
Abstract
Otic capsule dehiscences create a pathological third window in the inner ear that results in a dissipation of the acoustic energy consequent to the lowered impedance. Superior semicircular canal dehiscence (SSCD) was identified by Minor et al in 1998 as a syndrome leading to vertigo and inner ear conductive hearing loss. The authors also reported the relation between the dehiscence and pressure- or sound-induced vertigo (Tullio’s phenomenon). Prevalence rates of SSCD in anatomical studies range from 0.4% to 0.7% with a majority of patients being asymptomatic. The observed association with other temporal bone dehiscences, as well as the propensity toward a bilateral or contralateral “near dehiscence,” raises the question of whether a specific local bone demineralization or systemic mechanisms could be considered. The present report regard a case of a patient with a previous episode of meningitis, with a concomitant bilateral SSCD and tegmen tympani dehiscence from the side of meningitis. The patient was affected by dizziness, left moderate conductive hearing loss, and pressure/sound-induced vertigo. Because of disabling vestibular symptoms, the patient underwent surgical treatment. A middle cranial fossa approach allowed to reach both dehiscences on the symptomatic side, where bone wax and fascia were used for repair. At 6 months from the procedure, hearing was preserved, and the vestibular symptoms disappeared.
Introduction
The membranous labyrinth is located inside a hard-bony structure called the otic capsule (OC) that communicates with the middle ear cavity via 2 membranes (the round and oval windows) allowing fluid-mediated sound transduction, that is, the beginning of the hearing mechanism. The oval and round windows represent the 2 main physiological weak and compressible areas of the OC that alternate in depressing and bulging for this purpose. Other channels, including the cochlear and vestibular aqueducts and the foramina for vessels and nerves, represent additional windows that play scarce or no roles in auditory function. Abnormal communications of the OC may be also due to spontaneous and congenital dehiscences that related to defects during the embryological development. Among them, in the enlarged vestibular aqueduct syndrome part of the acoustic energy is lost since it is dumped due to shifting to the intracranial space. 1 Genetic conditions such as X-linked stapes gusher due to DFN3 locus mutations and Paget’s syndrome may also generate a third window effect. Moreover, defects during embryological development may result either in a complete dehiscence of the bone overlying the tegmen and/or the superior semicircular canal (SSC), or just in its thinning that becomes symptomatic in concomitance with additional factors (trauma, osteopenia, osteoporosis, sudden increase in intracranial pressure, and obesity).2-7 Chronic otitis media, cholesteatoma, temporal bone fractures or previous middle ear or skull base surgery are also involved for dehiscence occurrence. 8
Superior semicircular canal dehiscence (SSCD) was identified by Minor et al in 1998 9 as a syndrome of vertigo and oscillopsia. The prevalence rates in cadaveric temporal bone studies range from 0.4% to 0.7%10,11 and from 2% to 13% in computed tomography (CT) studies12,13 with the majority of patients being asymptomatic. Symptomatic patients will usually present with only cochlear, only vestibular or vestibulocochlear signs and symptoms. Patients mainly complain of noise or pressure-induced vertigo, hearing loss, dizziness, autophony, and tinnitus. When there is clinical suspicion, a confirmed diagnosis can only be achieved with high-resolution computed tomography (HRCT). According to Belden et al, the CT positive predictive value for detecting SSCD, using ultra-high resolution and reconstruction in the SC plan, is 93% with a collimation of 0.5 mm. 14 The diagnosis of SSCD is therefore made by combining clinical and radiological findings. Dehiscences of the posterior or lateral semicircular canals are less common. 15 Stimmer et al found dehiscence rates of 12% and 4.6% for the posterior and lateral semicircular canals, respectively, among 125 SCD. 16 According to Ahren and Thoulin and Lang, isolated tegmen defects occur in approximately 20% of temporal bones.17,18
The association between SSCD and other temporal bone defects has been widely described in the literature. The most common association is the one involving the dehiscence of SSC and tegmen tympani. Minor was the first author to have noticed such an association. 19 In 2016, Rodrigo et al described the common embryological origin of both structures that might explain the high rate of associated dehiscence. 20 Suryanarayanan and Lesser reported 3 cases of multiple tegmen defects forming a characteristic “honeycomb” pattern in association with SSCD. 21 Manzari presented the case of a 38-year-old male with bilateral posterior semicircular canal dehiscence associated with SSCD and typical right-sided vestibular and cochlear symptoms. 22 In 2018, Whyte et al studied possible associations between dehiscence in the superior and posterior semicircular canals, and the association of both dehiscences with other alterations in the temporal bone. They reported 28 cases of associations between SSC and tegmen tympani dehiscence and 3 cases that showed multiple temporal bone dehiscences associated with SSCD. 23 Multiple associated dehiscences without radiological evidence have also been recently described as otic capsule dehiscence syndrome. 24 In the present report, a case of a man suffering from bilateral SSCD and a unilateral tegmen tympani defect is presented, providing insights into the clinical course and surgical resolution.
Case Presentation
A 43-year-old man was referred to our hospital with an 8-months history of objective, sound/pressure elicited recurring vertigo, left tinnitus, and hearing loss. One year before he suffered from Streptococcus pneumoniae meningitis and was successfully treated with vancomycin for 20 days. Under otomicroscopy, a normal right tympanic membrane was found while in the left ear an attic retraction pocket was observed, with a pulsatile mass behind it. Pure tone audiometry showed normal hearing levels in the right ear and moderate conductive hearing loss in the left ear. Stapedial reflexes were present and were in the normal range, while tympanometry was type “A” bilaterally, with peak compliance value of 1 mL on the right side and 0.7 mL on the left side. Tullio’s phenomenon was found to be positive on the left side.
A HRCT of the temporal bone revealed bilateral SSC dehiscence, wider on left side; dehiscence of the tegmen tympani and mastoid tegmen on the left side and thinning on the right side; a meningocele imprinting the malleus head and the body of the incus on the left side, without signs of ossicle erosion (Figure 1).
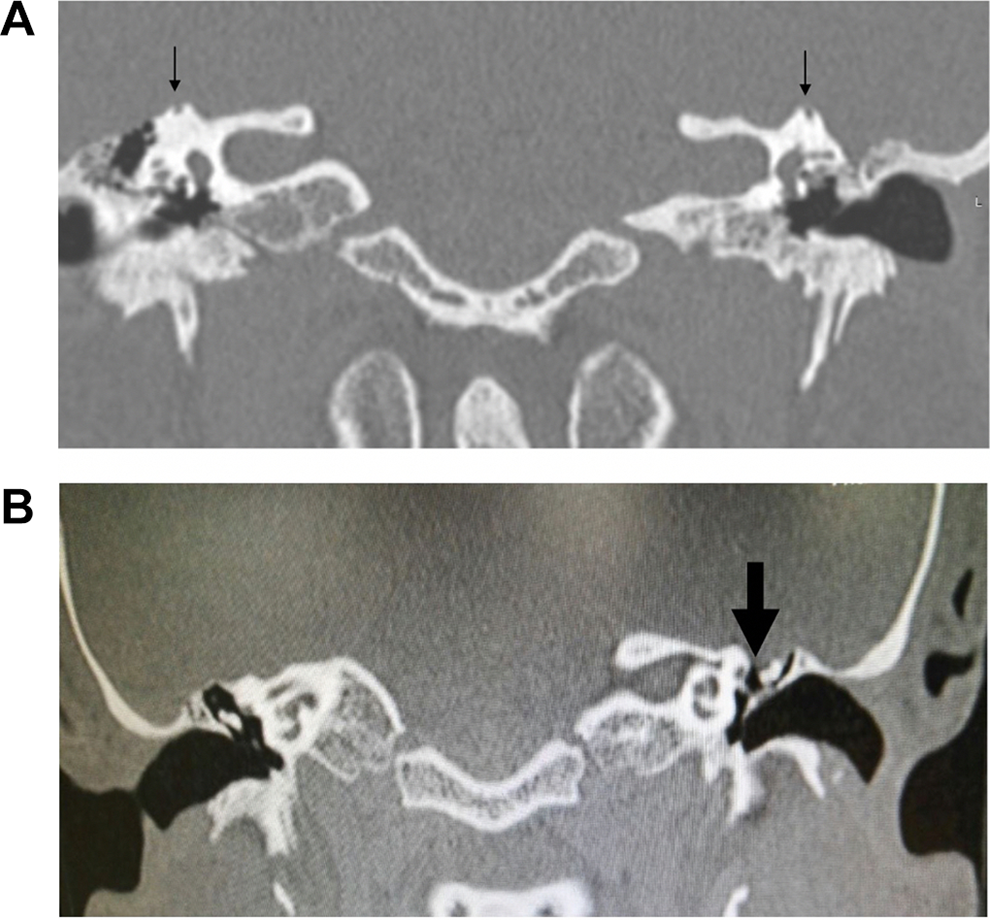
A, Temporal bone high resolution computed tomography (CT). Coronal view showing bilateral superior semicircular canal dehiscence (black arrows). B, Temporal bones high resolution CT. Coronal view showing dehiscence of tegmen tympani on left side (dotted arrow) and thinning on right side; left side meningocele; no aspects of ossicles erosion.
A surgical approach was planned through middle cranial fossa to repair both bony dehiscences (Figure 2). The hair around the area of the planned incision was shaved and the area infiltrated with 2% carbocaine with 1:100000 adrenaline. A piece of temporalis fascia was harvested for later use. Then the area of the craniotomy was exposed, and craniotomy was performed using a 3 mm cutting burr. The bone flap was carefully elevated away from the dura and preserved in saline for later use. A hemostatic microfibrillar absorbable sponge (Equitamp ®, Ergon Sutramed s.r.l., Magliano dei Marsi [Aq], Italy) was applied under the bony edges of the craniotomy. A small temporal lobe meningocele was then identified and gently elevated allowing visualization of the eroded area. After detection of the exit of the greater superficial petrosal nerve, the dehiscence of the SSC was identified posteriorly. Both dehiscences were then repaired with bone wax and autologous fascia and stabilized with fibrin glue (Tisseel ®, Baxter, Wien, Austria). Owing to the selected approach, it was not possible to get evidence of the condition of the ossicular chain that was however freed from the brain contact. A non-absorbable, heterologous dura (Neuropatch ®, BBraun, Milan, Italy) was then placed covering the repaired areas. Closure was achieved by anchoring the previously harvested bone flap in place using titanium plates. The temporal muscle was repositioned with absorbable sutures, and the skin closed with nylon sutures. A compressive dressing was applied. No postoperative complications were experienced by the patient. At otomicroscopy, pulsation at the level of the left attic eardrum had disappeared, as previously described. 10 At the 2 years follow–up, the patient was still devoid of further episodes of imbalance, vertigo or meningitis, with no significant hearing changes.
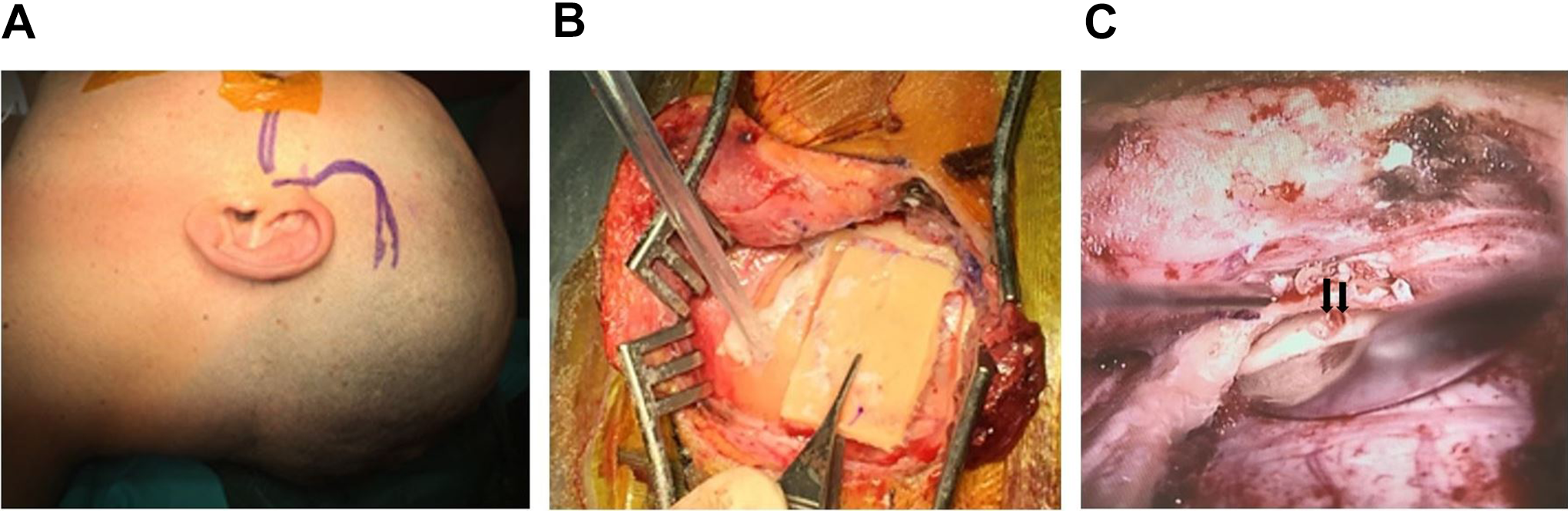
A, Planned incision for middle cranial fossa approach is drawn after hair being shaved. B, A 3 × 4 cm craniotomy is performed, and the bone flap is elevated. C, Bony dehiscences are individuated via a gentle depression of the temporal lobe (black arrows).
Discussion
Spontaneous dehiscences affecting the tegmen tympani and superior semicircular canal are considered the most common association in temporal bone defects, with an incidence of 36.4%. 11 In 2012, El Hadi et al described that spontaneous tegmen defects had a 56.5% incidence of associated SSC dehiscence, suggesting that they may form a common disorder. 25 Nadaraja et al found a 76% association and reported a 10.2 times greater probability of tegmen dehiscence in patients affected by spontaneous SSC dehiscence. 26 Recently, Whyte et al reported a 39.4% association of both these defects. 23 Such a strong relationship has been explained by the common embryological origin of both structures. 20
From a clinical point of view, this association may be revealed by isolated vestibular or auditory symptoms, or by both or neither of them. According to an analysis by Wackym, the most common symptoms in patients are disequilibrium, headache, dizziness, tinnitus, vertigo, hearing loss, and autophony. 24 Signs such as Tullio’s phenomenon (sound induced vertigo) and Hennebert’s sign (pressure induced nystagmus) are also characteristic. Another clinical feature often found in SSCD is a conductive hearing loss on pure tone audiometry, usually involving the mid-low frequencies. The SSCD creates a pathological third mobile window in the inner ear that results in a dissipation of the acoustic energy because of the consequent lowered impedance. 2
Defects in the tegmen tympani create a communication between the middle ear and the middle cranial fossa exposing the subarachnoid space to potential aggression by pathological agents coming from the middle ear. Sanna et al. described a 27.3% incidence of meningitis as first manifestation in spontaneous tegmen defects, 27 while Bruschini et al found a 73.1% incidence of bone defects in otogenic meningitis. 28 Furthermore, a defective middle fossa floor can create a pathway through which meningeal and/or cerebral tissue may herniate, potentially resulting in worse complications. 28 Surgical treatment is mandatory when life-threatening complications are experienced and is also proposed to symptomatic patients with debilitating symptoms (vertigo, hearing loss, dizziness, etc). Wackym et al found a high rate of psycho-behavioral comorbidities that can mask the symptoms caused by the dehiscence itself especially in pediatric and head-trauma populations. 29
Two main surgical approaches may be applied under these circumstances: one through a middle fossa craniotomy approach and the other via a transmastoid route. 30 In the present case, the former approach was selected in view of the direct resurfacing of the bony areas where the defects were found. 31 The reliability of this approach also lies in the more likely preservation of the SC function, against a 10% risk of pancanal loss of function reported with the transmastoid plugging procedure. 12 In fact, the patient in the present report showed no signs of canal function reduction and achieved complete regression of vestibular symptoms, with an overall high satisfaction rate. One major drawback of the selected surgical approach is the impossibility to control the conditions of the ossicular chain. In fact, the post-operative persistence of the conductive hearing loss would prompt planning an exploratory tympanotomy at a later stage.
Conclusions
Spontaneous temporal bone dehiscences represent a rare event, even more so in association with other temporal bone defects. Affected patients usually have debilitating symptoms and, especially in those with a previous history of meningitis, a surgical protocol is strongly recommended.
The definitive diagnosis always requires HRCT. The middle cranial fossa approach may be chosen for a wider and more accurate exposure with the repair of defects.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.