
Abstract
The objective of our study was to assess the relationship between postoperative opioid prescribing patterns and opioid consumption among patients who underwent septoplasty or rhinoplasty. A chart review of patients who underwent either septoplasty or rhinoplasty by 3 surgeons between July 2016 and June 2017 was performed, and pertinent clinical data were collected including the amount of narcotic pain medications prescribed. A telephone interview was then conducted to assess opioid usage and pain control regimen postoperatively. The number of opioid tablets prescribed and the number consumed were converted to total morphine milligram equivalent (MME) for uniform comparison. A total of 75 patients met the inclusion criteria, and 64 completed the telephone survey. Among these 64 patients, the mean (standard deviation [SD]) prescribed MME was 289.7 (101.3), and the mean (SD) consumed MME was 100.6 (109). Similarly, the mean (SD) number of opioid tablets prescribed was 42.4 (9.7), and the mean number of tablets consumed was 14.7 (16.3). Gender, procedure performed (septoplasty or rhinoplasty), use of Doyle splints, and surgeon were not associated with the amount of opioids prescribed or used. Subjective pain control was the only factor associated with an increase in opioid use (P = .0288). There was an overabundance of opioid pain medications prescribed compared to the amount consumed for pain control after septoplasty or rhinoplasty. Abuse of prescription opioids represents an important component of the nation’s opioid crisis. Surgeons must be cognizant of the problem and adjust prescribing practices accordingly.
Keywords
Introduction
The opioid epidemic continues to be rampant in the United States. In 2017, there were over 70 000 drug overdose deaths, with opioids involved in nearly 68% of these deaths. 1 Drug overdoses involving prescription opioids increased 5-fold from 1999 to 2017, being implicated in 35% of all opioid-related deaths. 1 In a 2016 article, the Surgeon General reported that over 2 million people in the United States were addicted to prescription opioids and over 12 million had misused the medications in 2015 alone. 2 A significant portion of prescribed narcotics are given in the acute postoperative period, and there is strong evidence in multiple surgical specialties that an overabundance of these medications is being prescribed for postoperative pain. 3 -7 It has been reported that 71% of opioid abusers obtain pills through methods of diversion—including receiving pills for free from family members or friends who had excess pills—making prescribed narcotics an important contributor to the opioid epidemic. 8,9
In recognition of the dangers imposed by prescription opioids, state and federal legislation have been implemented. Areas of focus primarily include education on pain management, prescription drug monitoring programs, and restrictions on prescribers. 10 -13 As frequent opioid prescribers, surgeons may be contributing to this opioid epidemic and therefore also have the opportunity to instigate change. In order to do so, we must better understand the scope of the problem following common surgical procedures. Sinonasal surgeries are some of the most common procedures performed by otolaryngologists, with the most recent estimates indicating as many as 500 000 per year. 14,15 This study compares the amount of prescribed opioids to the amount used for patients who underwent a septoplasty or rhinoplasty, seeking to help estimate a reasonable amount of narcotics to prescribe following nasal surgery.
Patients and Methods
The study was approved by institutional review board (IRB) of The Ohio State University prior to initiating any research. It was designed to assess the management of postoperative pain and opioid use following septoplasty with or without turbinate reduction or rhinoplasty with or without turbinate reduction. Patients were identified via chart review of a single tertiary medical center’s electronic medical record. The operative reports of 3 otolaryngologists were examined over a 12-month period. Included patients were at least 18 years old and underwent septoplasty or rhinoplasty between July 1, 2016, and June 30, 2017. Demographic information, operative details, and postoperative narcotic prescription information were recorded. Patients were excluded if they underwent concomitant procedures or had an existing opioid prescription for chronic pain. Of note, patients were included if inferior turbinate reduction and/or auricular cartilage graft was part of the procedure and however excluded if cartilage was harvested elsewhere. It should be noted that patients received local anesthetic (1% lidocaine with 1:100 000 epinephrine) at the site of incisions/dissection planes, but no nerve blocks were performed.
Patients who met the aforementioned inclusion criteria were contacted by telephone with a minimum of 3 separate phone call attempts made per patient. Phone calls were made during the month of July 2018. An IRB-approved telephone script was used for each conversation, and verbal consent was obtained prior to proceeding with the questionnaire portion of the call (Supplemental Material). Each patient was then asked a total of 9 questions related to postoperative pain control and opioid use. These questions asked details regarding the number of tablets taken, duration of opioid use, subjective pain control, the use of over-the-counter pain medications, opioid disposal, and whether prescribing fewer narcotic tablets would have been acceptable.
Using the Centers for Medicare & Medicaid Services’ opioid conversion table, 16 each patient’s prescribed and consumed total morphine milligram equivalent (MME) was calculated. We conducted bivariate analysis to evaluate for mean MME differences based on demographic data and clinical variables. A Student 2-tailed t test was used to detect differences between covariates such as surgical procedure (septoplasty or rhinoplasty), use of Doyle splints, subjective pain control, and use of supplemental over-the-counter pain medications. To detect significant differences in prescribing patterns among the 3 surgeons, a 1-way analysis of variance was used. A P value of <.05 was considered significant.
Results
According to operative logs, we identified 80 adult patients who underwent septoplasty or rhinoplasty in the 1-year time period. Following the chart review, 3 patients were excluded due to concomitant procedures being performed, 1 patient was ineligible due to a preexisting pain contract for sickle cell disease, and 1 patient had significant pain related to a postoperative complication (a septal hematoma that required a return to the operating room). A total of 75 patients met all inclusion criteria. Of these, 11 were unreachable by phone, leaving 64 patients who completed the telephone-based questionnaire (Figure 1).
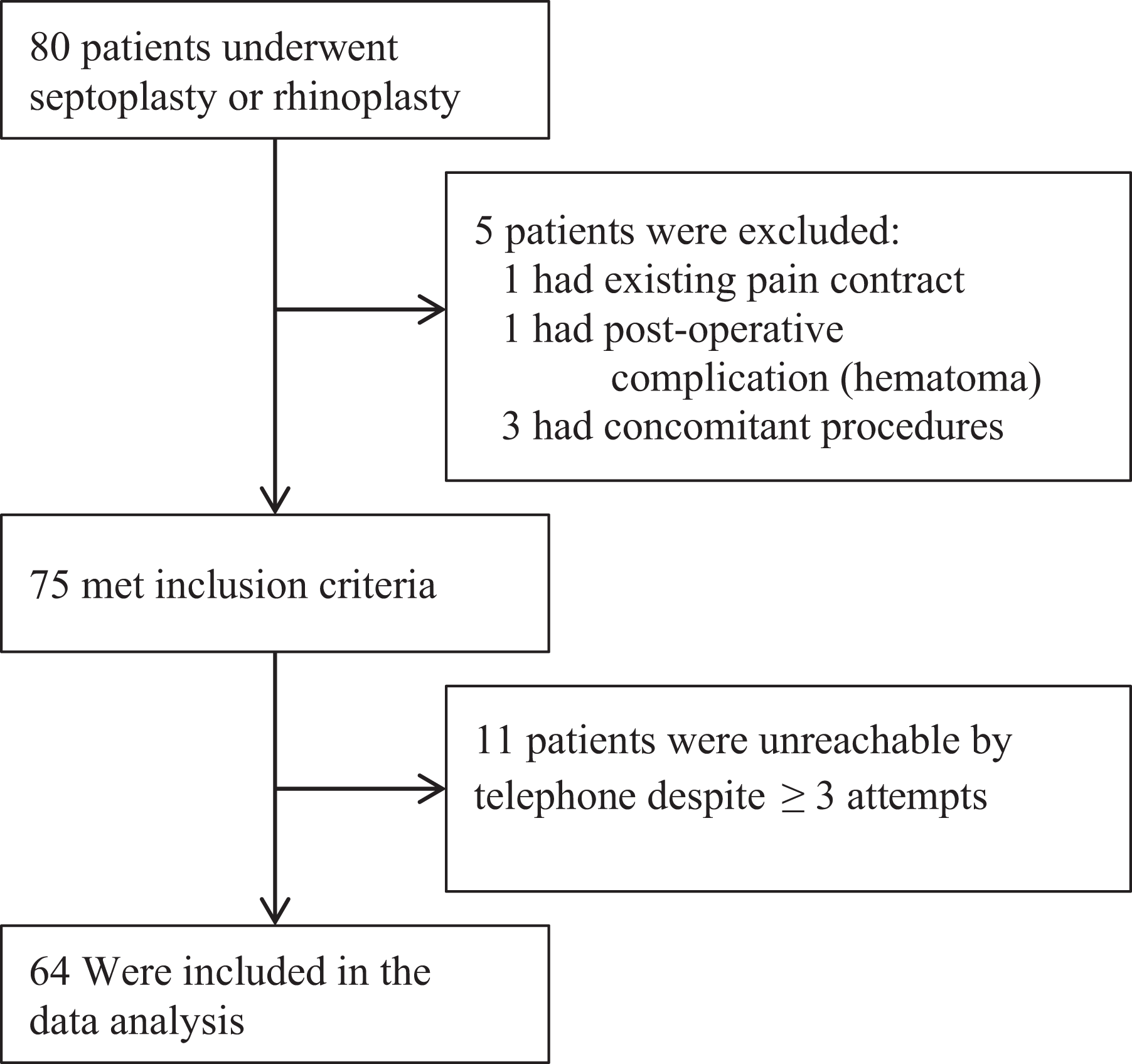
Summary of patients included in data analysis.
Of the 64 patients, 39 were males and 25 were females. The mean age was 44.4 ± 13.2 years (range, 22-74 years). Among all patients, the mean MME prescribed was 289.7 ± 101.3 and the mean MME consumed was 100.6 ± 109 MME. All but 1 of the 64 patients received a prescription for an opioid. Of the remaining 63 individuals, 43 (68.3%) received oxycodone or oxycodone/acetaminophen, 18 (28.6%) received hydrocodone/acetaminophen, 1 (1.6%) received tramadol, and 1 (1.6%) received hydromorphone tablets due to a medication allergy. There were 6 (9.4%) patients who denied significant postoperative pain and thus never filled their opioid prescription and 2 patients (3.1%) required refills despite being prescribed 40 tablets. The mean number of tablets prescribed, among all prescriptions, was 42.4 ± 9.7 (range, 20-60), and the mean number of tablets consumed was 14.7 ± 16.3 (range, 0-50).
A summary of MME prescribed and consumed, based on demographic data and various other clinical variables, can be found in Table 1. Bivariate analysis was performed, and there was no significant difference in mean MME—prescribed or consumed—based on gender (P = .637 and .657, respectively). Rhinoplasty compared to septoplasty did not reveal a significant difference in MME prescribed (P = .203). There was a higher MME use with rhinoplasty; however, findings were not statistically significant (P = .0646). Doyle splint use also did not show a difference in mean MME use (P = .278) nor did the use of additional over-the-counter pain medications (P = .226). The only variable to show a significant difference in narcotic usage was subjective postoperative pain control. For the 5 patients who did not achieve adequate pain control, 4 of the 5 underwent a septoplasty with turbinate reduction and 1 underwent a functional rhinoplasty with turbinate reduction for nasal obstruction. The mean MME used among these 5 patients was more than double that of those patients with adequate subjective pain control (91.5 ± 103.8 vs 202.5 ± 134.2, P = .0288). There was no significant difference in the mean MME prescribed or mean MME consumed, when comparing the 3 different surgeons (P = .526 and .554, respectively).
Summary of MME Prescribed and Used.
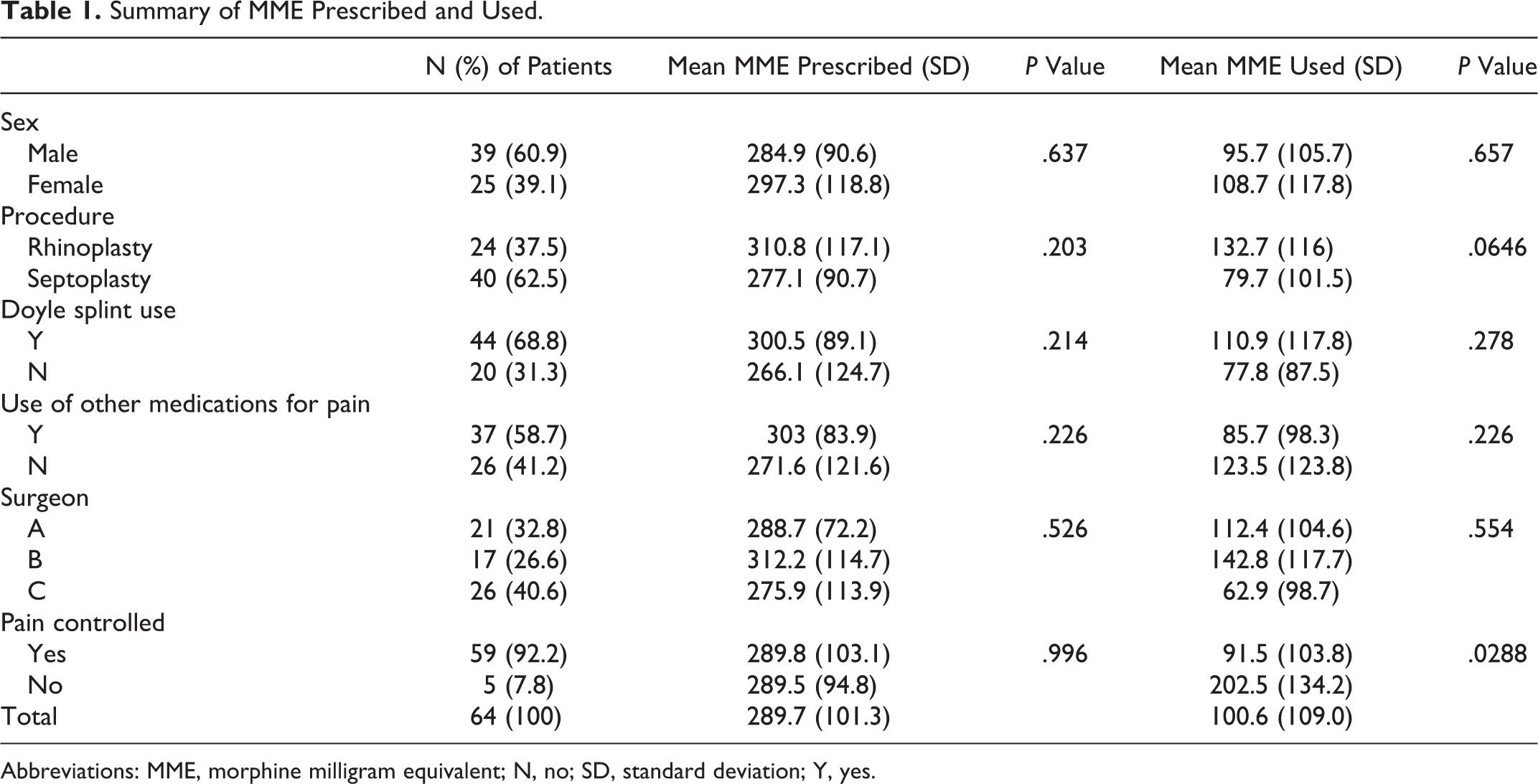
Abbreviations: MME, morphine milligram equivalent; N, no; SD, standard deviation; Y, yes.
Discussion
The late 1990s and early 2000s brought about a concerted effort in the medical community to treat pain more aggressively. Some pushed for pain to be recorded as a vital sign when evaluating patients, and the Joint Commission published a report in 1999 that recommended more aggressive treatment of patient pain. 17 Prescription opioids were viewed as a key part of the solution to this “pain epidemic,” and physician opioid prescriptions began to increase significantly. 18 While the greatest amount of opioids are being prescribed by chronic pain specialists, surgeons have the second highest rate of opioid prescribing (37% of all prescriptions). 17 Despite the fact that surgeons typically provide only short-term prescriptions, there is a significant risk for chronic opioid use that may not be fully appreciated. A 2017 report showed that patients who received a 5-day supply of opioid medication have a 10% chance of using opioids 1 year later. 19 There is no denying risks are associated with all opioid prescriptions; therefore, it is our duty as otolaryngologists to assess personal prescribing patterns and accept some responsibility for our role in the current national crisis.
Our study examines the prescribing habits at our institution for acute postoperative pain after septoplasty and rhinoplasty, confirming the overprescribing trend seen in many other surgical specialties. 3 -6,20 -22 On average, we prescribed 3 times the amount of narcotics needed with a mean of 42.4 ± 9.7 tablets prescribed and a mean of only 14.7 ± 16.3 tablets consumed. Interestingly, several recent studies have found very similar results, concluding that after sinonasal surgery 15 opioid tablets is sufficient for pain control in the vast majority of patients. 23 -25 We found that pain was subjectively achieved in the majority of respondents (93.8%); however, our data show a significant amount of individual variability. For example, the range of opioid tablets consumed in the postoperative course ranged from 0 to 50 tablets, with 7 (10.9%) patients not even filling an opioid prescription. Of those who could recall, only 6 (10.2%) of 59 patients required narcotics beyond postoperative day 7. On the other hand, 14 (21.9%) of 64 patients used 30 or more narcotic tablets. This illustrates the dilemma we as prescribers face. The inherently subjective nature of pain leads to difficulties in prescribing the appropriate amount of narcotics. Narcotic prescriptions directed toward the minority that experience significant postoperative pain inevitably leads to an overall excess.
A recent national survey clearly demonstrated significant variations in opioid-prescribing patterns among otolaryngologists. 26 This variability therefore often means excess pills are being prescribed. Multiple groups have now begun to establish multimodal analgesia protocols as a means to reduce overall opioid use. 23,24 Nguyen et al performed a systematic review of perioperative analgesic opioid alternatives and concluded that the literature supports the use of nonsteroidal anti-inflammatory drugs (NSAIDs), gabapentin, local anesthetics, and α-agonists following septoplasty and septorhinoplasty. 27 In many cases, these protocols propose that few or no opioids are prescribed, instead relying primarily on acetaminophen and/or NSAIDs. Nguyen et al recently published results from a prospective randomized trial in which patients underwent outpatient otolaryngology surgery and were randomly chosen to receive ibuprofen or an opioid medication as their primary analgesic. 28 The results showed an overall low usage of opioids as well as a significant reduction in opioid consumption for the ibuprofen group (2.04 tablets compared to 4.86 tablets in the opioid group).
Proper disposal of unused narcotics revealed another disturbing trend. Over 40% of our respondents (42.2%) reported not yet disposing of unused pills, and an additional 18.8% were unable to recall what came of their unused narcotics. Several patients admitted to saving them for future use, and some had already taken the pills for unrelated pain. Based on information from the 2016 study by Kennedy-Hendricks et al, 20.7% of patients reported having shared opioid medications with another person. 29 This trend of surgeons overprescribing narcotics only further increases the risk of opioid abusers obtaining pills through diversion. The US Food and Drug Administration has detailed proper methods for safe medication disposal, and it is a prescriber’s responsibility to ensure this information is provided to patients. 30
There are several limitations to our study. First, recall bias may have limited the accuracy and reliability of our results. At the time of the telephone-based questionnaire, some patients were asked to remember postoperative details from 1 year prior. Pain control as well as estimates for the exact number of opioid tablets consumed may have been inaccurate. Another concern is the complexity of these procedures and the variability in surgical technique that may affect pain. That being said, our findings demonstrated a substantial difference between the amount of opioids prescribed and the amount consumed, regardless of surgeon, procedure, or use of Doyle splints.
As surgeons, we obviously strive to achieve excellent pain management but now must consider the consequences of overprescribing opioids. In accordance with our study’s findings as well as a review of recent publications, 23 -25 we believe that 15 oxycodone 5 mg tablets (112.5 MME) would provide more than adequate pain control for the vast majority of septoplasty and rhinoplasty patients. Coupled with this reduction in prescribed opioids, we encourage surgeons to increase their preoperative counseling and patient education regarding postoperative pain expectations, pain control with acetaminophen and/or NSAIDs, and proper disposal of unused narcotics. For those patients who may ultimately require more than the initial number of prescribed opioid tablets, the ability to now electronically prescribe opioid medications in many states minimizes the concern for periods of prolonged uncontrolled pain in postoperative patients. Our otolaryngology community must continue to focus on modifying our prescribing patterns and reducing opioid prescriptions.
Supplemental Materials
Supplemental Material, Phone_script_with_consent_and_HIPAA_elements_(1) - Postoperative Prescriptions and Corresponding Opioid Consumption After Septoplasty or Rhinoplasty
Supplemental Material, Phone_script_with_consent_and_HIPAA_elements_(1) for Postoperative Prescriptions and Corresponding Opioid Consumption After Septoplasty or Rhinoplasty by Alexander N. Rock, Kenneth Akakpo, Corey Cheresnick, Benjamin M. Zmistowksi, Garth F. Essig, Eugene Chio and Stephen Nogan in Ear, Nose & Throat Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Materials
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.