
Abstract
Background:
Tuberculosis (TB) of posterior pharyngeal wall (PPW), either primary or secondary, is extremely rare and can mimic malignancy in elderly patients.
Case Report:
A 36-year-old female patient presented with complains of nonhealing ulcer at the back of her throat for 4 months. On examination, there was an ulceroproliferative growth covered with slough over PPW. Positron emission tomography scan showed uptake in PPW. There was no uptake in any other part of body. A biopsy from PPW lesion showed epithelioid cell granulomas with Langhans type giant cells. Auramine-rhodamine staining showed few beaded bacilli consistent with TB.
Conclusion:
Tuberculosis of PPW is an extremely uncommon entity and can mimic malignancy. It should be kept as one of the differential diagnosis as it can be cured solely by giving anti-tubercular therapy.
Introduction
Primary tuberculosis (TB) of oropharynx is an uncommon entity comprising of 0.05% to 5% of all cases of TB. Tonsils are the most affected site in oropharynx followed by soft palate. Tuberculosis of posterior pharyngeal wall (either primary or secondary) is extremely rare and can pose a diagnostic dilemma especially in elderly patients as it can mimic malignancy. We present a case of 36-year-old female who was diagnosed with TB of posterior pharyngeal wall.
Case Report
A 36-year-old female presented to our outpatient clinic with complains of a nonhealing ulcer at back of her throat for 4 months. There was no history of pain during swallowing, bleeding from ulcer, loss of appetite, recent weight loss, chronic cough, or fever. She did not have any addictions or history of any TB contact. On examination, there was around 3 × 3 cm ulceroproliferative growth covered with slough over posterior pharyngeal wall (Figure 1). Rest of the subsites of oropharynx were normal. There were no clinically palpable lymph nodes in neck. There was an indurated plaque like lesion involving left infraorbital region near nasal dorsum. 18F-FDG-PET/CT (fluorodeoxyglucose-positron emission tomography/computed tomography) scan was done to rule out any other primary lesion. It showed subcentimetric lymph nodes in submandibular region along with uptake in oropharyngeal wall (Figure 2). No other lesion was noted in rest of the body. Blood parameters including complete blood count, liver and kidney function tests were normal. Chest X-ray did not show any abnormality and patient was seronegative for human immunodeficiency virus (HIV). A biopsy was taken from posterior pharyngeal wall lesion which showed epithelioid cell granulomas with Langhans type giant cells. Auramine-rhodamine staining showed few beaded bacilli consistent with TB. Biopsy from infraorbital lesion also showed features consistent with TB. The patient responded well to the antitubercular therapy.

An ulceroproliferative growth involving posterior pharyngeal wall.
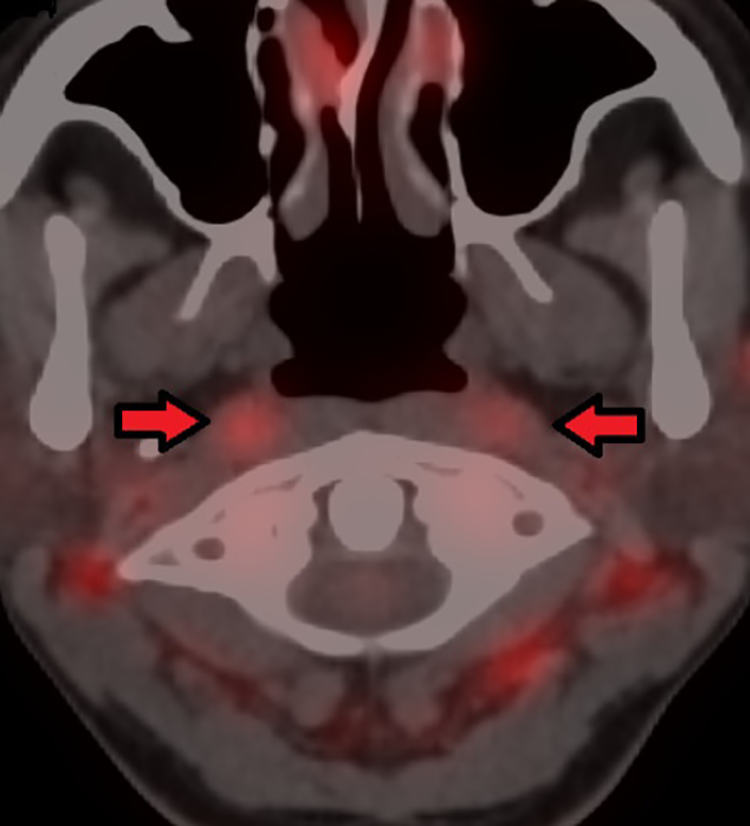
Fused PET-CT images with increased FDG uptake in the oropharyngeal wall.
Discussion
Extrapulmonary tuberculosis (EPTB) accounts for 15% to 20% of all cases of TB in immunocompetent patient while the burden may rise to 50% in immunocompromised patients like in those infected with HIV. 1 The most common site for EPTB are lymph nodes. 2
Tuberculosis of oral cavity or oropharynx is unusual because of phagocytic activity of saprophytes present in saliva which may inhibit the growth and multiplication of mycobacterium tuberculosis bacilli. Any breech in the oral mucosa due to irritation or inflammation, dental extraction, poor dental hygiene, and leucoplakia can predispose to TB. But even if there is no breach in mucosa, mycobacterium tuberculosis cross mucosal barriers by endocytosis within mucosal lymphoepithelial sites such as oropharyngeal and nasopharyngeal tonsils and Peyer’s patches. 3
Primary TB of oropharynx comprises of 0.05% to 5% of all cases of TB. The most common subsite in oral cavity is tongue while in oropharynx it is tonsils followed by soft palate. 4 Secondary TB of oropharynx can occur due to infected secretions from pulmonary TB. 5 Tuberculosis of posterior pharyngeal wall (either primary or secondary) is extremely rare. Patients can present with sore throat, globus sensation, dysphagia, or odynophagia. The examination of oropharynx and posterior pharyngeal wall may show an ulcero-profilerative growth which may bleed on touch.3,4,6. 7 It can also present as submucosal bulge clinically as well as radiologically. 6 All these features can mimic malignancy in an elderly patient and a high index of suspicion is required for diagnosis. Radiological evaluation in the form of computed tomography and magnetic resonance imaging can help in seeing the extent of lesion. Fluorodeoxyglucose-positron emission tomography (FDG PET-CT) imaging can show uptake in the tubercular lesions and help in determining the disseminated sites. 8 . 9 Definitive diagnosis can only be made by biopsy which shows caseating epithelioid cell granulomas with Langhans giant cells. Special stains like Zeihl-Neelsan and Auramine-rhodamine can be used to identify acid-fast bacilli. The treatment is solely anti-tubercular therapy.
Conclusion
Tuberculosis of oropharynx and particularly posterior pharyngeal wall is an extremely uncommon entity. Its clinical symptoms and signs can mimic malignancy. Fluorodeoxyglucose PET scan may be done to see the primary lesion or to rule out disseminated infection. A high degree of clinical suspicion is required for diagnosis and definitive diagnosis is by biopsy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.