
Abstract
Air-bone gap (ABG) is an important indicator of hearing status after myringoplasty. A number of factors have been associated with ABG, but some patients still have ABG without identifiable cause. This study aimed to evaluate the relationship between tympanic membrane (TM) vibration using laser Doppler vibrometry (LDV) and ABG after myringoplasty. Between January 2013 and January 2015, 24 patients with ABG of unknown cause after myringoplasty were enrolled at the Beijing Tongren Hospital. Thirty normal controls were recruited from the hospital staff. All patients underwent primary overlay myringoplasty. Pre- and postoperative air conduction (AC) and bone-conduction (BC) thresholds, and ABG were measured. Umbo velocity transfer function (UVTF) for vibration of TM was measured with LDV. Air conduction thresholds were significantly reduced after myringoplasty (all P < .05), while BC thresholds were not significantly changed (all P > .05). ABG was significantly reduced after myringoplasty (all P < .05). Air-bone gap was correlated with UVTF at 1.0 kHz (r = −0.46; P = .024). For patients with UVTF >0.08 mm/s/Pa, ABG was correlated with UVTF (r = −0.56; P = .029). For post-myringoplasty ABG without readily observable causes, there was a significant relationship between ABG and TM vibration. These results provide new insights in the understanding of this relationship and may help explain ABG after myringoplasty when there are no clear contributing factors.
Introduction
Myringoplasty is a surgical procedure used to repair perforation of the tympanic membrane (TM) using autologous materials such as temporalis fascia. It is one of the most common surgeries for chronic otitis media (COM), which is characterized by perforation of the TM combined with some degree of conductive hearing loss, as revealed by air-bone gap (ABG) in conduction using audiometry. Evidence suggests good outcomes for the procedure, with 9.6 to 15.0 dB of improvement in hearing thresholds for approximately 90% of patients. 1 -3
Air-bone gap is an important indicator of hearing status after tympanoplasty. Ribeiro et al 4 reported postoperative improvements in ABG for approximately 75% of patients. Saumil et al 5 showed that postoperative ABG was <10 dB in 51% of cases and <20 dB in 96% of cases. Nevertheless, other studies have reported smaller postoperative improvements in ABG. Pfammatter et al 3 reported that postoperative improvements in ABG were found in only 20% of cases, with an average residual ABG of 8 dB. Various factors may affect audiometric outcomes after myringoplasty, including the situation of the mucosa in the middle ear cavity, atelectasis of the middle ear, malfunction of the Eustachian tube, ossicular discontinuity, inflammation in the middle ear cavity and/or in the mastoid, the volume of the middle ear cavity, blunting of the tympanomeatal angle, lateralization of the reconstructed TM, tension of the reconstructed TM, fibrosis of the mucosa, tympanosclerosis, ossicular chain ankylosis, and the experience of the surgeon. 1,6
In some cases, there are no clear causes of postoperative ABG. The vibration of the TM is pivotal for transmitting sound via the ossicles to the stapes footplate. Because the displacement of the TM at the umbo is <1 µm at 120 dB sound pressure level, 7 and because the resolution of microscopes used in clinical surgery is >100 µm, it is impossible for surgeons to directly observe the vibration of the TM during or after myringoplasty. Laser Doppler vibrometry (LDV) has been used in otolaryngology to measure TM vibration in the nanometer range and can be used to distinguish some causes of tympanoplastic failure. 8 Laser Doppler vibrometry can be used to measure umbo velocity transfer function (UVTF). A UVTF study by Röösli et al 9 showed that inertia of the ossicles and cochlear fluid drive bone-conducted (BC) hearing <500 Hz but that sound radiating into the external hear canal contribute to BC hearing >3000 Hz. Reduced UVTF may indicate TM dysfunction, which may in turn relate to persistent ABG after myringoplasty.
The purpose of this study was to investigate the relationship between the vibration of the TM (using LDV) and ABG in patients with COM after myringoplasty. Better understanding of this relationship may help explain ABG after myringoplasty when there are no clear contributing factors.
Materials and Methods
Patients
Between January 2013 and January 2015, patients undergoing type I myringoplasty were admitted to the Beijing Tongren Hospital, Beijing, China. The inclusion criteria were (1) 18 to 60 years of age; (2) no otorrhea within 3 months before operation; (3) preoperative central tympanic large perforation, and postoperative complete TM with good mobility but no acute or chronic inflammation; (4) mobile ossicular chain without further middle ear pathology; and (5) postoperative hearing tests indicated conductive deafness with postoperative ABG ≤30 dB hearing level (HL) but with no obvious clinical causes (eg, poor Eustachian tube function, tympanomeatal angle blunting, lateralization of the reconstructed TM, infection in middle ear cavity and mastoid, atelectasis, tympanosclerosis, ossicular chain ankylosis, or middle ear adhesions). The exclusion criteria were (1) BC threshold >25 dB HL (500, 1000, 2000, 4000 Hz) in pure-tone audiometry; (2) history of previous ear surgery; (3) one year after myringoplasty, the temporal bone computed tomography (CT) showed middle ear mastoid cavity with soft tissue shadow; (4) long-term COM and external otitis; or (5) history of upper respiratory tract infection in recent months.
Data previously collected in normal hearing (NH) participants (n = 30) were used as control data for LDV measurements. 10 Normal hearing participants were recruited from the staff and medical students in our hospital and had no otopathy or systemic disease, no long history of noise exposure, and no acute or chronic upper respiratory inflammation. Air conduction (AC) thresholds were >25 dB HL across all audiometric test frequencies with no ABG. They all were with normal TM and Eustachian tube ranges at the time of their participation.
Ethical approval was obtained from the institutional review board of Beijing Tongren Hospital, Capital Medical University (No. 2014-0907). Informed consent was obtained from all patients.
Routine Audiological Examinations
Routine audiological examination consisted of otoscopy, followed by pure-tone audiometry in which AC thresholds were measured for both ears at 0.5, 1.0, 2.0, and 4.0 kHz. Bone-conduction thresholds were measured at 0.5, 1.0, 2.0, and 4.0 kHz in a soundproof booth. Air-bone gap was calculated at 0.5, 1.0, 2.0, and 4.0 kHz, and ABG ≥10 dB was considered as conductive deafness.
Measurement of TM Vibration
The stimulus and measurement system is illustrated in Figure 1. During measurement, the patient laid supine on an examination bed with the ear to be measured facing toward the otology microscope. Head brace was used to fix the forehead and occipital, and the fixable otoscope was implanted into the external auditory canal. The otologist positioned the laser beam from the LDV equipment (Polytec CLV-2534) through an ear speculum on the apex of the umbo. The ear speculum was paired with a sound coupler, through which a soft silicone probe was placed within 5 mm of the TM. The sound coupler also tightly sealed the ear canal. Pure tones at 0.5, 1.0, 2.0, and 4.0 kHz were generated at 90 dB sound pressure level (SPL) using a signal generator (Agilent Technologies). During the measurements, stimuli were continuously monitored and recorded using a probe microphone (ER7; Etymotic) placed in the external auditory canal near the TM. A site at the apex of the light reflex of the TM (close to the umbo) was chosen as the measurement location based on recordings in normal ears. Because the light reflex of the TM disappears after myringoplasty, measurements were made at the same site using light reflex microbeads, which weighed <0.05 mg. Since lying supine with head brace does not guarantee a completely stable TM, measurements were taken until at least 3 similar measurements were obtained.
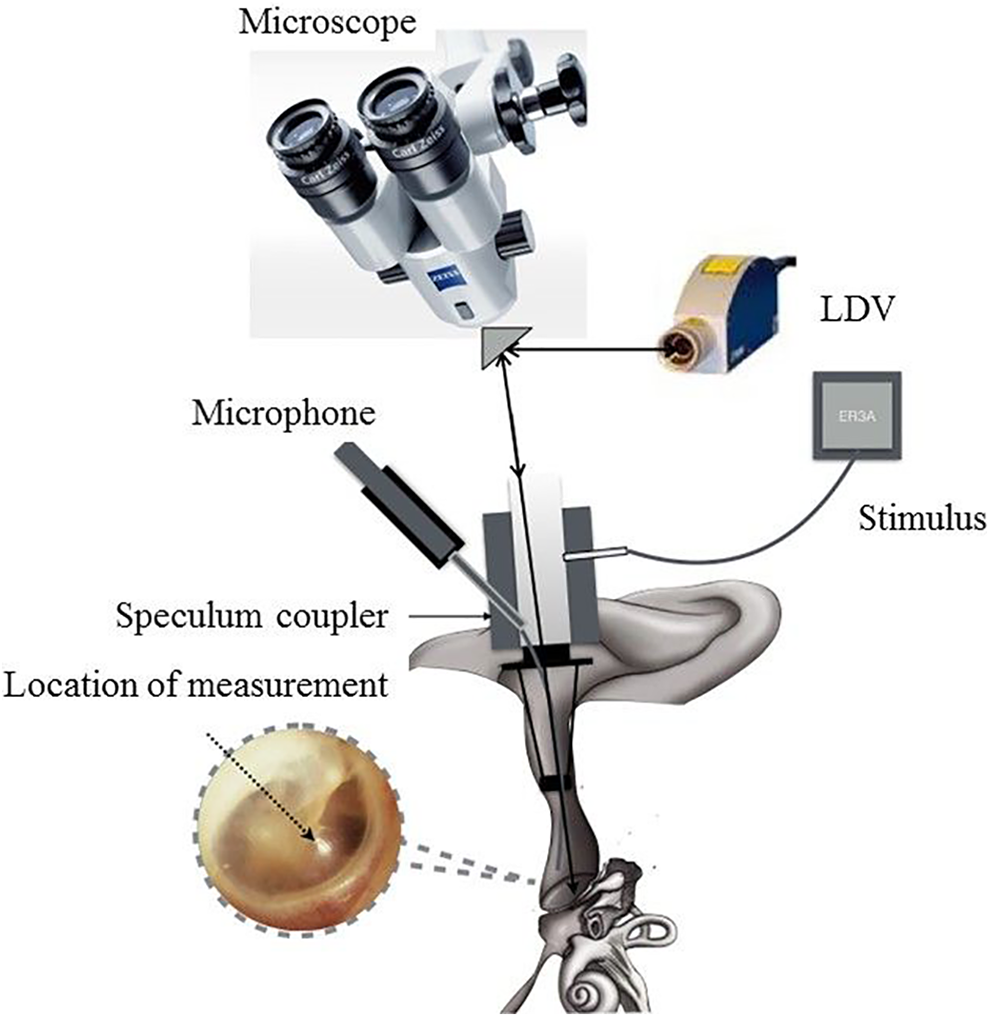
Schematic of the laser Doppler vibrometry (LDV) equipment used to measure vibration velocity in vivo human ears.
Data were presented in terms of the UVTF, which was calculated as the ratio between the measured velocity magnitude and the measured SPL. 11 Data were recorded only when the signal-to-noise ratio was >10 dB. Phase angle data were not recorded in this study.
Surgical Technique
The myringoplasty procedures were all performed by the same experienced senior otologist (author Y.L.) using overlay techniques. 12 In all cases, a retroauricular approach with limited canalplasty was used, and the temporalis fascia was used as graft material. A complete exploration of the tympanic cavity was performed.
Follow-Up
Pure-tone audiometry was reviewed to measure AC thresholds and BC thresholds, and to calculate ABG 12 months after myringoplasty. The temporal bone CT and UVTF were examined in the meantime.
Statistical Analysis
Repeated measures analyses of variance (RM ANOVAs) with post hoc Tukey pairwise comparisons were used to examine the effects of test frequency and/or measurement time for audiometric and UVTF measures. To compare across hearing impairment (HI) and NH groups, 1-way ANOVAs were performed. Pearson correlations and linear regression analyses were performed to describe the relationship between ABG and UVTF. Statistics were performed using SigmaStat 13.0 (Systat Software). In all statistical analyses, P < .05 was considered to be statistically significant.
Results
Characteristics of the Participants
A total of 150 patients were admitted during the study period. Of these, 24 patients (10 male, 14 female) met all criteria and were enrolled in this study (mean age: 39.1 ± 11.8 years). The remaining 126 patients included cases with no ABG, cases with Eustachian tube dysfunction, scar formation in middle ear cavity, and lateralization of the reconstructed TM, all of them were beyond the scope of this study. Myringoplasty was performed in 11 left ears and 13 right ears. All patients had a dry ear without infection for at least 3 months before the operation (mean dry ear duration: 11.7 ± 7.7 months). The mean follow-up time was 22.1 ± 6.9 months. Thirty NH participants (30 ears; 13 male, 17 female) were enrolled (mean age: 30.1 ± 8 years) as a control group; 15 were examined in the left ear and 15 in the right ear.
Figure 1 shows the mean AC thresholds (left panel), BC thresholds (middle panel), and ABG (right panel) before and after myringoplasty. A 2-way RM ANOVA was performed on the AC threshold data, with test frequency (0.5, 1.0, 2.0, and 4.0 kHz) and measurement time (before, after myringoplasty) as within-subject factors. Results showed significant effects for test frequency (F3,69 = 9.5, P < .001) and measurement time (F1,69 = 18.4, P < .001); there was a significant interaction (F3,69 = 3.7, P = .015). Post hoc Tukey pairwise comparisons showed that thresholds were significantly lower for 2 kHz than for 0.5 or 4.0 kHz before myringoplasty (P < .05 in both cases); there were no significant differences in thresholds among the remaining frequencies (P > .05 in all cases). After myringoplasty, thresholds were significantly lower for 0.5, 1.0, and 2.0 kHz, relative to 4.0 kHz (P < .05 in all cases); there were no significant differences in thresholds among the remaining frequencies (P > .05 in all cases). For all test frequencies, thresholds were significantly lower after myringoplasty (P < .05 in all cases).
A 2-way RM ANOVA was performed on the BC threshold data, with test frequency and measurement time as factors. Results showed a significant effect for test frequency (F3,69 = 7.6, P < .001) but not for measurement time (F1,69 = 3.0, P = .096); there was no significant interaction (F3,69 = 1.5, P = .224). Post hoc Tukey pairwise comparisons showed that thresholds were significantly lower for 1.0 kHz relative to 2.0 or 4.0 kHz and significantly lower for 0.5 kHz relative to 2.0 kHz (P < .05 in all cases); there were no significant differences in thresholds among the remaining frequencies (P > .05 in all cases).
A 2-way RM ANOVA was performed on the ABG data, with test frequency and measurement time as factors. Results showed a significant effect for test frequency (F3,69 = 9.9, P < .001) and measurement time (F1,69 = 29.7, P < .001); there was no significant interaction (F3,69 = 1.7, P = .181). Post hoc Tukey pairwise comparisons showed that ABG was significantly lower for 2.0 kHz relative to 0.5 or 4.0 kHz, before myringoplasty (P < .05 in both cases) and significantly lower for 2.0 kHz relative 4.0 kHz after myringoplasty (P < .05). There were no significant differences in ABG among the remaining frequencies before or after myringoplasty (P > .05 in all cases).
Figure 2 shows the percentage of cases with ABG ≤10, >10 and ≤20, and >20 dB before (left panel) and after myringoplasty (right panel), as a function of test frequency (and averaged across test frequencies). Before myringoplasty, ABG was ≤10 dB for only 8.3% of patients; after myringoplasty, ABG was ≤10 dB for 46.0% of patients. Before myringoplasty, ABG was >10 and ≤20 dB for 16.0% of patients; after myringoplasty, ABG was ≤10 dB for 28.3% of patients. Before myringoplasty, ABG was >20 dB for 76.3% of patients; after myringoplasty, ABG was ≤10 dB for 26.0% of patients.
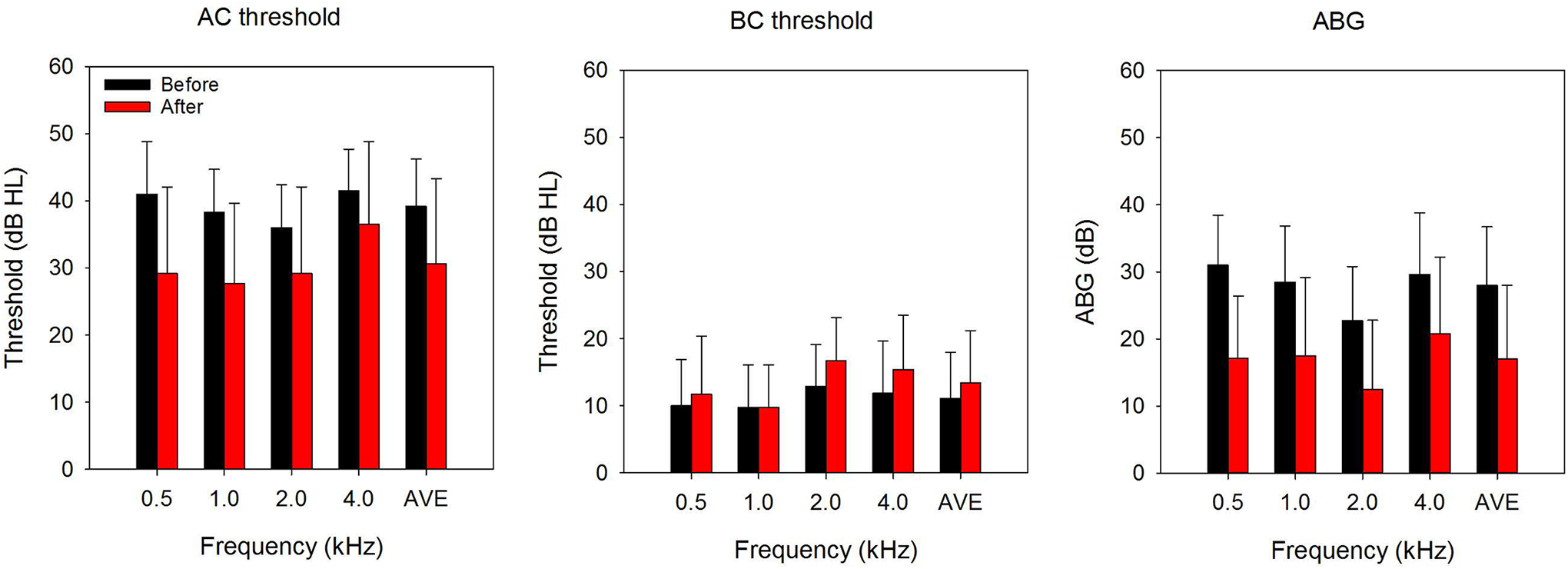
Left: mean air conduction (AC) thresholds before and after myringoplasty, as a function of test frequency. Middle: mean BC thresholds before and after myringoplasty, as a function of test frequency. Middle: mean air-bone gap (ABG) before and after myringoplasty, as a function of test frequency. The error bars show the standard deviation.
Figure 3 shows UVTF values for HI patients with ABG ≤10 dB (black bars), >10 and ≤20 dB (red bars), and >20 dB (green bars); data are also shown for all HI patients (gray bars) and for control NH patients (yellow bars). One-way ANOVAs were performed on the data for each frequency, with subject group (ABG ≤10 dB, ABG >10 and ≤20 dB, ABG >20 dB, NH) as the factor. For 0.5 kHz, there was a significant effect of subject group (F3,50 = 3.0, P = .040). Post hoc Tukey pairwise comparisons showed that UVTF values were significantly higher for ABG ≤10 dB than for ABG >20 dB (P < .05); there were no significant differences among the remaining subject groups. For 1.0 kHz, there was a significant effect of subject group (F3,50 = 8.8, P < .001). Post hoc Tukey pairwise comparisons showed that UVTF values were significantly higher for ABG ≤10 dB than for ABG >10 and ≤20 dB or ABG >20 dB (P < .05 in both cases); there were no significant differences among the remaining subject groups. For 2.0 kHz, there was a significant effect of subject group (F3,50 = 2.9, P = .047); However, post hoc Tukey pairwise comparisons showed no significant differences among subject groups. For 4.0 kHz, there was a significant effect of subject group (F3,50 = 12.3, P < .001). Post hoc Tukey pairwise comparisons showed that UVTF values were significantly higher for NH than for ABG >10 and ≤20 dB or ABG >20 dB and significantly higher for ABG ≤10 dB than for ABG >20 dB (P < .05 in all cases); there were no significant differences among the remaining subject groups. When data were averaged across all frequencies, results showed a significant effect of subject group (F3,50 = 4.7, P = .006). Post hoc Tukey pairwise comparisons showed that UVTF values were significantly higher for NH and ABG ≤10 dB than for ABG >20 dB (P < .05 in both cases); there were no significant differences among the remaining subject groups. When data were averaged across all frequencies and HI data were collapsed across ABG groups, results showed no significant difference between HI and NH patients (F1,52 = 2.1, P = .150).
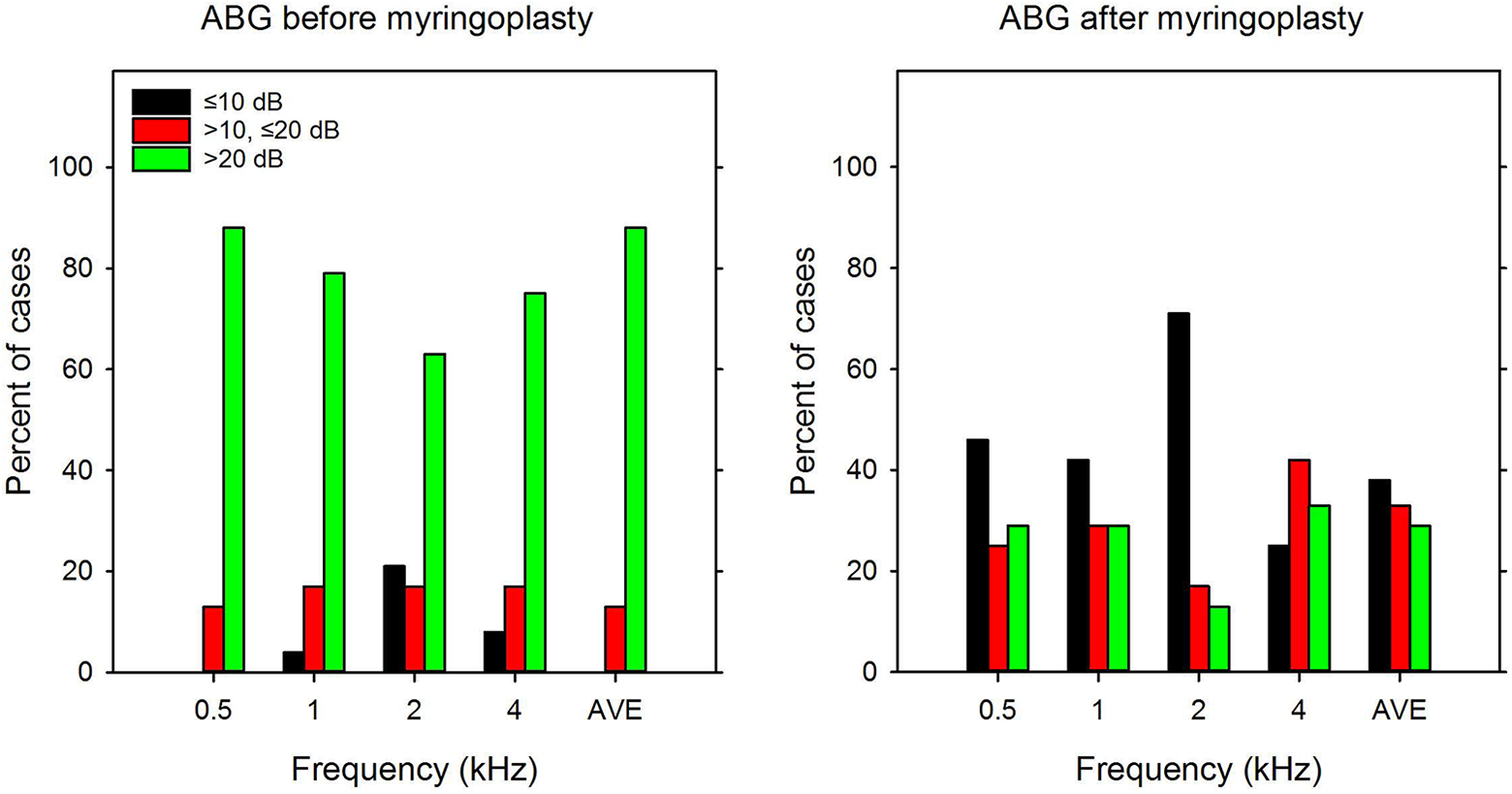
Left: percent of cases with air-bone gap (ABG) ≤10 dB (black bars), >10 and ≤20 dB (red bars), and >20 dB (green bars) before myringoplasty, as a function of test frequency; average data across all test frequencies are shown at the right of the panel. Right: same as left panel, but for data after myringoplasty. The error bars show the standard deviation.
Pearson correlations were used to compare ABG to UVTF values after myringoplasty for the different test frequencies. A significant correlation was observed only for 1.0 kHz (r = −0.46; P = .024); there were no significant correlations for the remaining test frequencies (P > .05 in all cases). Across all test frequencies, a significant correlation was observed between mean ABG and mean UVTF values (r = −0.53; P = .008). For the 13 participants who exhibited mean UVTF values >0.08 mm/s/Pa, a significant correlation was observed between mean ABG and mean UVTF values (r = −0.56; P = .029); there were no significant correlation between mean ABG and mean UVTF values for patients with mean UVTF values ≤0.02 or >0.02 and ≤0.08 mm/s/Pa (P > .05 in both cases). Across all test frequencies, no significant correlation was observed between mean ABG closure (the difference in ABG before and after myringoplasty) and mean UVTF values (r = 0.14; P = .190). (Figure 4).
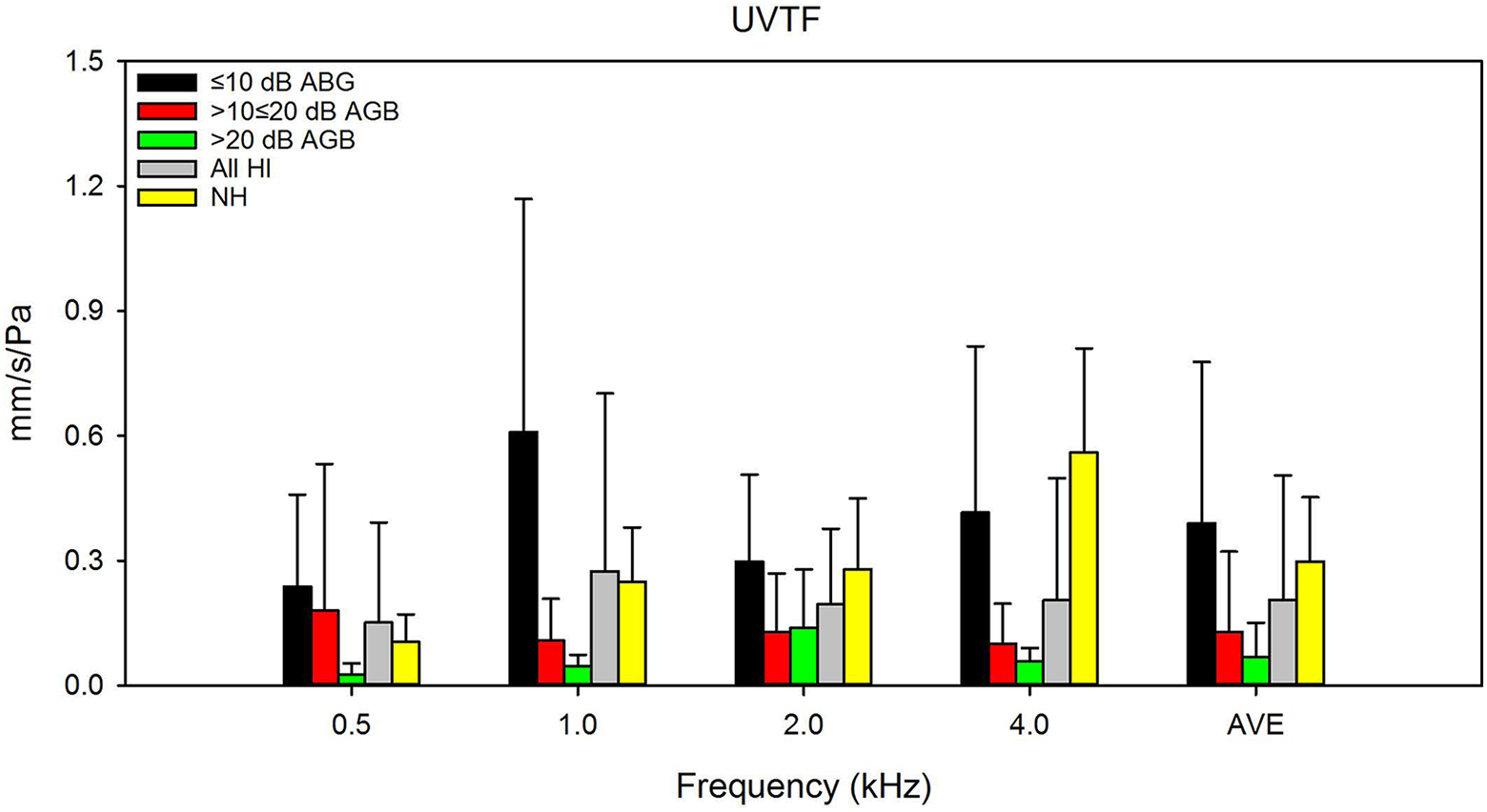
Mean umbo velocity transfer function (UVTF) values after myringoplasty for HI patients with air-bone gap (ABG) ≤10 dB (black bars), >10 and ≤20 dB (red bars), and >20 dB (green bars); the gray bars show mean HI data across all ABG groups, and the yellow bars show mean normal hearing (NH) control data. 10 Average data across all test frequencies are shown at the right of the panel. The error bars show the standard deviation.
Discussion
Air-bone gap is an important indicator of hearing status after myringoplasty. A number of factors have been associated with ABG, but some patients still have ABG without identifiable cause. Therefore, this study aimed to evaluate the relationship between TM vibration (using LDV) and ABG after myringoplasty.
Among these 24 patients and across all test frequencies, the percent of cases with ABG ≤10 dB increased from 0.0% to 38.0% after myringoplasty, and the percent of cases with ABG >20 dB was reduced from 88% to 29% after myringoplasty. There was a significant effect of test frequency, with 2.0 kHz producing the lowest ABG before or after myringoplasty. The greatest reduction in ABG after myringoplasty was observed at 0.5 kHz (14.1 dB).
A significant relationship between ABG and UVTF values at 1 kHz and averaged across all test frequencies. After surgery, ABG was >10 dB and UVTF was >0.02 mm/s/Pa in the majority of patients. For patients with UVTF values >0.08 mm/s/Pa, there was also a significant correlation between mean ABG and UFVT across all test frequencies. Thus, after primary myringoplasty with evident ABG but no readily observable causes, there was a significant relationship between ABG and TM vibration. These results provide new insights in the understanding of this relationship and may help explain ABG after myringoplasty when there are no clear contributing factors.
When averaged across all test frequencies and ABG groups, there was no significant difference in UVTF values between the present HI patients and NH patients from Wang et al. 10 However, when the ABG groups and test frequencies were considered, there was an inconsistent relationship between ABG and UVTF. For example, at 0.5 kHz, there was no significant difference among NH patients and HI patients for any of the ABG groups. At 1 kHz, HI patients with ABG ≤10 dB exhibited significantly higher UVTF values than did NH patients. At 4.0 kHz, NH UVTF values were significantly higher than HI values for any of the ABG groups. Across all test frequencies, NH UVTF values seemed most comparable to those from HI patients with ≤10 dB, which would be expected. The large effect of ABG group for UVTF values at 4.0 kHz suggests that this might be a worthwhile frequency with which to differentiate TM vibration among HI patients after myringoplasty.
It is unclear exactly how the microstructure of the TM affects sound transmission in the middle ear. During clinical examination, calcified plaques and local thinning have been observed in the TM even in patients with NH. 13 Patients with a history of tympanostomy tube or of middle ear inflammation and later healing of the TM show different degrees of conductive hearing loss. 14 In this study, 24 ears showed evident ABG with no readily observable factors on postsurgical examination. The anatomic and acoustic properties of the reconstructed TM may be important factors that influence the vibration of the TM itself and may underlie ABG after myringoplasty in cases where there are no easily observed factors.
Anatomically, the arrangement of collagen fibers of the reconstructed TM is altered after surgery. The human TM is a multilayer fiber structure consisting of distinct layers (outer epidermal, fiber, and mucosal epithelial layers), varying in density, thickness, composition, and arrangement in different regions. The fiber layer determines the tension of the TM. The collagen fibers of the TM have both a radial and circular arrangement. These 2 types of fibers contribute to the mechanical stiffness of the TM. 15 In guinea pigs, a fascia graft showed almost the same structure as the original fibrous layer of the TM, 16 but the arrangement of fibers in reconstructed TM was irregular. 17 The radial collagen fibers in the TM play an important role in the conduction of sound above 4 kHz. 18 Compared with NH data, post-myringoplasty data showed that the UVTF magnitude was decreased at 4.0 kHz. Even for large perforations, Röösli et al 9 reported that hearing returns almost completely across the frequency range except above 4 kHz. Sound energy is transferred from the eardrum via the ossicular chain to the stapes floor. Any change in mass, stiffness, and/or friction in the TM may impact the efficiency of transduction. Therefore, since the collagen fibers in the graft are not arranged in the same manner as in a native TM, it could be hypothesized that this factor affects hearing at specific frequencies. Unfortunately, no technology is yet available to determine collagen fibers arrangement in vivo.
In terms of the quality of the eardrum, thickness plays a vital role for TM vibration and affects TM stiffness. 19 Recently, thickness measurements on human TM using confocal microscopy showed a distribution between 115 and 145 μm, with increments of 2.5 μm. 20 The thickness of the reconstructed TM was distributed evenly; with each increment of TM thickness, the vibration of the TM decreased. 21 A previous study by our group showed that the thickness of the temporal muscle fascia reconstruction affects the TM itself and the vibration of the stapes floor. 22 Lee et al 23 found obvious effects on middle ear sound transmission when the TM thickness was >0.1 mm. The temporal muscle fascia is the most commonly used material in type I myringoplasty. The elastic fibers of the tensor fascia are dense and parallel and are similar in structure to the fibers in the TM; the continuous distribution may benefit the healing process due to better dimensional stability. 24 Nevertheless, the acoustic properties of the reconstructed TM are complex; the dampening effect associated with the added mass and stiffness of the graft may cause significant hearing loss, depending on the size and location of the graft material. 25 In this study, mean ABG and mean UVTF after myringoplasty were significantly correlated. To the extent that thickness of the reconstructed TM limits vibration, the present data suggest potential differences among patients in terms of TM thickness, but additional studies are necessary to confirm this relationship, especially by measuring the exact thickness of the TM, which was not done in the present study.
Previous studies reported important differences among patients in terms of thickness and contractility of autologous temporalis fascia. 24 The loose, crisscrossed elastic fibers in temporalis fascia, combined with scar tissue, might affect the healing and subsequent stability of the TM. 26 For myringoplasty, it is unknown whether interactions between the implant and the remnants of the TM may cause acoustic attenuation, negatively impacting patient hearing.
The TM and the manubrium (handle) of the malleus are connected by a soft tissue structure (tympano-mallear connection or TMC). The manubrium has a specific angle in the anatomical structure, especially in the umbilical plexus of the TM. Poor coupling in the TMC may affect the healing process, which may in turn affect the postoperative morphology of the TM. Voss et al 27 found that the TMC does not affect the middle ear acoustic transmission, but pointed out that further experiments are needed to determine the importance of structural and mechanical features for the function of TM microstructure. Some authors used the finite element model to study middle ear structure and found that links between the manubrium and TM create a cone that provides more efficient transmission of high-frequency sounds. 15 In addition, the tension of the reconstructed TM is an important factor that affects the vibration of the TM. Changes in the TMC have been shown to reduce the effective transmission of sound energy to the ossicles by <5 dB for in vitro models. 27 De Greef et al 28 argued that the TMC is one of the important microstructures that affects sound transmission and overall mechanical system structure. For the present patients with large ABG and small UVTF values, the change in thickness together with the connection of the reconstructed TM may have reduced tension, which in turn reduced the vibration of TM at umbo. In addition, the middle ear mucosa and pneumatization of the temporal bone have been shown to have no significant effect on postoperative middle ear transfer function. 29 Given the difference in sound transmission loss between in vitro and in vivo models, the effects of ossicular coupling between the TM and manubrium should be explored further.
There are some limitations to the study. It is possible that larger perforation of the TM may have contributed to the ABG after myringoplasty. Pfammatter et al 3 reported a significant linear correlation between the preoperative size of TM perforation and the postoperative ABG; however, 20% of these patients had complete ABG closure after myringoplasty. In addition to the size of the perforation, the materials used to reconstruct the TM affect the vibration characteristics. Although the structures of the temporal fascia and TM have some similarities, the fascia underwent healing process after myringoplasty, resulting in different thickness of the TM and unstable characteristics of the TM. TMC is important to maintain the morphology of TM, and its sound transmission properties need to be further studied. The sample size was relatively small; we will further improve the study design, expand the sample size, and combine with the finite element model and temporal bone study to further explore the vibration characteristics of the TM. While UVTF values from the present HI patients were compared to those from NH patients from Wang et al, 10 it might be useful to compare to UVFT values collected in the myringoplasty patients who were excluded from this study (as the cause of ABG was known).
In this study, an overlay technique was used (as opposed to an undelay technique), partly due to the large perforation of the TM in the patient group. Another reason for using the overlay technique was that the gelatin sponge used in underlay technique may not be completely absorbed; such incomplete absorption may affect the sound transmission in the middle ear cavity. No materials (eg, gelatin sponge), which are regularly used in underlay techniques, were inserted in the middle ear cavity. Also, in underlay patients, ABG closure was not always achieved, possibly because of limited mobility for the reconstructed TM. Although it is possible that using an underlay technique might reduce the incidence of residual ABGs after myringoplasty, it is unclear how the underlay technique might affect the relationship between ABG and UVTF. The relationship between ABG and UVTF in underlay patients needs further study.
In terms of practical considerations, LDV is useful for understanding persistent ABG after myringoplasty where there are no obvious causes. Laser Doppler vibrometry has also been used as a preoperative diagnostic tool to detect TM dysfunction in patients with conductive hearing loss, as well as for intraoperative observation of the ossicular chain after ossicular implantation. The present data showed an inverse correlation between ABG at 1 kHz and UVTF, which might be useful when assessing long-term hearing after myringoplasty. In addition, LDV is convenient and noninvasive.
Conclusions
In general, function is determined by structure. The random arrangement of collagen fibers and the thickness of the reconstructed TM may impair sound transmission at the TM, leading to incomplete closure of ABG. 3 Almost 30% of the cases had lower amplitude of TM vibration when measured using LDV. In this study, significant relationships were observed between ABG and UVTF at 1 kHz, and between mean ABG and UVTF across all frequencies. In addition, there was a significant relationship between mean ABG and UVTF across all frequencies for patients with UVTF values >0.08 mm/s/Pa. For post-myringoplasty ABG without readily observable causes, there was a significant relationship between ABG and TM vibration. These results provide new insights in the understanding of this relationship and may help explain ABG after myringoplasty when there are no clear contributing factors.
This work was supported by grants from the 2016 Beijing Capital Clinical Specialized Technology Grant (Z1611000516144), the 2016 Beijing Cultivation and Development of Science and Technology Grant (Z161100005016090), the Priming Scientific Research Foundation for the senior researcher in Beijing Tongren Hospital, Capital Medical University (2015-YJJ-GGL-015), and the Beijing Natural Science Foundation (7142040).
Footnotes
Acknowledgments
The authors sincerely thank Dr Fei Zhao from Cardiff Metropolitan University for his comments and suggestions during manuscript preparation. The authors also thank John J. Galvin III for editorial assistance.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.