively.8,27,29,34
Incus necrosis is among the most common causes of stapedectomy failure,12,15,26,35,36 and its management in revision stapedectomy is challenging. The literature shows that the incidence of LPI necrosis in revision stapedectomy ranges from 5% to 49%.5,8,12,15,17-24 Theories for why this occurs vary but include overly zealous crimping, loss of blood supply, or a poorly fit prosthesis causing inflammation and bone erosion over time.12,37,35,36 All techniques of ossicular reconstruction should be considered in case of incus necrosis. For cases of erosion and minimal compromise of the long process of the incus, standard primary stapes surgery techniques, with a longer wire prosthesis that attaches to the incus higher up on the long process, may be employed.4,27,29,37 For those cases with a shortened incus, bypass techniques have been described to overcome the incus necrosis.4,5,9,26-29,32,34,38,39
If there is too much erosion of incus to allow the fitting of any prosthesis, a final option is to bypass the incus and attach the prosthesis directly to the malleus.4,5,28,29,34,37 In many earlier series, malleovestibulopexy (connecting malleus to the vestibule) was the technique of choice, using either prosthesis or malleus relocation with reshaped incus.4,5,10,28,29,34,37 However, prosthesis positioning is technically challenging and has a potentially higher incidence of vertigo and SNHL after surgery.29,40
Hearing outcomes have been mixed. An ABG ≤10 dB was obtained in 59% of our cases. This rate varies between 18% and 80% in the literature. One-year postoperative results with ABG closure to less than 10dB have ranged from 18% to 60% with malleostapedotomy techniques,4,28,29,32,31 from 30% to 54% for cases employing prostheses that engage the shortened incus.4,28,29,31 Mangham, in a revision stapedotomy study, demonstrated that an ABG of 10 dB or less, at 1 year of follow up, in patients in which the new device was yet again attached to a normal incus, necrotic incus, or malleus, had similar success rates, ranging from 47% to 54%. 29 Even if attaching the new device to the malleus was more stable, maintaining success for a median of 75 months, malleus attachment was not the obvious solution to revision stapedectomy in all cases of incus necrosis because the procedure is more difficult than incus attachment and has almost a 5-fold greater risk of inner ear damage. 29
An ABG ≤20 dB has been reported in 64% to 96.3% of cases.4,8,28,29,30,31 Our success rate of 86.4% can be considered acceptable.
In 9 (47.4%) cases, in our series, with erosion or minimal necrosis, it was possible to reposition a piston prosthesis higher up on the incus stump. Teflon piston were used in 5 cases and titanium prosthesis in remaining 4 cases. An ABG ≤20 dB was obtained in 8 (88.9%) of 9 cases and ≤10 in 6 (66.7%) of 9 cases.
In 6 cases, of which one in second revision, angled titanium prostheses were placed. An ABG ≤20 dB was obtained in 5 of the 6 (83.3%) cases and ≤10 in 4 cases (66.6%). Secondary revision surgery, with angled prosthesis placement, was performed on a single patient after the initial revision with piston Teflon prosthesis placement. Six months after our initial revision stapedectomy with piston Teflon prosthesis, a CHL redeveloped. Despite a second revision, there was a persistent conductive loss. One-year postoperative results with ABG closure to less than 10dB has ranged, in the literature, from 30% to 54% for cases employing prostheses that engage the shortened incus.4,28,29,31 Yetiser asserts that incus necrosis is the result of vibratory movements at the prosthesis–incus contact site due to flaccid prosthesis or restenosis of the oval window constricting the prosthesis. 16 Anatomic study of Toth et al revealed wide variations of diameters and shape of the LPI. Best possible crimping of stapes prosthesis depends not only on the shape and diameters of the LPI but also on the vertical surface of the LPI as well. To prevent incus necrosis due to compression of the feeding blood vessels, the maximum contact surface of the loop of stapes prosthesis should be about 1.9 mm in length. 41
Over the last decade, bone cements have been introduced as an adjunct to ossicular chain reconstruction and have been used when incus necrosis is encountered in cases of chronic otitis media and revision stapedectomy. Glass ionomer and hydroxyapatite bone cements have been used to reconstruct LPI necrosis in revision stapedectomy.4,5,26,28-30 If ionomer cements are used, footplate and facial nerve should be covered with pieces of gelfoam to protect them from potential reaction to the cement. 5 In our study, 2 cases of incus restoring with glass ionomer bone cement were performed; the prosthesis (platinum-PTFE Spiggle & Theiss piston prosthesis) was reinserted first to the remaining LPI, and bone cement was placed on the lateral surface of the incus long process to fix the prosthesis. There were no complications with respect to the use of cement. In these cases, the postoperative ABG is >20 dB in 1 (50%) case and ≤20 in the other case (50%). There was no case with ABG ≤10 dB.
Hearing outcomes using cements for ossicular reconstruction have been variable, cases number small, and follow-up limited. Feghali et al 42 examined 4 cases of incus necrosis reconstruction using ionomeric cement and found ABG closure to within 10 dB in a single patient. Chen and Arriaga 43 reported an ABG closure to within 10 dB in 4 (57.1%) of 7 cases of long-process incus erosion where ionomeric cement was used to reconstruct the incus remnant, whereas in the other 3 cases, the postoperative ABG exceeded 20 dB. Gonim reports a mean postoperative ABG improvement from 38.6 (±4.8) to 9.3 (±3) dB with glass ionomer bone cement plug technique with an ABG closure to within <10 dB in 22 (81.5%) cases. 5
For those cases with a shortened or subtotal LPI necrosis, bypass techniques have been described to overcome the incus necrosis.4,5,9,26-29,32,34,38,39
In 3 cases of partial incus necrosis, a Donaldson type ventilation tube (1.14 diameter mm, Silicone; Xomed-Treace Inc) was reshaped and placed on the residual incus stump to stabilize prosthesis (Figure 1). The ABG closure reduced to ≤10 dB in 100% of cases. El Seifi 27 in 1996 proposes this technique in which the original prosthesis is replaced on the stump, a segment of Silastic tube 4-mm long and 1.3 mm in diameter is slit on one side halfway along its length and is threaded over it along the incus stump, with the slit facing medially and superiorly so that it engages the wire. The tube with the wire loop is pushed superiorly as far as it goes until it engages the thicker proximal part of the stump and grasps it by its recoil. Six (86%) of the 7 operated-on cases had complete closure of the ABG over the follow-up period (3 months to 3 years).
This method, proposed by El Seifi 27 and adopted by our Institution, offers an easy, effective, and inexpensive solution to a difficult problem. Some techniques require a stapedectomy and the use of prostheses to be inserted on the incus residual stump, such as the polycel cup implant or the modified Robinson prostheses. 39
In 2 cases of subtotal necrosis of LPI, in our study, a polycel cup piston prosthesis implant (Incus necrosis strut-Xomed Treace) provides an ABG closure within 20 dB in 100% of cases; there was no case with ABG ≤10 dB.
The limits of this study are the retrospective design, the small number of cases for each group and the lack of objective criteria in defining the minimal or partial necrosis.
Conclusion
The study shows that even in cases of long incus process necrosis, it is possible to obtain excellent functional results. The choice of technique should be considered according to the degree of necrosis. Piston replacement with the same type or angled type prosthesis, in cases of erosion or minimal LPI necrosis, and modified Donaldson type ventilation tube, in cases of partial LPI necrosis, provided excellent hearing results.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.