
Abstract
Sigmoid sinus thrombophlebitis is a severe and potentially fatal intracranial complication of acute otitis media and middle ear cholesteatoma. Early administration of broad-spectrum antibiotics and immediate radical mastoidectomy are the recommended standard treatments; however anticoagulant therapy is always an option worthy of clinical consideration. Here, we report a case of middle ear cholesteatoma complicated with sigmoid sinus thrombophlebitis in a patient who received anticoagulant therapy for 1 year before the operation because of the coronavirus disease 2019 pandemic.
Introduction
Sigmoid sinus thrombophlebitis is an intracranial complication of acute otitis media and cholesteatoma, with potentially serious consequences. It is reported that cholesteatoma is the most common cause of sigmoid sinus thrombophlebitis.1-3 In recent years, with the increase in antibiotic resistance, the incidence has started to rise again.
Early application of broad-spectrum antibiotics and surgical intervention are first-line therapy for sigmoid sinus thrombophlebitis. However, the role of anticoagulant therapy in sigmoid sinus thrombophlebitis is still widely debated, especially the effect of postoperative anticoagulation therapy. This article reports a case in which anticoagulant therapy was administered before the operation, reviews the relevant literature, and presents a new and feasible approach to the use of anticoagulant therapy for sigmoid sinus thrombophlebitis.
Case Report
A 61-year-old male patient came to our department for treatment because of intermittent high fever lasting for a week, accompanied by right ear pain, hearing loss, dizziness, headache, nausea, and vomiting. Physical examination showed a large amount of purulent discharge in the right external auditory canal, edema, and tenderness behind the ear. Temporal area computed tomography (CT) showed possible mastoiditis and cholesteatoma in the right middle ear, involving the right auditory ossicles (Figure 1). Cranial magnetic resonance imaging (MRI) and magnetic resonance venography (MRV; Figure 2) showed abnormal signals in the right middle ear tympanum and mastoid cell together with a filling defect in the right transverse sinus and sigmoid sinus, which indicated right middle ear cholesteatoma and thrombosis of the right transverse sinus and sigmoid sinus.
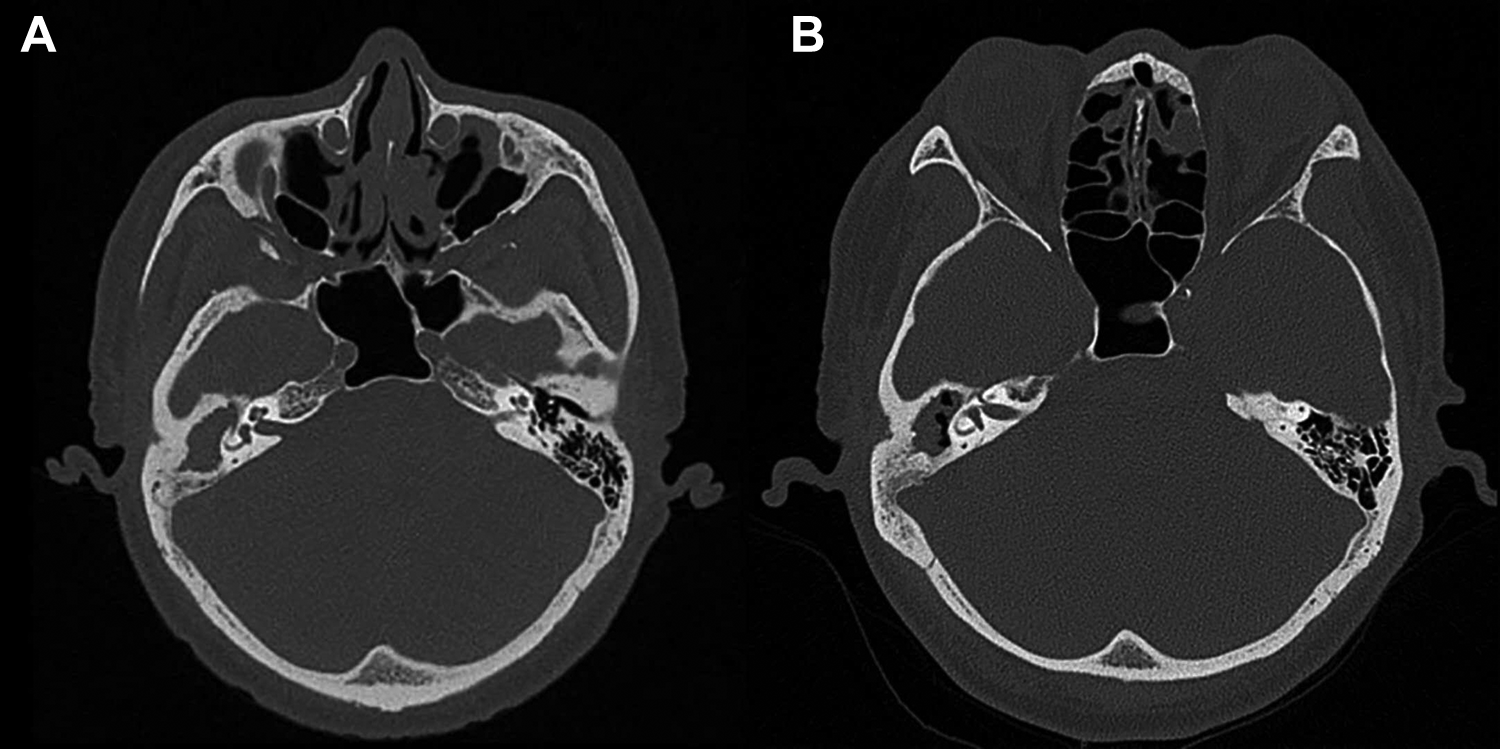
Temporal bone CT showed (A) possible mastoiditis and cholesteatoma in the right middle ear and (B) a reduction in the soft tissue shadow in the mastoid cavity compared to the pretreatment image. CT indicates computed tomography.
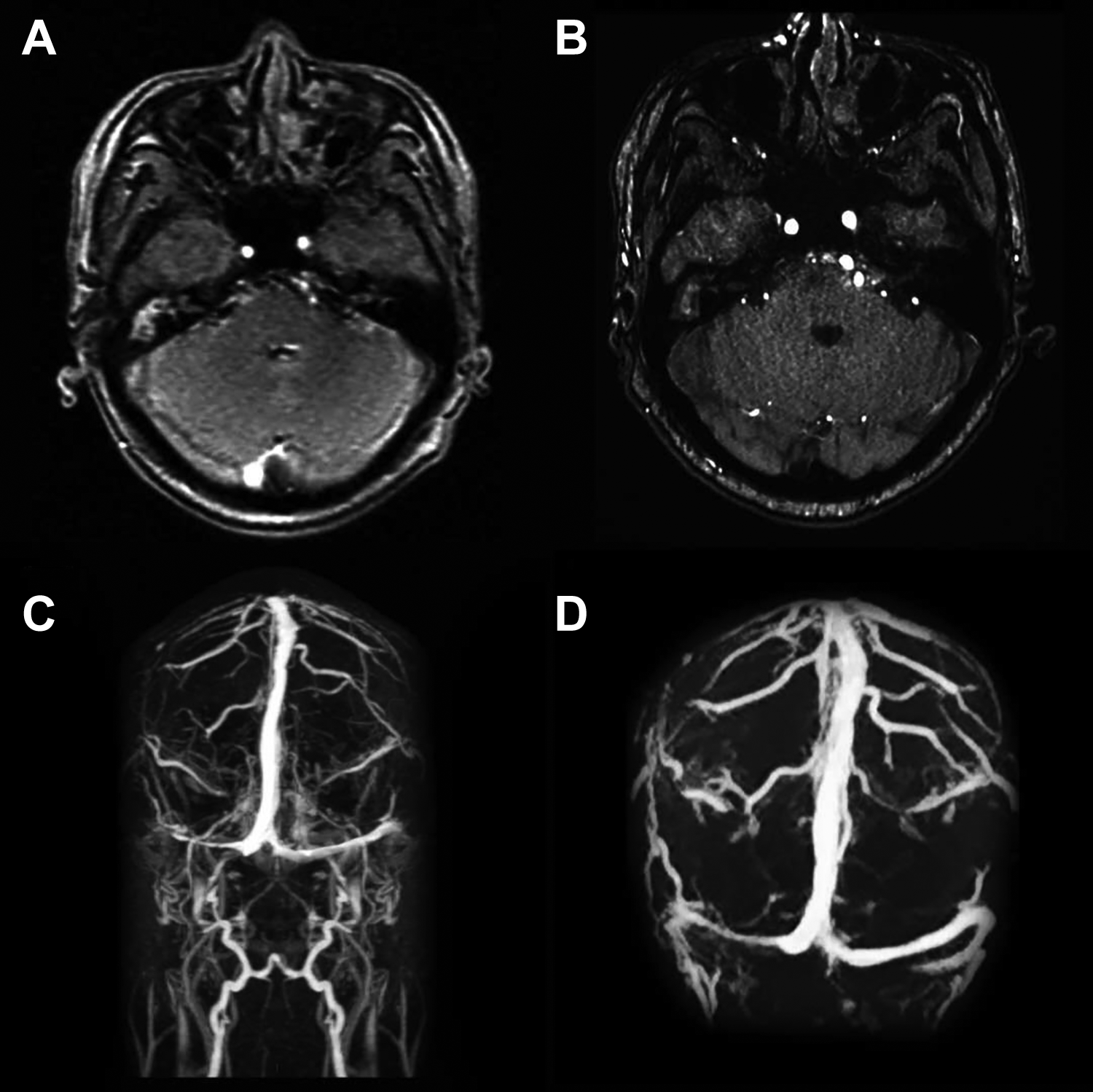
MRI suggested: (A) right side sigmoid sinus thrombosis; (B) a slightly smaller thrombus area than before treatment. MRV showed (C) the filling defect of the right transverse sinus and sigmoid sinus; (D) a slightly smaller thrombus range than before treatment. MRI indicates magnetic resonance imaging; MRV, magnetic resonance venography.
After consultation with a neurologist, the patient followed their advice and received treatment for 15 days in the Department of Neurology before surgery. Craniocerebral CT venography showed a stripe filling defect shadow in the right lateral transverse sinus, sigmoid sinus, and internal jugular vein, indicating thrombosis, thrombophlebitis, and right middle ear cholesteatoma. The patient was given a subcutaneous injection of enoxaparin sodium (4000 IU) and oral administration of warfarin sodium tablets (1.5 mg) for anticoagulant therapy, as well as anti-infection and intracranial hypertension treatment. Due to the coronavirus disease 2019 (COVID-19) pandemic, the patient continued taking oral warfarin sodium tablets (3 mg) for 1 year and was regularly tested for clotting function.
Compared to the pretreatment examination, reexamination of cerebral venography indicated that the thrombus area was slightly smaller and the local venous sinus was slightly narrower, indicating the slowing down of thrombosis (Figure 2). Computed tomography of the temporal bone showed a slight decrease of the soft tissue shadow in the mastoid cavity compared to the initial finding (Figure 1). The patient then underwent open radical mastoidectomy and sigmoid sinus exploration under general anesthesia. During surgery, we found that the surface of the sigmoid sinus bone wall was intact and light red in color (Figure 3). A follow-up examination after discharge showed that the patient had recovered well.
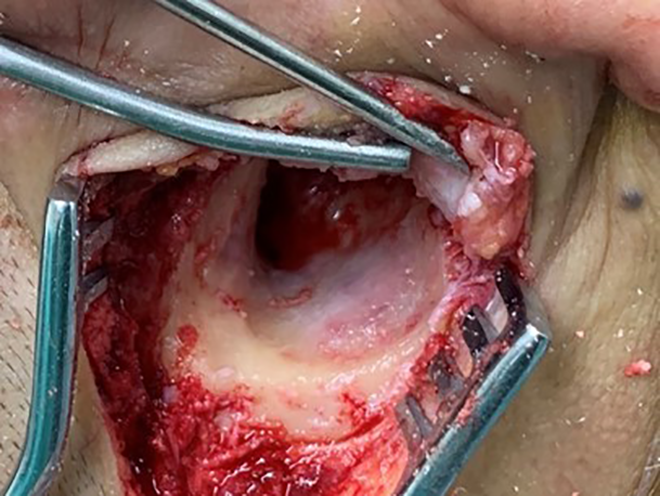
The surface of the sigmoid sinus bone wall was intact and light red in color.
Discussion
Due to the extensive use of antibiotics, the incidence of sigmoid sinus thrombophlebitis has been on the rise in recent years, and symptoms which were considered typical of the disease, such as “picket fence” fever, headache, dizziness, nausea, vomiting, neck stiffness, erythema, and altered mental status, with otorrhea, retroauricular edema, and pressing pain (Griesinger sign),4-8 are no longer typical. The patient did not have typical symptoms of “picket fence” fever after admission, owing to his treatment with antibiotics before admission. However, the patient had symptoms of intracranial hypertension such as headache, dizziness, nausea, and vomiting. Retroauricular edema and pressing pain (Griesinger sign) are the pathological features of sigmoid sinus thrombosis and mastoid vein thrombosis,9,10 therefore Griesinger sign can be considered as a possible warning sign of sigmoid sinus thrombosis. In this case, the patient had this typical sign.
Cholesteatoma has been reported to be the most common cause of sinus sigmoid thrombophlebitis.1-3 Possible mechanisms of the disease caused by middle ear cholesteatoma are6,11,12: (1) cholesteatoma tissue directly destroys the bone plate of the sigmoid sinus wall, causing compressive necrosis of the intima and the formation of mural thrombus or (2) when the bone wall of the sigmoid sinus is intact, inflammatory lesions extend from the tiny vessels or guide veins in the mastoid cavity to the sigmoid sinus, leading to thrombosis. Based on intraoperative findings, we predict that in this patient, the disease may have been caused by the second pathogenesis.
Early use of broad-spectrum antibiotics and surgical intervention are recognized as the preferred treatment for sigmoid sinus thrombophlebitis. Common operations include5,7,8: radical mastoidectomy, sigmoid sinus aspiration or incision, thrombectomy, and internal jugular vein ligation. Some authors have suggested that relatively conservative surgical treatment can achieve a good prognosis, without the need to open the sigmoid sinus or remove blood clots or ligate the internal jugular vein.8,12 According to the fourth type of the new surgical classification for endoscopic surgery of middle ear cholesteatoma proposed by Sun et al, 13 this patient underwent radical mastoidectomy with microscopic guidance.
At present, the role of anticoagulant therapy in sigmoid sinus thrombophlebitis is still controversial. The risks of anticoagulant therapy include embolism, drug interactions, induced thrombocytopenia, bleeding, as well as hemorrhagic skin necrosis.2-5 Nevertheless, the incidence of complications caused by anticoagulants is low and usually nonfatal, therefore some authors have suggested that it is reasonable to consider anticoagulation treatment before obtaining more evidence. 14 According to the guidelines and recommendations of the British Society of Haematology on the treatment of cerebral venous thrombosis in children, the anticoagulation group achieved better survival and cognitive outcomes, even if there was no evidence that anticoagulation increased the recanalization rate. 15
Some authors recommended anticoagulant therapy for its potential benefits, such as limiting the spread of thrombus, improving sinus recanalization, and reducing sequelae of the nervous system.4,7,16,17 Ropposch et al 2 treated patients with ordinary heparin for 3 days after surgery, followed by low molecular weight heparin for 3 months, and reported that no complications occurred.2,3 Coutinho et al 18 treated 16 children with anticoagulation therapy combined with antibiotics and radical mastoidectomy. A higher recanalization rate was obtained and no anticoagulant side effects were observed. Ulanovski et al 12 reported that 22 (91.7%) children received low molecular weight heparin within 3 to 6 months after surgery, again without any complications caused by the anticoagulant therapy. Scherer and Jea 11 reported the case of a 6-year-old child who received enoxaparin for 6 months after surgery, and MRI showed his dural sinus venous thrombosis had disappeared completely.
However, preoperative anticoagulant therapy for sigmoid sinus thrombophlebitis has rarely been studied. In this case, the patient received anticoagulant and anti-infective treatment before the operation. One year after commencing warfarin maintenance treatment, due to delays caused by the COVID-19 pandemic, re-examination of cerebral venography showed that the thrombus range and the local venous sinuses were slightly smaller than before (Figure 2). Furthermore, no adverse complications occurred during anticoagulation treatment. The patient then underwent radical mastoidectomy and recovered well. The success of long-term preoperative anticoagulation therapy in this case suggested a new and feasible use of anticoagulant therapy for sigmoid sinus thrombophlebitis.
In spite of these positive reports, some authors do not recommend anticoagulation therapy. Rosenberg and Parikh 19 treated patients with low molecular weight heparin for 7 months after surgery and found no sinus recanalization in the patient’s follow-up MRV at 3 and 19 months. Raja et al 5 reported that patients’ venous sinuses were recanalized without anticoagulation after surgical intervention and antibiotic treatment for 6 weeks. Prasad et al 7 believed that radical mastoidectomy and removal of infected tissue are the main treatment methods of sigmoid thrombophlebitis, and anticoagulation is usually not required.
In summary, because of the increase in drug-resistant bacteria, patients’ symptoms may no longer be typical, which brings new challenges to clinicians. Early diagnosis and timely treatment can improve the poor prognosis of patients with sigmoid thrombophlebitis. Computed tomography and MRI play an important role in diagnosis and treatment. Now, the choice of anticoagulation and mastoid opening time of otogenic sigmoid sinus thrombophlebitis is still a clinical problem to be discussed. Receiving anticoagulant therapy before surgery can prevent the development of thrombosis and other intracranial complications, thereby reducing the risk for surgery. Therefore, preoperative anticoagulation therapy is worth considering as a therapeutic strategy. In future, multicenter studies will be needed to compare the efficacy of various treatments enabling clear conclusions to be drawn concerning the best treatment.
Footnotes
Authors’ Note
Lanlai Yuan and Jie Yuan contributed equally to this work. A legally authorized representative of the patient gave written consent for the publication of this case report.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.