
Abstract
Objectives:
Studies investigating the effects of intravenous (IV) ketamine in pain management after septorhinoplasty is limited. This study aims to evaluate the efficacy of low-dose IV infusion of ketamine on pain scores.
Methods:
This randomized, prospective, double-blind study was conducted with 48 patients who underwent septorhinoplasty. Intravenous ketamine bolus (0.5 mg/kg) was administered to the ketamine group (group K, n = 24) at anesthesia induction, and ketamine infusion was continued (0.25 mg/kg/h) during the surgery. In the control group (group C, n = 24), the same protocol was administered using saline instead of ketamine. Furthermore, 50-mg dexketoprofen trometamol was administered to both groups 30 minutes before the end of the surgery. Then it was repeated at the 12th and 24th hours postoperatively. Pain scores were evaluated with the visual analogue scale. Consumptions intraoperative of opioid and sevoflurane, rescue opioid requirement, patient satisfaction, and side effects were recorded.
Results:
Pain scores were significantly lower in group K at all postoperative periods (P < .05). There was no significant difference between the groups in terms of intraoperative sevoflurane and remifentanil consumptions (P > .05). Rescue opioid analgesic requirements were significantly lower in group K than group C (0/24 vs 6/24, respectively; P = .022). Side effects were similar between the groups (P > .05).
Conclusion:
We recommend the administration of low-dose ketamine infusion during septorhinoplasty surgery because it reduces the requirement for rescue opioid analgesia and postoperative pain scores.
Introduction
The purpose of septorhinoplasty, one of the most common aesthetic surgeries, is to create a functional nose with a natural appearance that is compatible with other features of the face and ensures comfortable breathing. 1 Despite advances in surgical techniques, pain management during nasal surgery remains a significant challenge. 2 Inadequate pain management directly affects the success of the surgical procedure and also negatively affects health care costs by increasing opioid use and recovery time. 3
Although opioids that can be used for postoperative pain are quite effective analgesics, concerns about their adverse effects have increased the interest in alternative analgesics. 4 Many pharmacological or non-pharmacological methods have been attempted for pain management after septorhinoplasties such as nonsteroidal anti-inflammatory analgesics, intravenous (IV) lidocaine infusion, α-2 receptor agonists, gabapentinoids, and intraoperative local anesthetic infiltration. 5 -7
In the last 2 decades, many studies have been conducted on the effects of ketamine on postoperative pain, chronic pain, depression, and postop delirium treatment. 8 -11 Ketamine is a phencyclidine derivative synthesized in 1962. 12 It is the only anesthetic agent with analgesic, hypnotic, and amnesic effects. It is an IV anesthetic used in general induction such as thiopental and propofol. Acting as an NMDA (N-methyl-D-aspartate)-receptor antagonist, ketamine has an analgesic effect at the spinal cord level. The NMDA receptors have an essential role in initiating and maintaining spinal nociceptive events after tissue damage, nerve dysfunction, and surgery. 13 Despite being a potent analgesic, the use of this agent is limited because it causes hallucinations and agitation during awakening. However, when used at a subanesthetic dose, it still shows a strong analgesic effect, and the psychomimetic adverse effects of ketamine are infrequent at these doses. 14 To the best of our knowledge, this prospective, double-blind, randomized study is the first to evaluate the analgesic effectiveness of perioperative low-dose ketamine infusion in septorhinoplasty surgery.
The primary aim of this study was to investigate the effect of IV low-dose ketamine infusion on pain scores in septorhinoplasty surgery, and the secondary aims were to evaluate its effect on rescue analgesia, patient satisfaction, and intraoperative anesthetic consumption.
Materials and Methods
Ethical approval for this prospective, randomized, double-blind study was obtained from the local ethics committee of Ataturk University Faculty of Medicine. A total of 48 patients aged 18 and 45 years were American Anesthesiologists Association (ASA I-II) and for whom septorhinoplasty surgery was planned were included in the study. All patients were informed in detail about the anesthesia and pain assessment procedures, and their written consent was obtained for participation in the study.
The ASA III-IV patients, those allergic to ketamine; those with severe cardiac, hepatic, and renal disease; those with a long-term opioid and nonopioid analgesic use history and pregnant women; those unable to communicate; those with a history of psychosis; those using 3 or more psychotropic drugs; and those with severe hypertensive and glaucoma were excluded from the study. Using a computer program, patients were randomly assigned into 2 groups at a ratio of 1:1. These groups were group control (group C, n = 24) and low-dose ketamine infusion group (group K, n = 24). Postoperative pain assessors, patients, and practitioners were blinded by the study groups and the drug content. Saline preparations used for group C were prepared with the same volumes of preoperative and intraoperative infusion solutions as those prepared for the group K to guarantee double-blind.
The standard monitoring procedure, including electrocardiography, oxygen saturation, and noninvasive blood pressure, was administered. Crystalloid infusion solution (8 mL/kg/h) was maintained throughout the operation. All surgeries were performed using the same surgical technique by the same surgical team.
Study Protocol
Anesthesia induction was performed with midazolam (1 mg), propofol (2-3 mg/kg), and rocuronium (0.6 mg) in all patients. Remifentanil 0.5 to 1 µg/kg was administered over 60 to 90 seconds. Remifentanil infusion was maintained during the surgery with systolic blood pressure not exceeding 100 mm Hg. The maintenance of anesthesia was conducted with 2% sevoflurane. In the last 30 minutes of the surgery, dexketoprofen trometamol (50 mg) was administered IV. Subsequently, it was given at the 12th and 24th hours postoperatively. Remifentanil infusion was terminated at the end of the surgery.
The determination of the ketamine dosage protocol in this study is based on previously published relevant studies. To induce anesthesia, ketamine 0.5 mg/kg bolus was administered IV to the patients in group K followed by ketamine infusion 0.25 mg/kg/h during the surgery. In group C, the same protocol was implemented using normal saline. The infusions were terminated in both groups postoperatively.
Surgical Technique
Septorhinoplasty was performed in all patients with the same technique and the same surgical team. Open technical septorhinoplasty surgery was performed. Lidocaine infiltration was performed to reduce bleeding by providing vasoconstriction. It was applied to the anterior, middle, and posterior parts of the septum, incision line, valve area, and lateral osteotomy lines, and the incision was started. After the incisions were completed, the skin and soft tissue were elevated to reveal the nasal roof. Upper lateral cartilages were visualized and separated from the septum. The graft was removed from the septum. Filing, resection, and reduction were performed. With osteotomies, the bone pyramid was freed from the frontal and maxillary bones and reshaped. Spreader grafts were placed. After suturing, a tampon was inserted into the nose, and fixation was performed using plaster and external splint.
Postoperative Analgesia Management and Outcomes
In both groups, patients were administered IV 50 mg dexketoprofen trometamol 30 minutes before the end of the surgery, and this administration was repeated at the 12th and 24th hours postoperatively. Pain score evaluation and the other examinations of the patients was performed by an anesthesiologist blinded to the analgesic drugs and grouping. Visual analog scale was used to evaluate the state of postoperative analgesia (visual analogue scale [VAS] 10 = most severe pain, 0 = no pain). Tramadol 1 mg/kg described as a rescue analgesic in patients with a VAS score of ≥4. Central nervous system side effects (hallucinations and nightmares), double vision, nausea, vomiting, hypersalivation, and nystagmus were recorded during a 24-hour follow-up. Intraoperative consumptions of remifentanil and sevoflurane were recorded. Patient satisfaction was classified from 1 to 4 (1 = poor, 2 = moderate, 3 = good, and 4 = excellent).
Statistical Analysis
Statistical analysis was performed on SPSS software version 22.0 (IBM Corp). Descriptive statistics were presented as means ± SD. The histogram and Kolmogorov-Smirnov tests were used to determine the distribution of values, and χ2 or Fisher exact test was used to compare the categorical values between groups. The student t test was used to analyze normally distributed data containing continuous variables. Mann-Whitney U test was used for non-normally distributed values. For the statistical significance, P < .05 was considered.
Results
Eligible patients for this study were analyzed and are presented in a Consolidated Standards of Reporting Trials flow diagram (Figure 1).
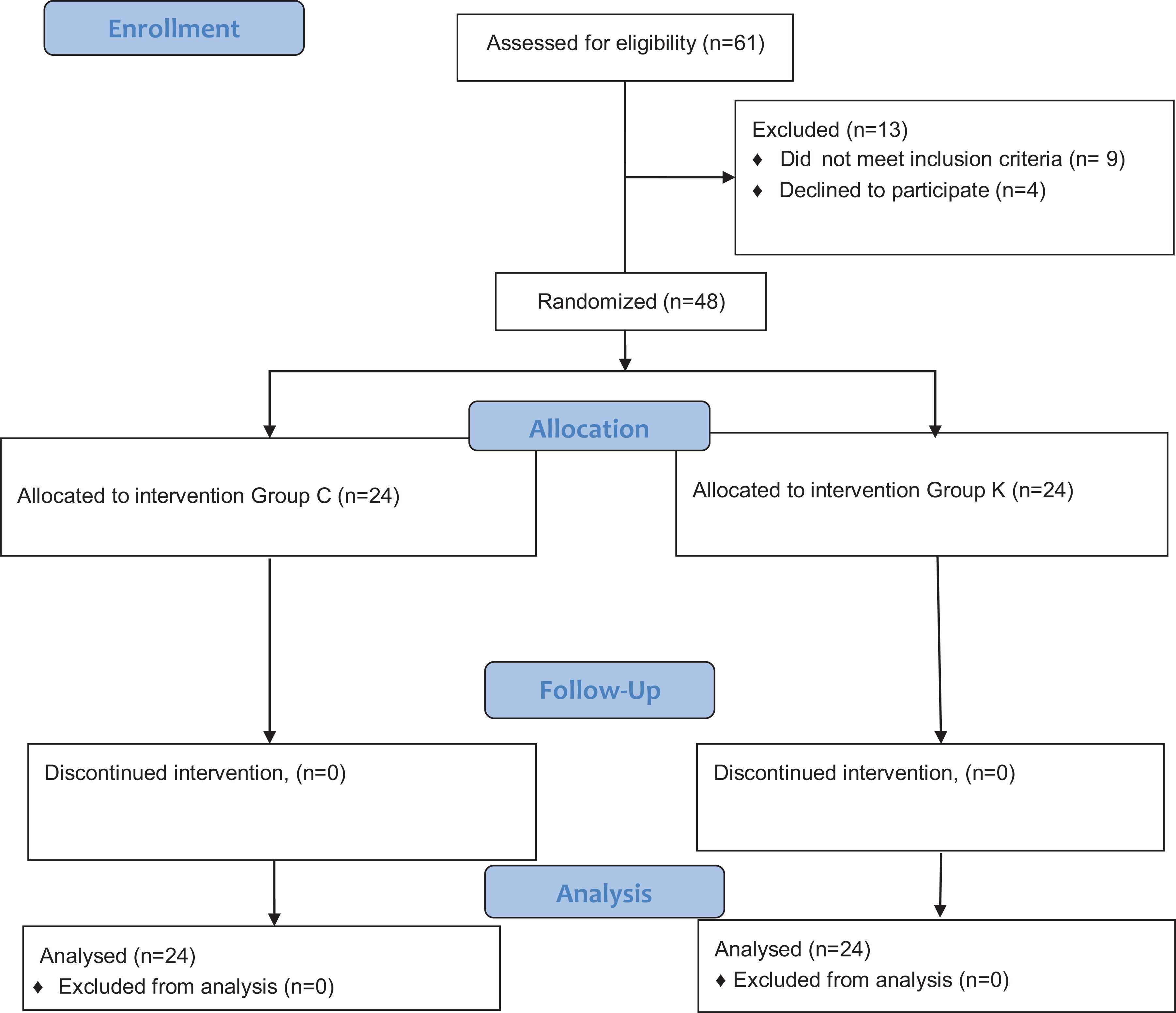
CONSORT diagram. CONSORT indicates Consolidated Standards of Reporting Trials.
No statistical difference was observed between groups in terms of demographic data (age, weight, gender, ASA classification, duration of anesthesia, and operation time). Details are presented in Table 1. Details are presented in Table 1. Likewise, vital parameters were similar between groups (P > .05).
Demographic and Clinical Data of Study.a
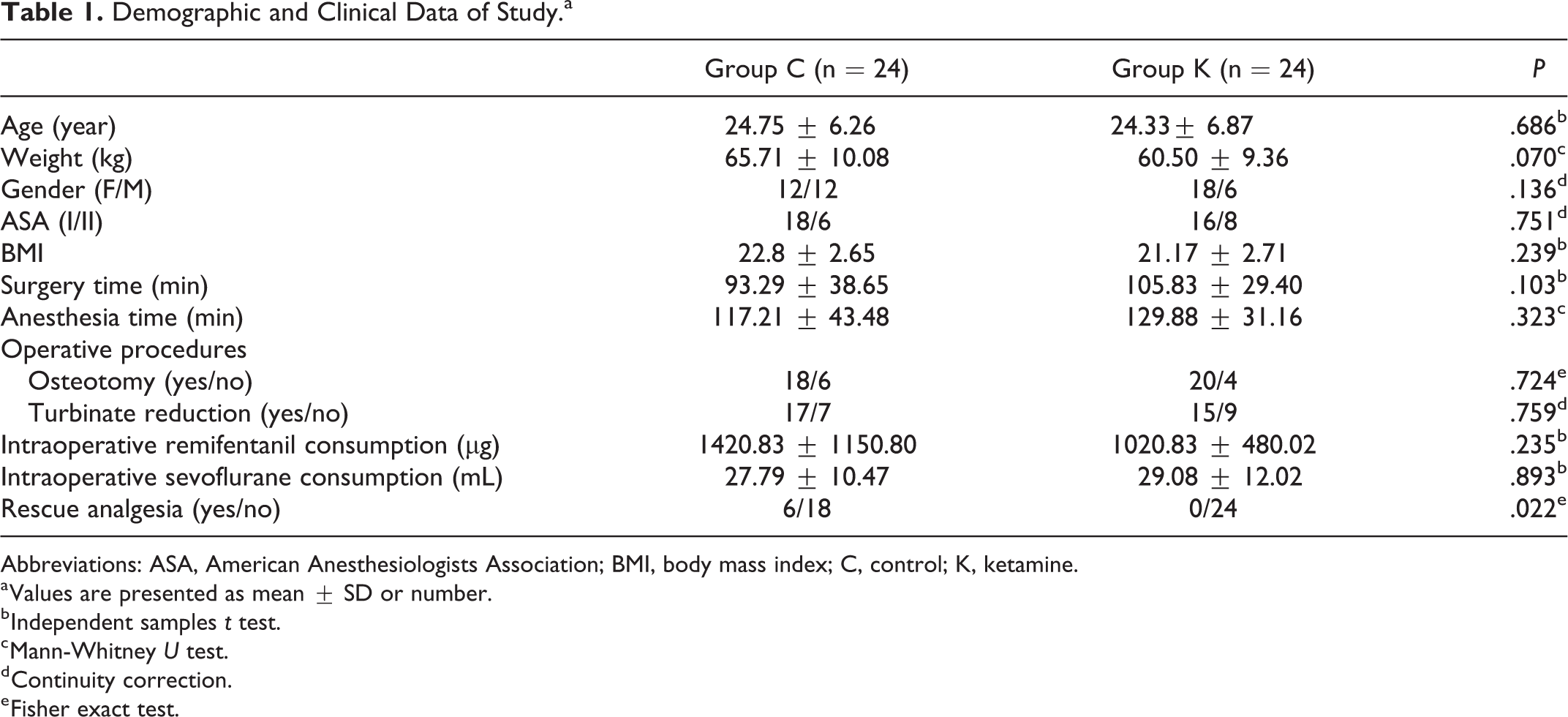
Abbreviations: ASA, American Anesthesiologists Association; BMI, body mass index; C, control; K, ketamine.
a Values are presented as mean ± SD or number.
b Independent samples t test.
c Mann-Whitney U test.
d Continuity correction.
e Fisher exact test.
Visual analogue scale scores were significantly higher in group C than in group K at postoperative 30 minutes, 1, 2, 4, 8, 12, and 24 hours (P < .05; Table 2). The need for additional opioid analgesics was significantly higher in group C than in group K (6/24 vs 0/24, respectively, P = .022).
Pain Scores.a
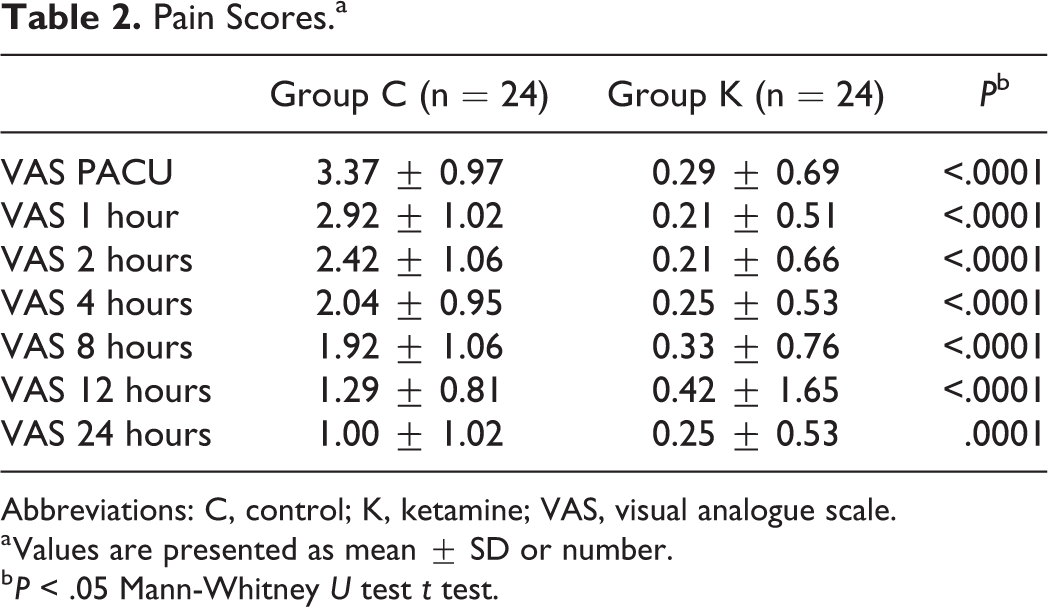
Abbreviations: C, control; K, ketamine; VAS, visual analogue scale.
a Values are presented as mean ± SD or number.
b P < .05 Mann-Whitney U test t test.
No difference was observed in terms of the intraoperative remifentanil consumption between group C and group K (1420.83 ± 1150.80 µg vs 1020.83 ± 480.02 µg, P = .235). Additionally, no difference was observed in terms of the intraoperative sevoflurane consumption between group C and group K (27.79 ± 10.47 mL vs 29.08 ± 12.02 mL, P = .893).
Patient satisfaction was higher in group K (P = .003). Nausea was observed in 4 patients in group C and 1 patient in group K, but there was no statistically significant effect (P = .348). Furthermore, there were no other side effects (vomiting, hallucination, and arrhythmia) observed in the 2 groups (P > .05; Table 3.).
Side Effects and Patient Satisfaction.a
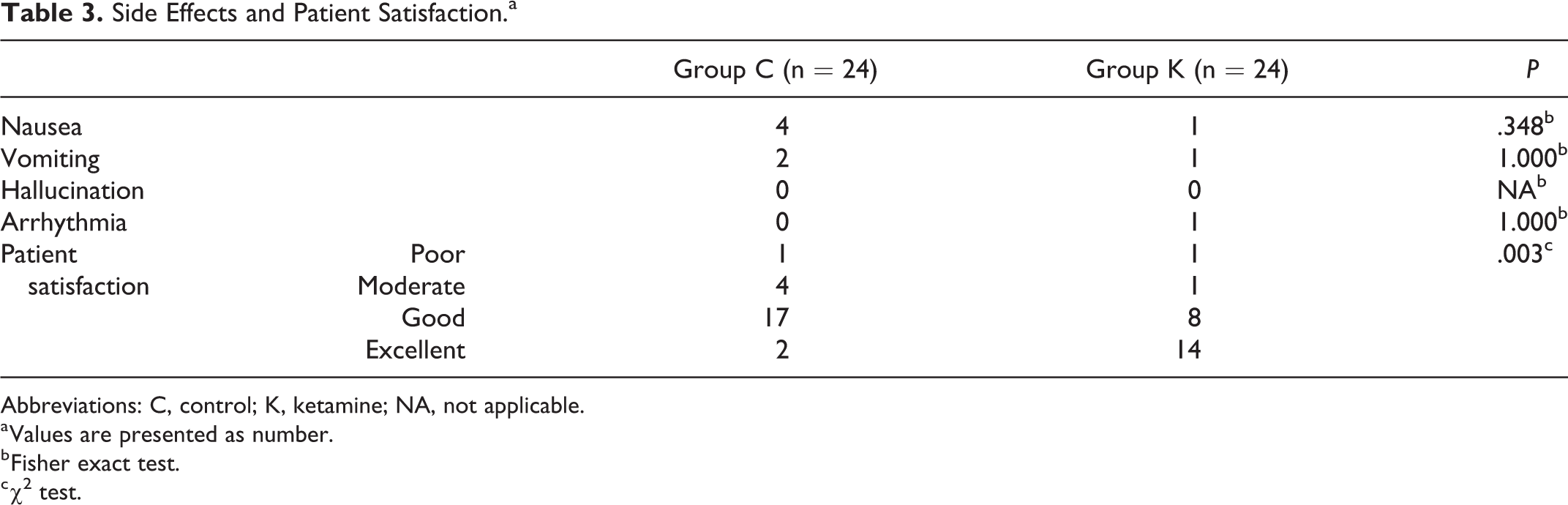
Abbreviations: C, control; K, ketamine; NA, not applicable.
a Values are presented as number.
b Fisher exact test.
c χ2 test.
Discussion
We investigated the postoperative analgesic effect of low-dose ketamine infusion during septorhinoplasty. We showed that IV ketamine infusion significantly reduced postoperative pain during the first 24 hours compared to group C. Additionally, IV ketamine significantly reduced the use of postoperative rescue opioid analgesia.
In patients undergoing septorhinoplasty, soft tissue injury, and severe pain due to osteotomy may occur during the postoperative period. 15 Early mobilization, shortened hospitalization, reduced hospital costs, and increased patient satisfaction can be achieved with effective postoperative pain management. The American Pain Society recommends IV ketamine as a component of multimodal analgesia in adults undergoing extensive surgery, especially those with opioid tolerance. 16 Although ketamine has a clinical history of >50 years in anesthesiology practice, it is still not used to its full extent due to its psychotomimetic side effects. This drug is an NMDA-receptor antagonist and provides both analgesic and antihyperalgesic effects by binding to phencyclidine receptors in NMDA channels and non-competitively inhibiting glutamate activation. 17
Whether ketamine acts as an anesthetic or analgesic depends on the dose administered. Especially in recent years, its use in the treatment of chronic pain, postoperative pain, and depression has made ketamine popular again. When used as an anesthetic agent, the induction dose of ketamine is about 1 to 2 mg/kg; in contrast, when used as an analgesic, the IV subanesthetic bolus dose should be <1 mg/kg, and the infusion dose should be <1.2 mg/kg/h. 18
In different studies, low-dose ketamine was used to provide postoperative analgesia. Low-dose ketamine is used for postoperative analgesia at 0.1 to 0.5 mg/kg bolus and 0.1 to 0.25 mg/kg/h doses for cholecystectomy, spinal fusion surgery, and breast surgery. 8,19,20 Consistent with the literature, IV 0.5 mg/kg bolus dose followed by 0.25 mg/kg/h infusion during the surgery was preferred in the present study.
Low-dose ketamine reduces pain and opioid consumption as well as the risk of opioid-induced hyperalgesia. 21 In systematic reviews, low-dose ketamine has been shown to reduce opioid consumption by 32%. 22 Studies show that low-dose ketamine reduces postoperative pain scores by 87%, 59%, and 54.5%. 23 -25 Furthermore, ketamine-related side effects are less in these subanesthetic doses. Although very rare under general anesthesia, benzodiazepine premedication reduces the psychotomimetic side effects. 22 Therefore, in the present study, we performed midazolam premedication during anesthesia induction to avoid ketamine-related psychotomimetic side effects. Other reasons for the absence of psychotomimetic side effects might be the administration of ketamine under general anesthesia or low-dose administration.
Studies report that ketamine provides a significant reduction in the minimum alveolar concentration (MAC) of sevoflurane. 26 Although, animal studies show a decrease in the MAC of sevoflurane with ketamine administration, 27,28 there was no difference in intraoperative opioid and sevoflurane consumption in our study.
The prevailing view for postoperative pain management is that multimodal analgesia techniques are superior to conservative approaches. There are systematic reviews about the safe use of ketamine as a component of multimodal analgesia in acute postoperative pain. 29,30 We implemented multimodal analgesia by administering nonsteroidal anti-inflammatory drugs during the postoperative period in addition to IV ketamine administration at the first hour and postoperative IV administration following the preoperative bolus dose. Patient satisfaction was also better in the ketamine-treated group. This result can be attributed to better pain scores.
There are certain limitations to this study. First, the side effects related to low-dose ketamine may not be accurately calculated in this sample size. Although patients were followed up for side effects during the hospital stay, they were not followed for long-term psychosomatic effects after discharge. Further studies are required for the long-term effects of ketamine. Secondly, patients were followed up for the first 24 hours after the operation. Moreover, the long-term outcomes of patients for opioid usage were not proven according to our study protocol. If long-term results were evaluated, different results could have been obtained. Lastly, hemodynamic parameters were used to decide on anesthesia management in terms of intraoperative consumption. If anesthesia and analgesic monitoring such as bispectral index and surgical pleth index were applied, differences in intraoperative consumption could occur.
In conclusion, we believe that perioperative low-dose ketamine administration is an effective and safe alternative component of multimodal analgesia for septorhinoplasty surgeries.
Footnotes
Authors’ Note
IA, MEA, and ECC contributed to conceptualization. IA, MSG, and ECC contributed to data curation. AA contributed to formal analysis. IA, MEA, and AA contributed to methodology. IA, MSG, and ECC contributed to project administration. AA contributed to visualization. IA and AA contributed to writing—original draft. IA, MEA, ECC, MSG, and AA contributed to writing—review and editing. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.