
Abstract
Infectious pseudoaneurysm is a rare condition characterized by arterial wall dilation, usually due to an adjacent infectious focus. We present an 8-year-old male with a 3-day history of progressive, severe headache 2 weeks after treatment for a parapharyngeal abscess. Computed tomography revealed a left internal carotid artery (ICA) pseudoaneurysm inferior to the skull base and a small parapharyngeal abscess inferior to the pseudoaneurysm. The patient was admitted for intravenous antibiotic treatment and underwent transfemoral endovascular coil occlusion of the cervical ICA pseudoaneurysm without complications. We discuss the presentation and management of rare vascular complications of parapharyngeal abscesses involving major arteries of the neck and the role of neurointerventional embolization in these cases.
Keywords
Report
Infectious pseudoaneurysm is a rare condition characterized by arterial wall dilation, usually due to an adjacent infection. 1 Rates of vascular complication due to a neck infection are rare. However, with mortality rates are as high as 77% without and 35% with treatment, these present with substantial potential risk. 2 Carotid pseudoaneurysms are at high risk for rupture. 3 To our knowledge, there are few reports of infectious pseudoaneurysms in children secondary to head and neck infections.1-5
An 8-year-old male presented with a 3-day history of severe left-sided headache, fever, and fatigue. He had left neck fullness and reduced neck mobility; the remainder of the head and neck exam was normal. Two weeks prior, he was hospitalized with a left parapharyngeal abscess. Computerized tomography (CT) scan showed a 1.3-cm parapharyngeal abscess (Figure 1). He improved clinically with 48 hours of intravenous (IV) ampicillin/sulbactam. The child was afebrile during the hospitalization with improved neck motion and decreased trismus. He was discharged with 10 days of oral amoxicillin–clavulanate. A repeat (CT) scan showed a 21 × 20 × 27 mm left internal carotid artery (ICA) pseudoaneurysm inferior to the skull base with a small parapharyngeal abscess inferior to the pseudoaneurysm (Figure 2).
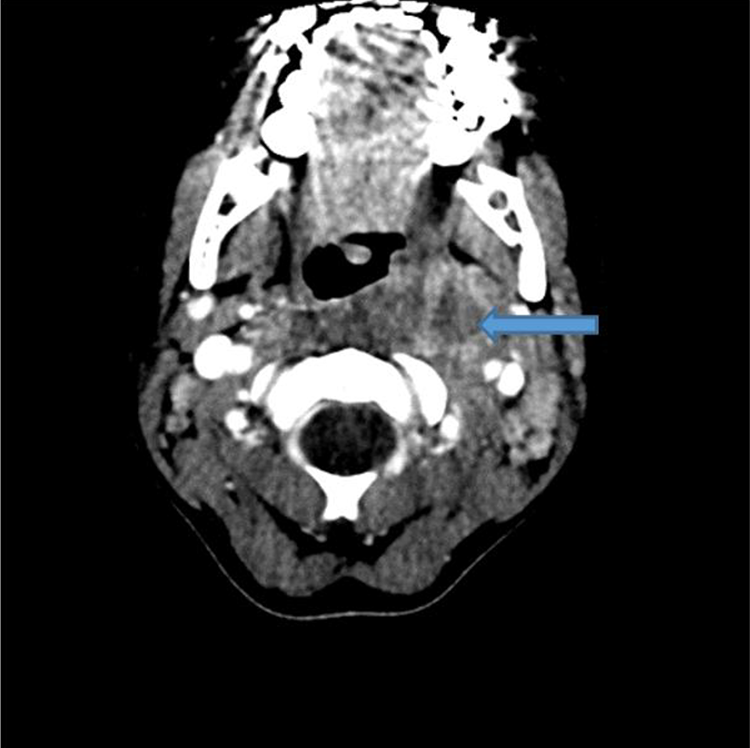
Computed tomography with contrast, axial view of a left parapharyngeal abscess (blue arrow) measured approximately 1.3 cm. This was the initial CT 2 weeks prior to his presentation with the left ICA pseudoaneurysm. CT indicates computed tomography; ICA, internal carotid artery.
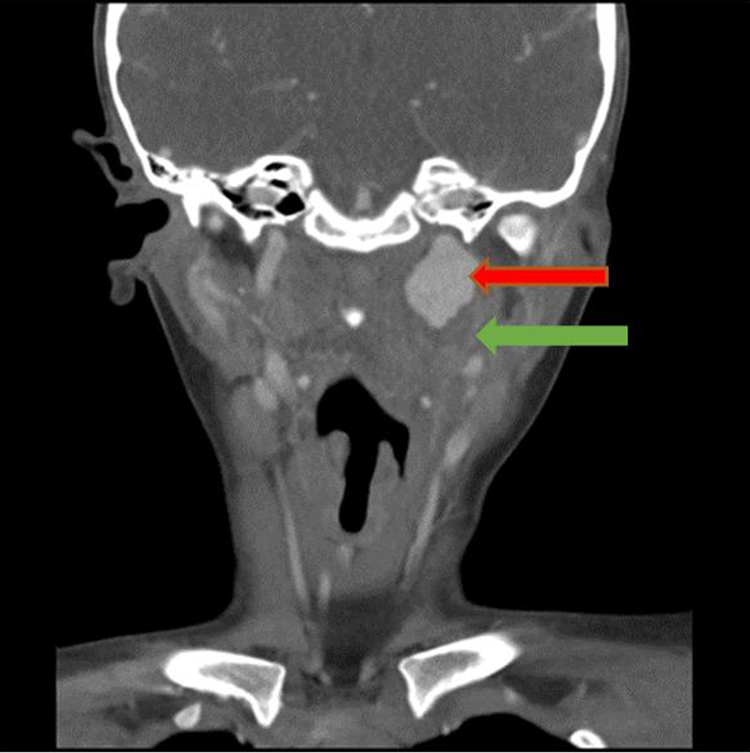
Computed tomography with contrast, coronal view of a large left ICA pseudoaneurysm (red arrow) with a small parapharyngeal space abscess (green arrow) at the inferior aspect of the aneurysm. ICA indicates internal carotid artery.
He was started on IV ceftriaxone and oral clindamycin and hydrocodone/acetaminophen with alternating ketorolac for headaches. Surgical drainage of the abscess was considered too high risk for rupture. The child was started on dual anti-platelet therapy including Plavix and aspirin to prevent clotting. On day 4, he underwent transfemoral cerebral angiography and coil occlusion of the cervical ICA pseudoaneurysm (Figure 3A and 3B). 6 Due to concern of flow through the pseudoaneurysm on follow-up magnetic resonance imaging and arteriogram (MRI/MRA), the patient was taken 2 days later for further coiling of the left ICA. Subsequent ultrasound (US) showed a small amount of flow into the pseudoaneurysm so aspirin was stopped. On repeat US, no appreciable flow was noted and was confirmed on MRI/MRA. Aspirin was restarted to avoid thromboembolism from the occluded stump. Magnetic resonance imaging also showed improvement in the parapharyngeal infection. Blood cultures taken at admission and 4 days later were negative. Antibiotics were changed from clindamycin and ceftriaxone to vancomycin and ampicillin/sulbactam for better coverage of MRSA and pharyngeal flora after an infectious disease consultation and were continued for 5 more weeks. He was discharged 1 week after presentation and was asymptomatic with headaches resolved. Magnetic resonance arteriogram a month later revealed a collapsed pseudoaneurysm sac without recanalization, and aspirin was discontinued.
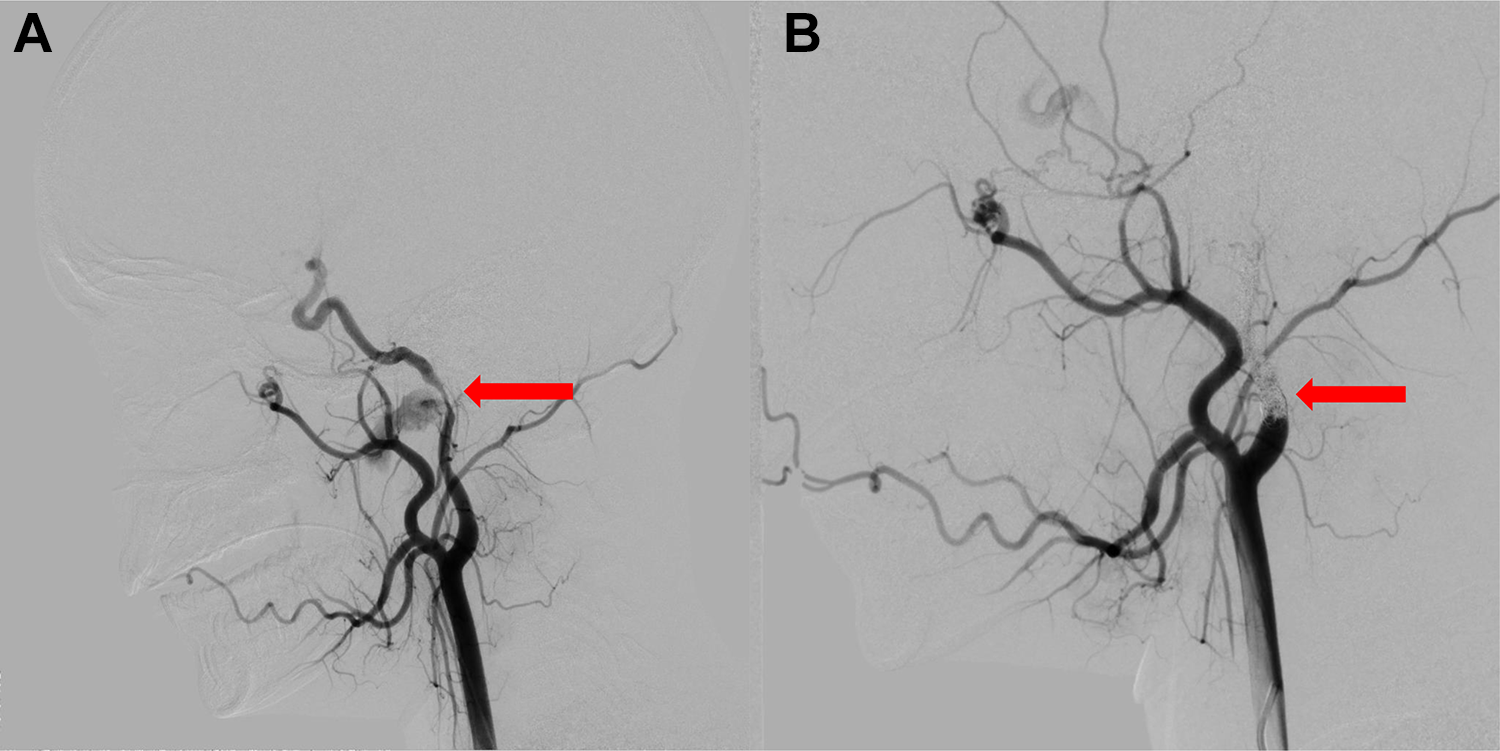
A, Angiogram lateral view shows a giant pseudoaneurysm of the distal cervical segment of the left ICA causing stenosis of the parent vessel in arterial phase (red arrow). B, Angiogram lateral view following embolization showing the coil cast occluding the cervical carotid artery (red arrow). No filling of the giant pseudoaneurysm is visualized. The cavernous carotid is noted to be reconstituted via the artery of the foramen rotundum. ICA indicates internal carotid artery.
Discussion
Complications of deep neck abscesses are rare but can lead to significant morbidity and mortality. Vascular complications should be considered in children with severe headache, bruits, lower cranial nerve palsies, Horner syndrome, and nasal or oropharyngeal bleeding. 7 Diagnosis is challenging and choosing appropriate imaging is an important step in workup. Angiography is the gold standard for diagnosis of pseudoaneurysm; however, this modality is costly and incurs a risk of neurological injury. 8 Computed tomography angiography (CTA) and MRA can replace most invasive angiographic procedures. 9 The choice of the radiological investigation should follow discussions with the neurosurgical and radiological colleagues. 10 Both CTA and MRA have high sensitivities and specificities of 70% to 90%. 11 In this child, a CT of the neck was used for diagnosis, and MRI and MRA to further evaluate the vascular architecture prior to procedural intervention.
Treatment options include observation, stenting, surgical ligation, and embolization. Conservative management is rarely an option,12,13,14; consequences of an untreated pseudoaneurysm include clot propagation, embolization, and hemorrhage. 13
The lack of long-term data surrounding the efficacy and safety of stenting precludes its recommendation by some physicians. 3 While a viable treatment option, best practices for post-stent anticoagulation in pediatric patients still needs formalized investigation. 15 Concerns remain that the introduction of metal coils to an infected area may contribute to persistent infection, although previous literature does not substantiate this theoretical complication. 16 Novel unforeseen complications like carotid-cutaneous fistulae may arise. 17 Robust, specific data on surgical ligation of the ICA for treating pediatric infectious pseudoaneurysms are also lacking. However, it is generally accepted that the complexity and danger of surgical ICA ligation increases significantly with proximity to the skull base. In patients treated with surgical ligation, mortality rates have been reported as greater than 17%. 13 In this case, the pseudoaneurysm was located just inferior to the skull base, precluding surgical ligation due to lack of proximal carotid control.
Neurointerventional embolization has been previously utilized as an effective endovascular treatment modality for infectious pseudoaneurysm of the ICA in children.4,12,18 Risks include thrombosis, late stent stenosis, and perioperative stroke. 19 These complications are rare, but as with stenting, more robust data surrounding embolization and its long-term outcome profile are necessary. Yet compared to surgical ligation, conservative management, and stenting, endovascular therapy has advantages, particularly for small abscesses proximal to large vessels for patients that tolerate balloon test occlusion. 4
This case highlights why vascular complication involving the major arteries of the neck should be considered in the differential diagnosis for patients presenting with new complaints after treatment for neck infections. Timely diagnosis is essential, and CT should be ordered without delay due to the potential for serious morbidity and mortality. Neurointerventional embolization is a growing diagnostic modality that merits consideration for proximal infectious pseudoaneurysms of the ICA. Management of such a complication requires a multidisciplinary team including pediatric neurosurgery, critical care, infectious disease, otolaryngology, and hematology.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.