
Abstract
Successful cochlear implantation in the setting of labyrinthitis ossificans is challenging. Various surgical techniques are described to circumvent the region of ossification and retrograde insertion of the electrode array is one such option. While reverse programming is often recommended in the case of retrograde electrode insertion, we present our experience of retrograde electrode insertion for labyrinthitis ossificans, where standard programming was adopted due to patient preference and provided satisfactory outcomes.
Keywords
A 44-year-old diabetic man with hypertension and associated nephropathy presented to the otolaryngology department with sudden bilateral profound sensorineural hearing loss of 8 months’ duration, following septicemia complicating a urinary tract infection. His audiogram and brainstem-evoked response audiometry showed bilateral profound hearing loss. The hearing aid trial was out of speech spectrum and his Categories of Auditory Performance (CAP) score was zero at presentation. Magnetic resonance imaging and high-resolution computed tomogram (HRCT) of the temporal bone and brain showed features of labyrinthitis ossificans (right more than left) with decreased fluid signal involving bilateral inner ear (scala vestibuli more than scala tympani and the semicircular canals; Figure 1).
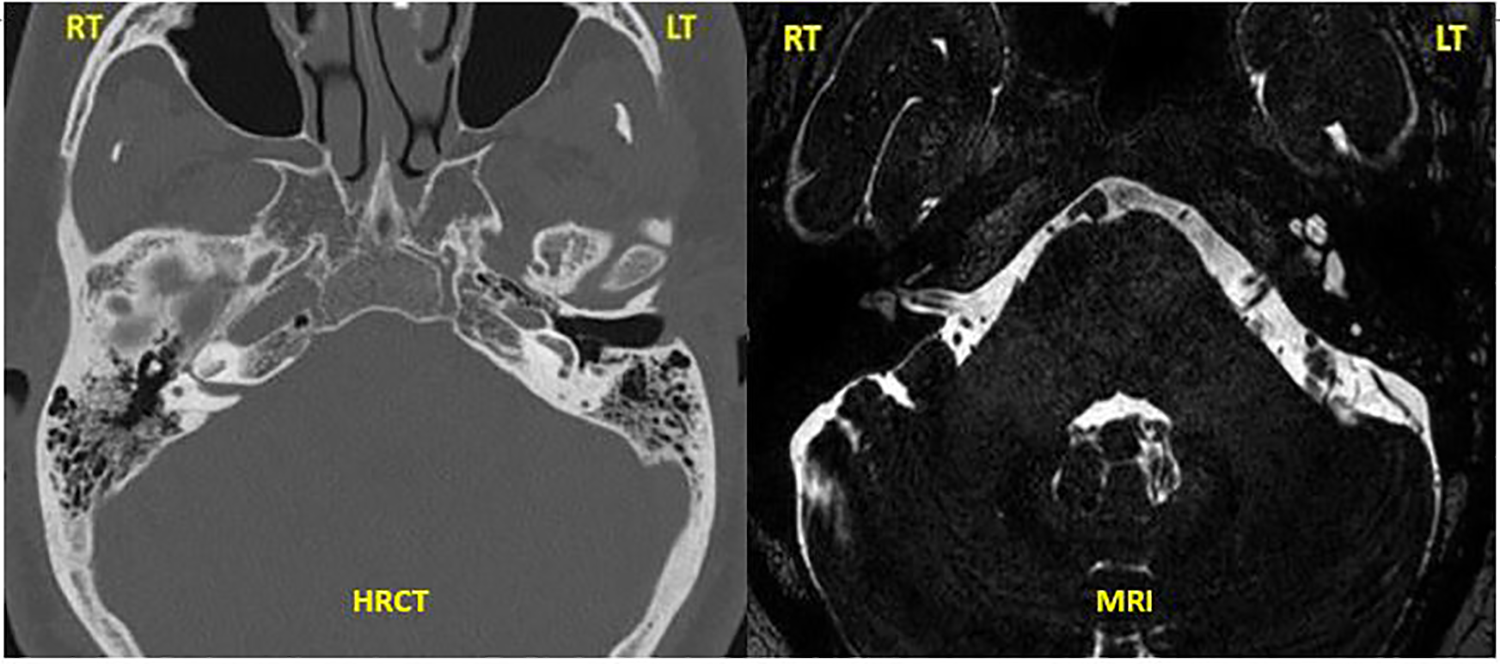
High-resolution computed tomogram of the temporal bone and MRI brain T2 drive sequence axial view showing complete ossification of all turns of the cochlea with loss of fluid signal on the right side and basal turn ossification on the left side. MRI indicates magnetic resonance imaging.
He underwent a left cochlear implantation via a standard mastoidectomy and facial recess approach under general anesthesia. A partial drill out of the basal turn was attempted until a patent lumen was seen; however, only 4 electrodes of a dummy electrode array could be inserted. Therefore, a middle-turn cochleostomy was performed. On attempting anterograde (apical) electrode insertion with dummy electrodes, only 3 electrodes could be inserted. Hence, a retrograde technique was adopted which allowed successful insertion of 12 electrodes from the middle turn toward the basal turn. We used an Advanced Bionics 1J implant (HiReS 90K ADVANTAGE CI with HiFOCUS 1J ELECTRODE and Naida Q30 speech processor, Advanced Bionics India Pvt. Ltd.; Figure 2). Intraoperative impedances were normal, and neural response imaging (NRI) responses were obtained for the first 8 electrodes.
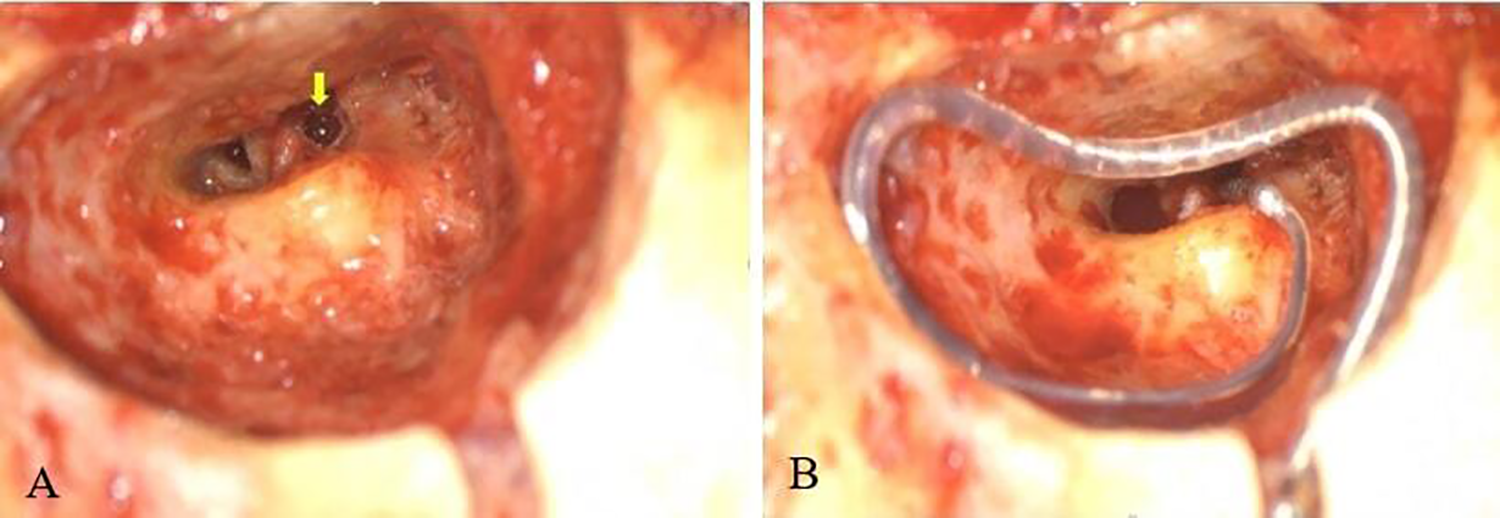
A, Middle-turn cochleostomy (yellow arrow) via extended facial recess approach with (B) retrograde electrode insertion and securing of the implant.
Postoperatively, the position of the electrode array was confirmed by a plain X-ray, modified Stenvers view. During the initial activation of the implant, reverse programming was tried, considering the retrograde insertion of the electrode array, but the patient had discomfort with the sound stimulus. Hence, a regular programming was adopted. His aided audiogram showed responses within the speech spectrum (Figure 3) and postoperative NRI responses were good up to the eighth electrode. His auditory perception improved subsequently and a CAP score of 11 was obtained at 12 months following surgery. He was able to have a telephonic conversation with familiar people.
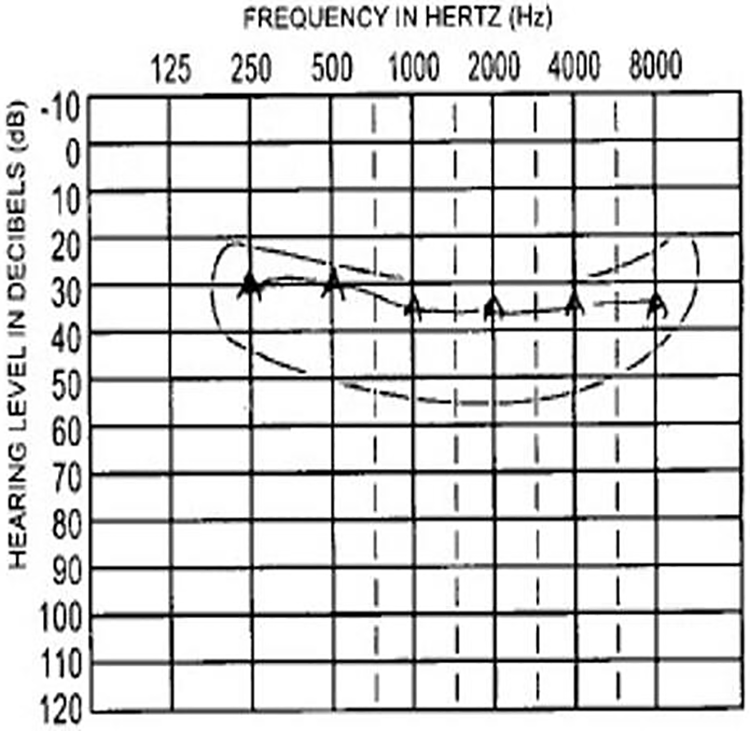
Postoperative aided audiogram of the left ear showing responses within the speech spectrum.
Labyrinthitis ossificans is a cause of progressive and sometimes rapidly progressive sensorineural hearing loss. A cochlear implant should be considered early as the advancing ossification process within the cochlea can prevent cochlear implantation at later stages.1-3 Various surgical approaches 3 have been described in obliterated cochlea such as, partial drill-out of the basal turn, scala vestibuli insertion, complete drill out of the basal turn, middle-turn cochleostomy with anterograde electrode insertion, and middle-turn cochleostomy with a double electrode array insertion. If none of these are possible then auditory brainstem implant is an option. The middle-turn cochleostomy is performed 2.5 mm anterior to the oval window and inferior to the processus cochleariformis. The electrode array can be inserted in an anterograde (preferred) or retrograde manner if a double electrode array is not available. The retrograde approach requires reprogramming of the electrodes as the standard program codes for higher frequencies at the basal electrodes. In our patient, however, we did a standard programming as the patient found the sound quality provided by reverse programming intolerable. Senn et al have reported good open set speech discrimination scores despite intracochlear array direction changes during retrograde cochlear implantation. 4 Postoperatively, a good CAP score improvement can be achieved without altering the programming strategy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflict of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.