
Abstract
The nasopharyngeal bursa is an invaginated space that links the remnants of the notochord with the pharyngeal epithelium. Nasopharyngeal bursitis can occur in the midline of the upper portion of the nasopharynx if the notochord remnants and midline recess continue to persist. Nasopharyngeal bursitis, also known as Tornwaldt cyst, can be divided into cystic and crusting types. Crust types are relatively rare. Electrocauterization of the ulcerative lesion of the crust type is an effective and minimally invasive method. This report presents a case of crust-type nasopharyngeal bursitis that heals spontaneously without electrocauterization therapy.
A 51-year-old man was referred to the Department of Otolaryngology at our university hospital for the evaluation of deep-seated nasal pain with postnasal discharge. He felt the aforementioned symptoms 2 months before his visit and was treated in a local clinic, but his symptoms did not improve. He denied having any history of nasal trauma and surgery or systemic disease. He was worried about the possibility of cancer.
Endoscopic examination revealed an ulcer-like lesion covered with crusts in the midline of the upper posterior wall of the nasopharynx (Figure 1). Magnetic resonance imaging (MRI) was performed to evaluate the possibility of the ulcerative lesion being cancerous; however, it revealed no significant local mucosal thickening or enhancing lesion in the mucosal wall of the nasopharynx and Rosenmuller fossa. The endoscopic and MRI findings were suggestive of crust-type nasopharyngeal bursitis, so we decided to observe the lesion.
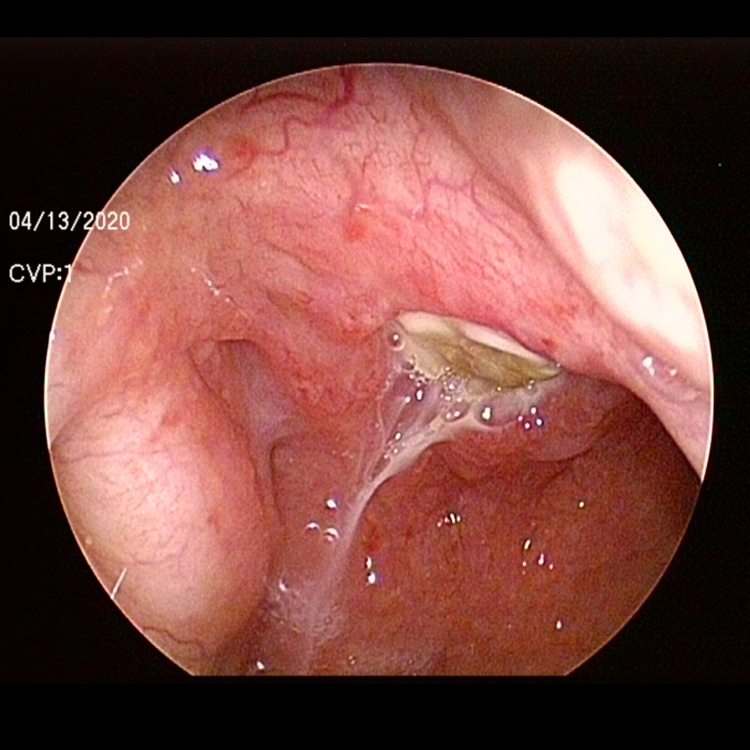
Nasal endoscopy reveals an ulcer-like lesion covered with crusts in the midline of the upper posterior wall of the nasopharynx.
However, nasal endoscopy revealed that the ulcerative lesion was persistent 6 weeks after the first visit (Figure 2A). He presented with postnasal discharge having an unpleasant taste. Biopsy of the lesion and endoscopic electrocautery therapy were recommended; however, he refused it, so we decided to keep observing. Even though the patient was not followed up regularly, nasal endoscopy revealed complete recovery of the ulcerative lesion after 6 months of the first visit (Figure 2B). He had no further deep-seated nasal pain and postnasal discharge with an unpleasant taste.
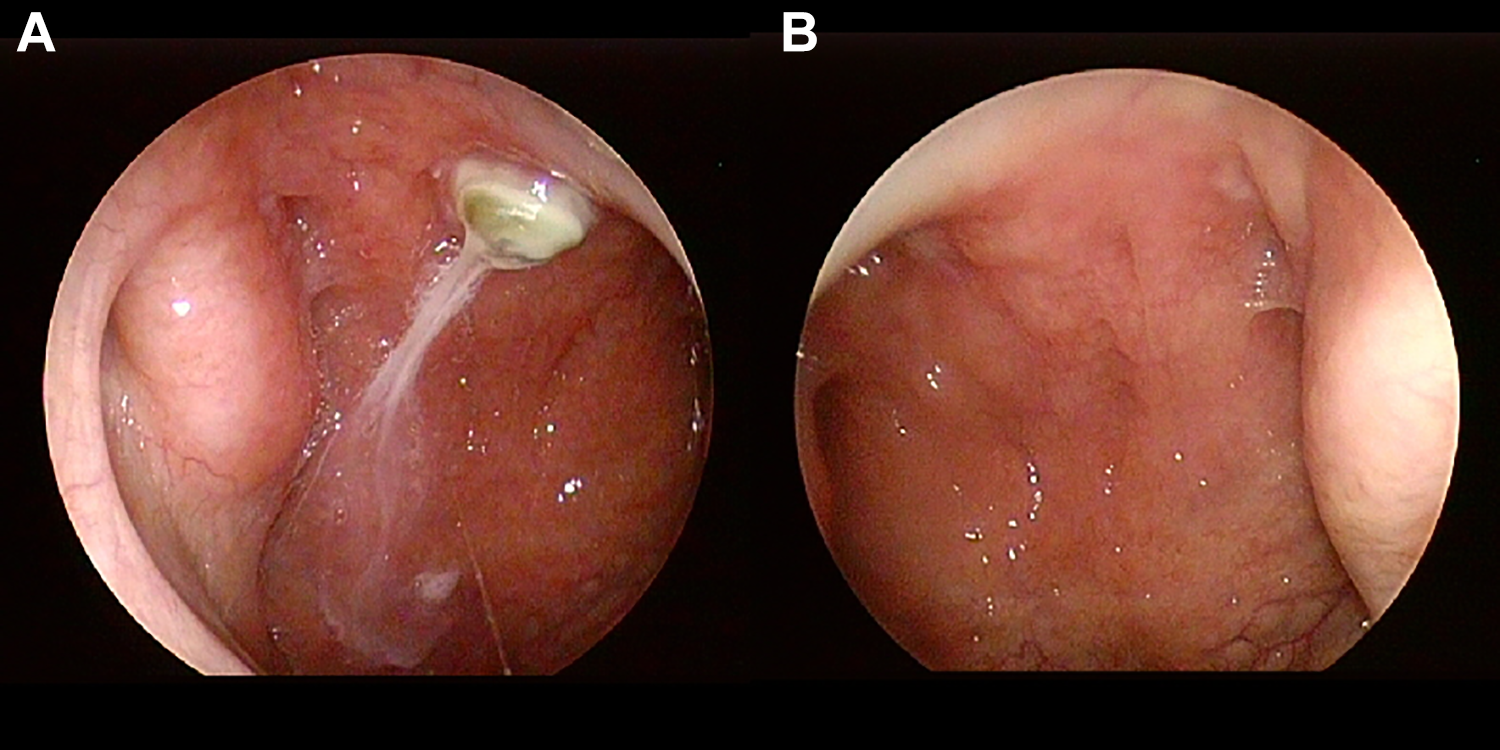
A, Nasal endoscopy reveals that the ulcerative lesion was persistent 6 weeks after the first visit. B, Nasal endoscopy reveals complete recovery of the ulcerative lesion 6 months after the first visit.
The nasopharyngeal bursa is an invaginated space that links the remnants of the notochord with the pharyngeal epithelium. The notochord forms the vertebral column. Nasopharyngeal bursitis, also known as Tornwaldt cyst, can occur in the midline of the upper portion of the nasopharynx if the notochord remnants and midline recess continue to persist. Nasopharyngeal bursitis can be divided into cystic and crusting types. 1 The orifice of the nasopharyngeal bursa is the cystic type when it is obstructed and the crust type when the crust is where it is without obstructing the orifice. Cystic types are more common. Crust types are relatively rare. The foul odor and bad taste can be perceived as the crust falls off. 2
Nasal endoscopy and radiologic tests are required for the proper diagnosis. Magnetic resonance imaging is more useful than computed tomography. The former is suitable for the diagnosis of the cystic type, which it reveals as a soft tissue mass with well-defined margins. The cystic type of nasopharyngeal bursitis might require differential diagnosis with nasopharyngeal cystic lesions such as Rathke pouch cyst, adenoid retention cyst, and branchial cleft cyst. 3 Histologically, cystic types of nasopharyngeal bursitis can be differentiated from the other nasopharyngeal cystic lesions. However, the crust type has no peculiar histological features.
The crust type may require differential diagnosis with nasopharyngeal carcinoma in that it is characterized by ulcerative lesions. The crust type of nasopharyngeal bursitis is accompanied by the crust in the ulcerative lesion, but usually without nasopharyngeal carcinoma. Magnetic resonance imaging and biopsy findings, along with clinical features, are required for the diagnosis of nasopharyngeal carcinoma. Electrocauterization of the ulcerative lesion of the crust type is an effective and minimally invasive method. 2 The endonasal endoscopic approach can ensure a clear visual field and facilitate the use of surgical instruments. This report presents a case of crust-type nasopharyngeal bursitis that heals spontaneously without electrocauterization therapy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.