
Abstract
The aim of this study was to investigate the functional results of glass ionomer cement (GIC) and incus transposition (IT) used for treatment of incus long process defects in pediatric patients. The medical records of 40 patients, aged 10 to 16 years, who underwent ossicular reconstruction due to incus long process defect between January 2010 and July 2017 were reviewed for age and gender, types of ossiculoplasty technique, types of graft used for tympanic membrane repair, preoperative–postoperative audiological examinations, and length of follow-up. The mean preoperative air-bone gap (ABG) was 29.40 (8.47) dB, the mean postoperative ABG was 15.25 (8.55) dB in the entire group, and the difference was statistically significant (P < .001). The functional outcome (ABG ≤ 20 dB) was 80% (32 patients) in the entire group. The mean hearing gain was 18.83 (9.43) dB and postoperative mean ABG was 20 dB or better in 17 (94.4%) patients in the GIC group. The mean hearing gain was 10.31 (9.44) dB, and postoperative mean ABG was 20 dB or better in 14 (63.6%) patients in the IT group. The mean hearing gain was significantly higher in the GIC group than in the IT group (P = .026), and the postoperative mean ABG was significantly higher in the IT group than in the GIC group (P = .045). The functional success rates were significantly higher in GIC group than in IT group (P = .020). There were no statistically significant differences between groups in terms of postoperative speech reception threshold and word recognition scores (P = .628, P = .260, respectively). The graft success rates were 94.4% (17 patients) in the GIC group and 90.9% (20 patients) in the IT groups. There was no statistically significant difference between groups in operated side (P = 1.000). Reconstruction of small incus long process defects using GIC is a valuable technique and can be safely used in pediatric patients. The hearing outcomes are significantly better in GIC rebridging technique when compared with a sculpted IT technique.
Introduction
The ossicular chain transmits the vibration of tympanic membrane (TM) effectively to the inner ear fluids. A discontinuity of the ossicular chain disturbs the energy transfer and results in a conductive hearing loss. It is well known that unilateral hearing loss has important consequences in pediatric population. The presence of hearing loss in early childhood has negative effects on the development of language, speech, and learning skills in this population, and these children have such difficulties with achieving their academic potential precisely. One of the most common cause of unilateral hearing loss in children is ossicular chain defect due to chronic otitis media with or without cholesteatoma, adhesive otitis media, and retraction pockets. The most common encountered ossicular chain defect in otologic surgery is the erosion of the long process of incus with otherwise intact ossicular chain. In 1960, Austin 1 reported that isolated incus defect with an intact malleus and stapes suprastructure was present in 60% of ossicular defects.
The optimum ossicular reconstruction technique should be relatively easy to perform and also has acceptable hearing outcomes. The ideal ossiculoplasty material should be easy to position, biocompatible, cost-effective, and stable in its position. Since the first introduction of ossiculoplasty in 1950s, various innovative materials and surgical techniques have been used to repair incus defects including interposition of a biological autograft or allograft (eg, sculpted incus, cortical bone, cartilage), partial ossicular replacement prosthesis, Teflon plastics, bioinert and bioactive ceramics, titanium and gold metals, and biocement (eg, glass ionomer cement [GIC], phosphate cement, carboxylate cement, silicate cement). 2 There has been no single ossicular reconstruction method that received universal acceptance due to all methods have advantages and disadvantages.
Autograft incus transposition (IT) technique was first introduced by Hall and Rytzner 3 in 1957 and it has been widely used thereafter. Classic incus interposition technique had high graft displacement rates, and the hearing outcomes were frequently poor with this technique. Later studies showed that graft displacement rates reduced to a great extent when the incus was sculpted by proper drilling and shaping for its engagement stapes head and fitting the malleus handle. In this way, the sculpted incus became popular. 4
Glass ionomer cement was first used by dentists for repair of dental pathologies. Recently, it has been frequently used by otologist and neuro-otologist for ossicular chain reconstruction, stabilization of implantable devices (Teflon piston, ossicular implant, etc), mastoid obliteration and repair of bony defects of tegmen, external ear canal, or skull base. 5
Although the outcomes of the repair of incus long process defects using GIC rebridging and IT technique are widely discussed in adults, 6 -9 there is a paucity of study investigating the results in the pediatric population. This study aimed to evaluate and compare the anatomical (graft take) and functional results (hearing threshold, air-bone gap [ABG], hearing gain) in pediatric patients treated with GIC and IT ossiculoplasty at our tertiary center.
Patients and Methods
Forty pediatric patients aged between 10 and 16 with an incus long process defect and intact malleus and stapes superstructure were included in this study, of 157 pediatric patient who had undergone surgery due to chronic otitis media in our center between January 2010 and July 2017. The retrospectively collected data included patients’ age and gender, types of ossiculoplasty material (GIC, IT), and preoperative and postoperative audiological examinations.
Our exclusion criteria were revision surgery, failed TM closure, stapes or malleus fixation, traumatic ossicular dislocation, tympanosclerosis or cholesteatoma, and additional malleus or stapes defects. All patients were followed up at least 12 months.
The study was approved by the local ethics committee (no: E-18-1907) and conducted in accordance with the ethical principles described by the Declaration of Helsinki.
Patients were classified 2 groups according to type of ossiculoplasty technique they received: GIC (group 1), and IT (group 2). Temporalis muscle fascia graft was used for the closure of TM perforation.
All patients underwent preoperative and postoperative (at 6 months) pure tone audiometry measurements at 0.5, 1, 2, and 4 kHz and at 3 kHz frequencies using an Interacoustic AC-40 (Middelfart, Denmark) clinical audiometer. The average of the values at 2 and 4 kHz was used to calculate the value for 3 kHz. Preoperative and postoperative air and bone conduction thresholds, speech reception thresholds (SRTs), and word recognition scores (WRS) were measured at the 4 frequencies. The ABG was calculated as the average difference between the air and bone conductions at 4 frequencies (0.5, 1, 2, and 3 kHz). 10 A successful functional result was defined as a postoperative ABG of ≤20 dB.
Postoperative follow-up controls were generally performed at the hospital at 1, 3, 6, and 12 months and annually thereafter. Anatomical success was defined as an intact TM without medialization, lateralization, or perforation.
Statistical data analysis was performed using SPSS 21 (SPSS Inc; IBM Company, Chicago, Illinois). Data were expressed as mean (standard deviation) and as proportion (%). Chi-square test was used for comprising of categorical data. Mann-Whitney U test was used for nonparametric variables, whereas paired sample t test was used for parametric variables. A P < .05 was accepted as statistically significant.
Surgical Techniques
All operations were performed via an operating microscope (Möller-Wedel Optical, Hamburg, Germany) under general anesthesia. All surgical procedures were performed by the senior author (R.O.K.). We used postauricular approach to expose the middle ear cavity, and a mastoidectomy was performed when necessary. Following the exposure of the middle ear cavity, ossicular chain status was evaluated. In cases where the ossicular chain could not be visualized accurately, a minimal atticotomy was performed and the atticotomy defect was repaired with a small piece of conchal cartilage at the end of surgery. In cases with an incudostapedial gap larger than two-thirds the length of the incus long process, we performed IT technique for the reconstruction. If the gap between the incus remnant and the stapes head was less than one-third the length of the incus long process, we used GIC.
In group 1, incudostapedial gap was repaired with GIC (Ketac-Cem, Espe Dental AG, Seefeld, Germany). Glass ionomer cement contains a sterile powder and a dissolving liquid. These 2 components were mixed on a metal plate with a blunt pick for about 30 seconds until the mixture became muddy. An exothermic reaction occurs following the mixture of components. The mixture must be used within 2 to 4 minutes since it gets harden within 7 to 10 minutes. Before application of GIC, any blood or the mucosa over the stapes suprastructure and over the incus remnant must be removed to obtain a dry surface on which GIC adheres properly. Small pieces of absorbable sponges were placed into the middle ear cavity to prevent accidental contact of GIC and middle ear surfaces. The prepared GIC mixture was placed between incus remnant and stapes suprastructure with a microhook. The hardness of GIC was evaluated with a pick, and the movement of ossicular chain was evaluated by gentle pressure on the malleus handle and the observation of the synchronous movement of the stapes and round window membrane.
In group 2, ossicular chain defect was repaired with sculpted IT technique. After observation of the incus defect, the incudomalleolar joint was detached with an angled hook, and the incus was removed with an alligator forceps. Later, the remnant long process of incus was removed completely, and an acetabulum was created in its stump using a diamond burr to engage stapes head. A small groove was created on the body of incus using a diamond burr to fit the handle of malleus. The sculpted incus was placed between stapes head and handle of malleus. Absorbable sponges were placed all around the transposed graft to support it and prevent fixation to the posterior wall.
Finally, middle ear cavity was packed with absorbable sponges and the graft material (temporalis fascia) was placed medial to the TM remnant. The external ear canal was filled with absorbable sponges to support the graft laterally.
Results
A total of 40 pediatric patients (19 female, 21 male) with 40 operated ears (26 left, 14 right) who met the criteria mentioned above were included in this study. The mean length of follow-up was 26.25 (14.80) months ranged from 12 to 60 months. The mean age was 12.97 (1.59) in the entire group and ranged from 10 to 16 years. There were 18 patients in the GIC group and 22 patients in the IT group. The demographic information of patients in the GIC and IT groups was presented in Table 1.
Characteristic of Patients in the GIC and IT Groups.a
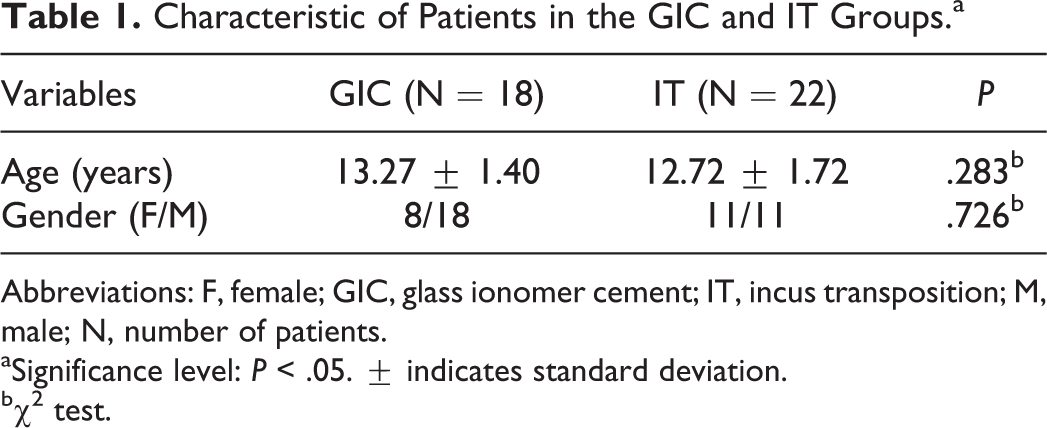
Abbreviations: F, female; GIC, glass ionomer cement; IT, incus transposition; M, male; N, number of patients.
aSignificance level: P < .05. ± indicates standard deviation.
bχ2 test.
The graft success rate was 92.5% (37 patients) in the entire group. The graft success rates were 94.4% (17 patients) in the GIC group and 90.9% (20 patients) in the IT groups. There was no statistically significant difference between groups in graft success (P = 1.000).
The mean preoperative ABG was 29.40 (8.47) dB, the mean postoperative ABG was 15.25 (8.55) dB in the entire group, and the difference was statistically significant (P < .001). The functional outcome (ABG ≤ 20 dB) was 80% (32 patients) in the entire group. Hearing outcome in groups 1 and 2 were given in Table 2.
Comparisons of Hearing Outcomes and Functional Success Between Groups.a
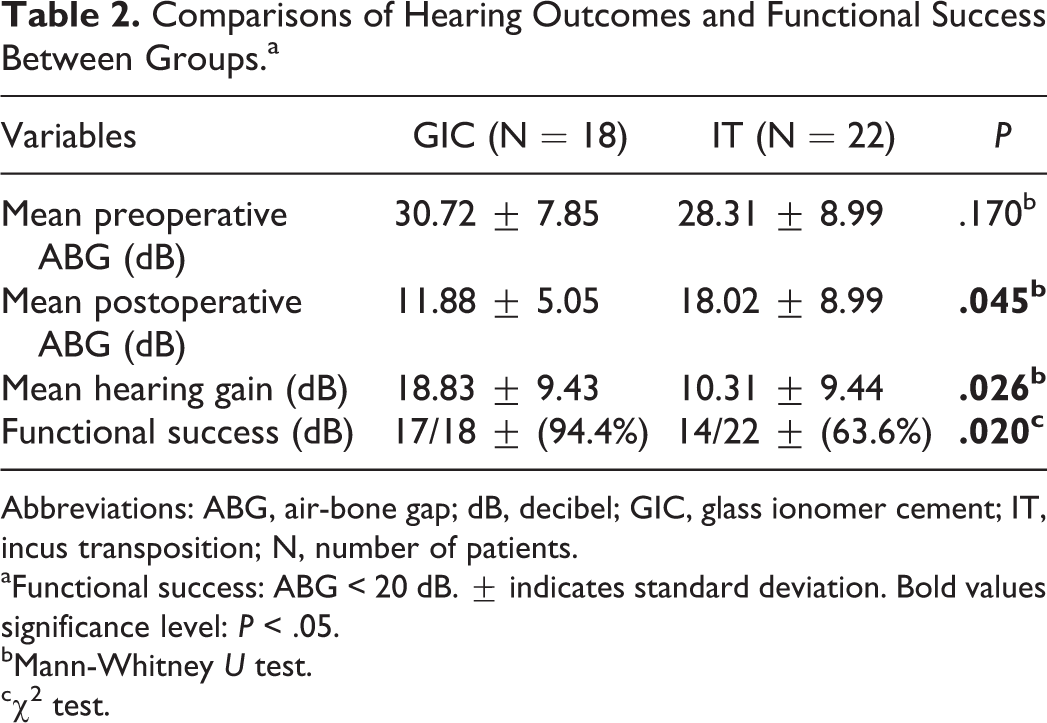
Abbreviations: ABG, air-bone gap; dB, decibel; GIC, glass ionomer cement; IT, incus transposition; N, number of patients.
aFunctional success: ABG < 20 dB. ± indicates standard deviation. Bold values significance level: P < .05.
bMann-Whitney U test.
cχ2 test.
The mean preoperative SRT was 42.10 (12.25) dB, the mean postoperative SRT was 27.32 (14.70) dB in the entire group, and the difference was statistically significant (P < .001). The mean preoperative WRS was 92.30%, the mean postoperative WRS was 93.85% in the entire group, and the difference was not statistically significant (P = .210). The pre- and posttreatment air conduction pure tone average and WRS results for all patients are reported (Figures 1 and 2, respectively).
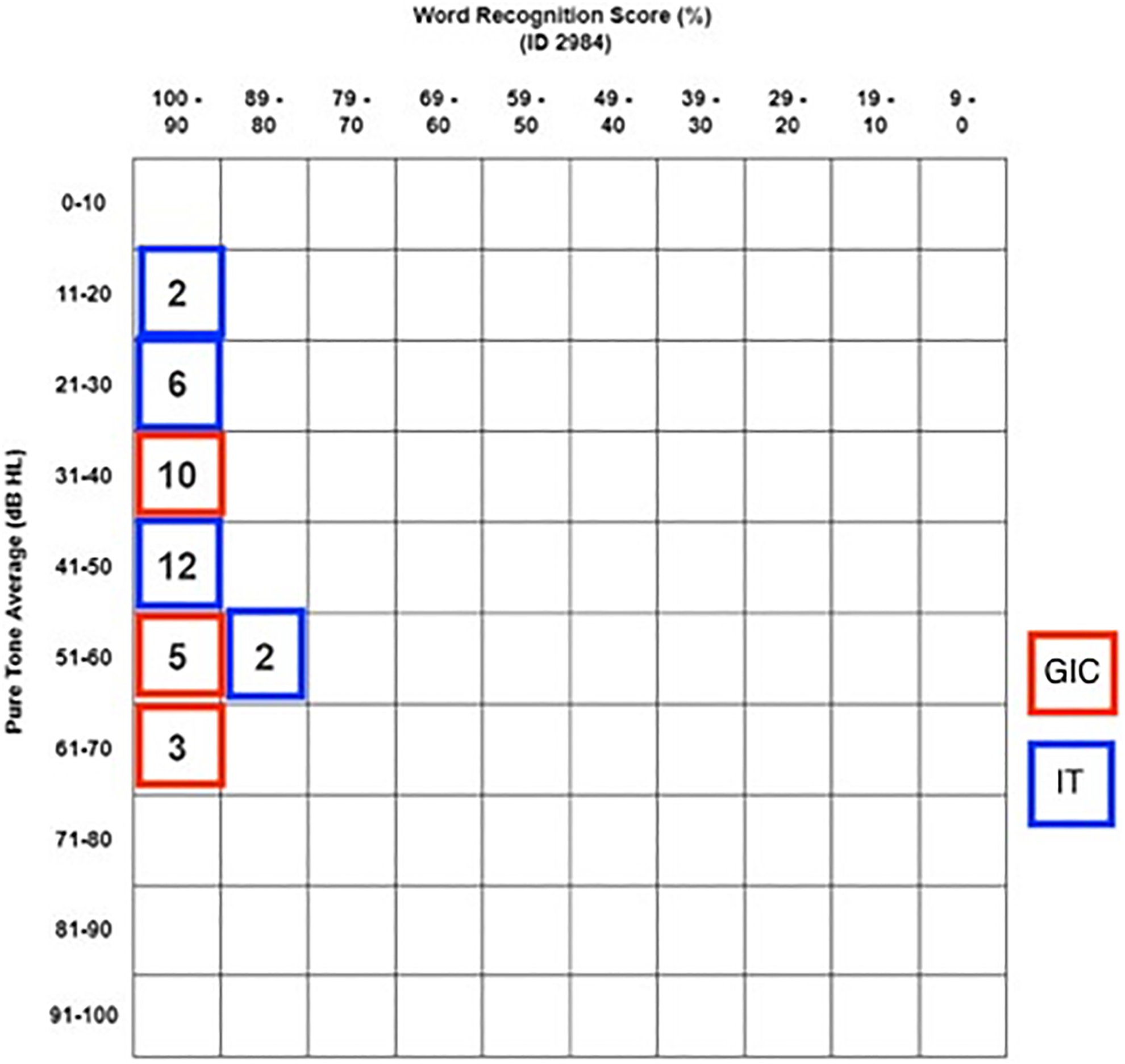
Pretreatment pure tone average and word recognition score scattergram.
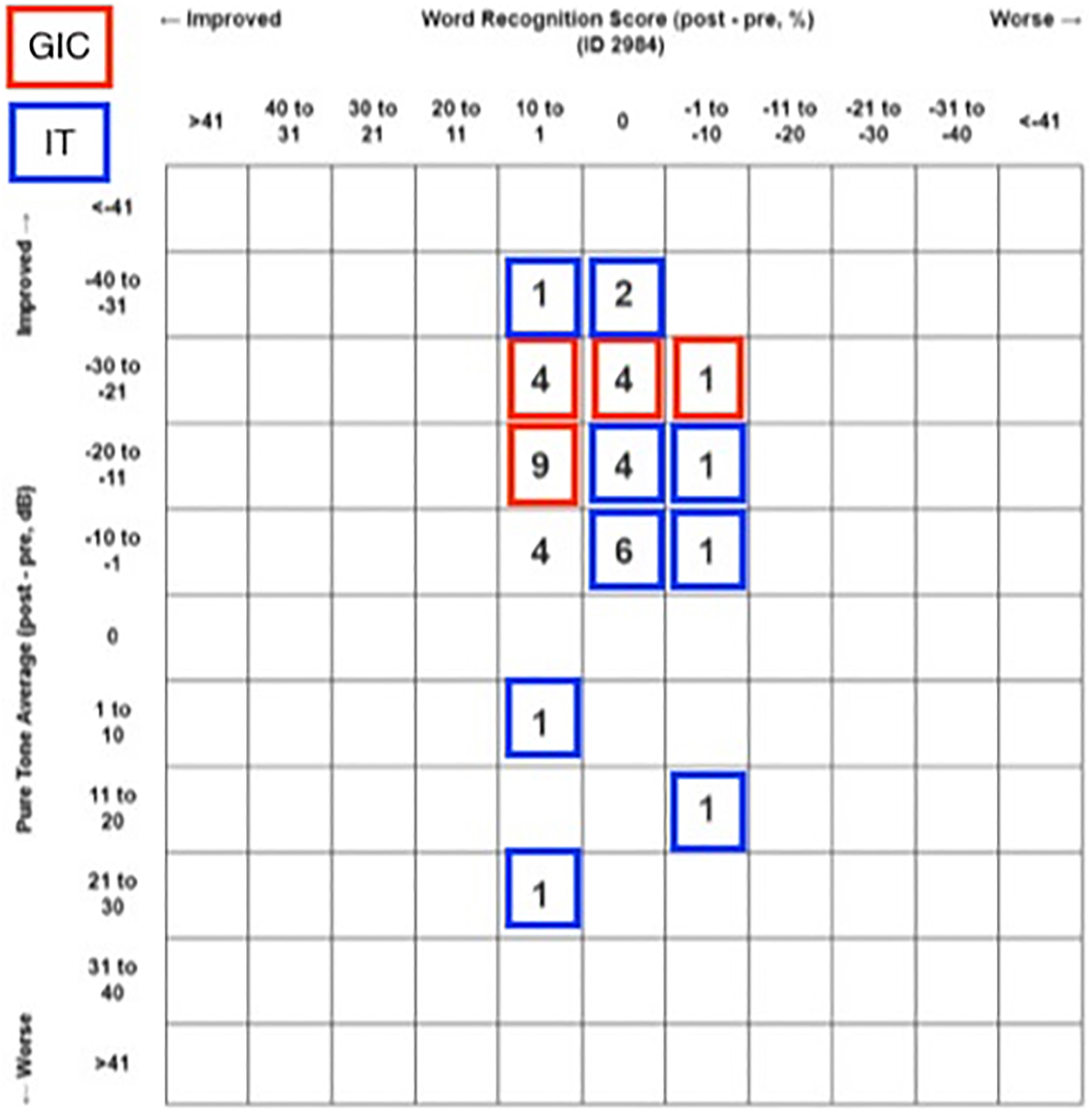
Posttreatment pure tone average and word recognition score scattergram.
In the GIC group, the mean preoperative SRT was 45.22 (12.82) dB, the mean postoperative SRT was 26.05 (14.33) dB, and the difference was statistically significant (P < .001). The mean preoperative WRS was 92%, the mean postoperative WRS was 94.6%, and the difference was not statistically significant (P = .810).
In the IT group, the mean preoperative SRT was 39.54 (11.75) dB, the mean postoperative SRT was 28.36 (15.26) dB, and the difference was statistically significant (P < .001). The mean preoperative WRS was 92.50%, the mean postoperative WRS was 93.10%, and the difference was not statistically significant (P = .174). There were no statistically significant differences between groups in terms of postoperative SRT and WRS (P = .628, P = .260, respectively).
Discussion
Our results showed that the ossicular chain repair with GIC rebridging technique has much greater hearing outcomes than sculpted IT technique. The graft success rates were 94.7% and 90.9% in the GIC group and the IT group, respectively. We did not observe any serious complication associated with the use of GIC. We may state that GIC can be safely and effectively used for ossicular chain reconstruction in pediatric patients with incus long process defects.
The long process of incus is the most susceptible ossicles to both trauma and infections due to the course of its blood supply and anatomical position. 11,12 The authors found that isolated incus defect with an intact malleus and stapes suprastructure was present in 60% to 75% of ossicular defects. 13,14 Since the erosion of incus results in a conductive hearing loss, repair of incus long process defect is a significant consideration of hearing reconstruction in tympanoplasty. Numerous techniques and materials have been shown to be successful for closure of the gap between malleus and stapes, even that there is no consensus in the literature on which technique or material is proper to perform.
Incus long process defects can be repaired by bypassing the defect or rebridging the ossicular gap. Autologous or homologous biografts, synthetic allografts, and biocompatible bone cement are widely used graft materials for the repair of these defects.
Allograft prosthesis is made from biocompatible synthetic material. The most commonly used allograft ossicular replacement prostheses are Teflon, polyethylene, porous plastics, metals (eg, steel, gold, titanium), and ceramics. These materials are ready for use, can be reshaped or trimmed, and do not require drilling but they have higher extrusion and displacement rates than autografts, their cost is relatively high, and there is a risk of ossicular necrosis due to contact with the prosthesis. 15,16 The risk of prosthesis extrusion is found to be significantly high particularly in poor ventilated ears, but the risk can be reduced substantially by the placement of cartilage between the prosthesis and TM. 12
The use of homologous incus graft obtained from human cadavers has been abandoned due to the potential risk of transmission of virus or prion. The most commonly used autograft ossiculoplasty biomaterials are incus remnant, cortical bone, and cartilage. The autologous IT technique was offered as an alternative to type 3 tympanoplasty described by Hall and Rytzner. 3 In this technique, the sculpted incus is placed between the handle of malleus and stapes head. The advantages of autologous incus graft include lower extrusion rate and cost, biocompatibility, and no risk of toxicity or transmitting infections. However, this technique requires the proper drilling and shaping of incus for the stabilization of graft between stapes and malleus. Displacement, necrosis, lysis, or bony adhesion of graft may result with poor hearing levels. In a study conducted on 177 patients who underwent ossiculoplasty with IT, the authors reported that mean postoperative ABG was less than 10 dB in 55% of patients, and less than 20 dB in 85% of patients. 17 O’Reilly et al 16 reported on 137 patients who underwent ossiculoplasty with IT, the mean postoperative ABG was 18.6 dB and 66.4% of patients had an ABG of less than 20 dB. Albu et al 18 performed ossiculoplasty with autologous and alloplastic incus graft and found a mean ABG of 14.5 dB. Sanna et al 4 compared autologous IT versus porous plastic prosthesis with or without cartilage and found a mean postoperative ABG of less than 15 dB in 63.2% of patients with autologous IT, 41.5% of patients with plastic prosthesis with cartilage, and 37.5% of patients with plastic prosthesis without cartilage. Nevoux et al 19 used composite cartilage for the repair of incus defects in their large pediatric series, and they reported a mean hearing gain of 6 dB at postoperative 12 months. In the present study, we performed autologous IT in 22 patients, 63.4% of whom had an ABG of less than 20 dB, and the mean postoperative ABG was 18.02 dB.
Recently, there has been an increasing interest by otologist in bone cement rebridging ossiculoplasty techniques. The use of GIC in ossicular defects preserves the anatomical and physiological nature of ossicular chain conduction system, and these results with more predictable and more satisfying hearing outcomes. Glass ionomer cement is cheap in price compared to ossicular replacement prosthesis or homologous incus, and estimated cost for the amount of bone cement used for ossiculoplasty is less than $1 per patient. It is ready to apply and ready to find, stable, and highly biocompatible. The use of GIC in ossicular defects between incus remnant and stapes is a faster procedure (15 minutes) than any ossiculoplasty technique (30-45 minutes). 15 An exothermic reaction occurs when 2 components (powder and liquid) are mixed for 15 to 30 seconds. However, exothermic heat is produced at the time of mixing the powder and liquid contents of the bone cement. In our experience, we did not encountered heat-related problem in the tissues around the surgical field at the time of application. The mixture starts to get hardened in a few minutes and reaches its maximum stiffness in 7 to 10 minutes. Nonetheless, there are some substantial matters that should be considered during GIC application. The operation field should be dry and bloodless, and any mucosa overlying the ossicles should be removed before the application of GIC. The studies showed that the contact of GIC with wet surface and the low pH levels results with the release of GIC. Since GIC has a potential risk of neurotoxicity, come into contact with the neural structures such as dura, perilymph, oval, and round window and the facial nerve should be avoided. There are several cases that reported the aluminum encephalopathy and death due to contact of aluminum-containing cement with cerebrospinal fluids and neural tissues. 20 Therefore, placement of small pieces of absorbable sponges over the aforementioned susceptible structures may prevent the accidental contact of GIC with these structures. In an experimental animal study, GIC was directly applied on the facial nerve. The authors reported that GIC caused foreign body reaction, increased inflammation, and granulation tissue formation around the nerve, but it did not lead to a permanent facial nerve dysfunction. 21 In case of any contamination of GIC with neural structures, GIC should be suctioned carefully and tympanic cavity should be irrigated with sterile saline. In our study, we did not observe any serious complication associated with GIC.
Brask 22 performed incudostapedial bridging with GIC in 22 patients and reported a postoperative mean ABG of 16 dB and an ABG of less than 20 dB in 81.3% of patients. Bayazit et al 23 used GIC in 46 patients with incus long process defects and achieved successful hearing restoration in 78.6% of patients. Baglam et al 24 performed incudostapedial rebridging ossiculoplasty in 136 patients and reported a postoperative mean ABG of 16.54, with an ABG of less than 20 dB in 81.6% of patients. Ozer et al 25 reported a successful hearing result with incudostapedial rebridging in 60% of patients. Dogan et al 26 used GIC in 15 pediatric patients with incus defects and found a postoperative mean ABG of 13.00 dB and a mean hearing gain of 20.33 dB. In the present study, we achieved a postoperative mean ABG of 11.88 dB, an ABG of less than 20 dB in 94.4% of patients, and a mean hearing gain of 18.83 dB in the GIC group.
In the literature, there are several studies that investigated the hearing results of GIC and IT techniques (Table 3). Dere et al 6 compared GIC and IT in reconstruction of incus long process defects in adults and reported that there was no significant difference between groups regarding postoperative mean ABG gain. Somers et al 15 compared hydroxyapatite bone cement and IT in patients with incudostapedial defect and found that mean hearing gains at postoperative 6 and 12 months were significantly greater in hydroxyapatite group than in IT group. Demir et al 27 compared the hearing outcomes of GIC and IT in type 2 tympanoplasty, and they did not find a significant difference in functional results between groups. Yazıcı et al 8 reported better functional results in patients underwent incudostapedial rebridging with GIC than in those underwent IT. In their study, they did not find a significant difference regarding graft take between groups. Celenk et al 7 compared GIC versus IT and found that the mean hearing gain was significantly greater in the GIC group (19.36 dB) than in the IT group (15.20 dB). They also reported a postoperative mean ABG of less than 20 dB in 78% and 63.2% of patients in the GIC and the IT groups, respectively. In the present study, the functional results were significantly better in the GIC group (94.4%) than in the IT group (63.4%). We also compared the anatomical results (graft success) between groups, and we did not find a significant difference between groups.
Results of GIC and IT Techniques in the Literature Compared With the Present Study.a
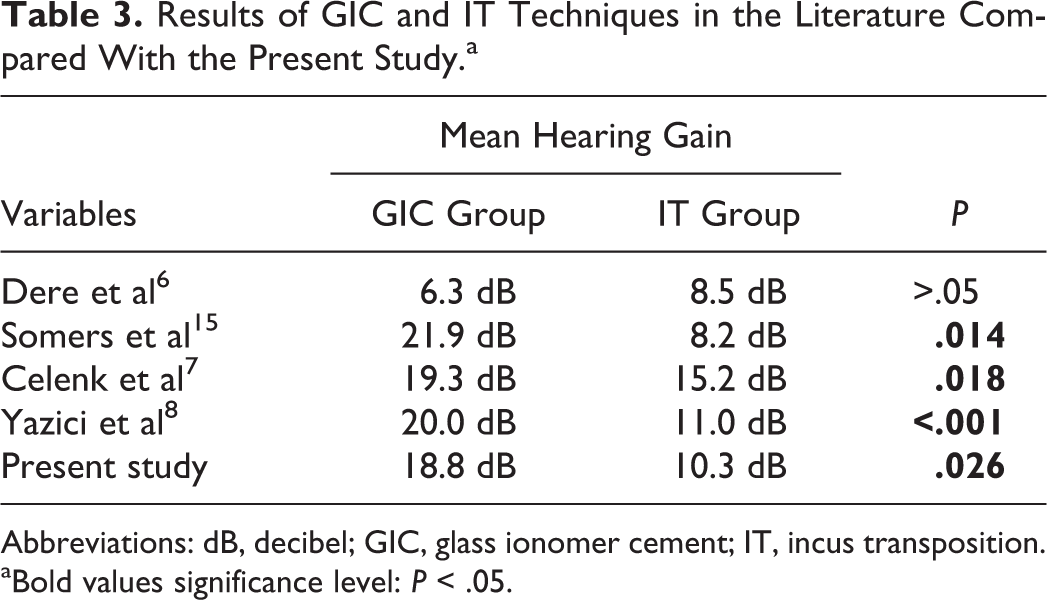
Abbreviations: dB, decibel; GIC, glass ionomer cement; IT, incus transposition.
aBold values significance level: P < .05.
The limitation of our study is the small number of patients. On the other hand, some authors claim that the bone cement will be fractured in the long term and reexploration will be required. Further new studies with larger number of pediatric patients and long-term follow-up are needed to validate these techniques.
In conclusion, reconstruction of small incus long process defects using GIC is a valuable technique and can be safely used in pediatric patients. Glass ionomer cement technique enables the physiological reconstruction of ossicular chain, and the hearing results are significantly better in appropriate patients when compared with a sculpted IT technique.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.