
Abstract
Introduction:
Leukoplakia is a precancerous lesion considered to be within the spectrum of histopathological results from parakeratosis, through stages of dysplasia to invasive cancer. Narrow band imaging (NBI) endoscopy has been introduced to improve early diagnosis of benign and malignant laryngeal lesions. The aim of this literature review was to evaluate the accuracy of preoperative evaluation of vocal fold leukoplakia with NBI endoscopy in comparison with histology.
Methods:
A systematic review of the literature was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines, using 3 different databases: PubMed, Embase, and Scopus. The included articles in the systematic review were identified combining each of the following terms: “narrow band imaging” OR “NBI,” [AND] with each of these terms: “laryngeal leukoplakia,” OR “vocal fold leukoplakia,” OR “vocal cord leukoplakia.”
Results:
The articles that fully met the inclusion criteria were 5 case series, conducted between January 2010 and February 2018, and published between 2017 and 2019. The selected articles included 312 patients (86% males and 14% females), affected by 382 vocal cord leukoplakia, evaluated with NBI endoscopy and that underwent surgical microlaryngoscopy with biopsy. Based on the studies included in the review, accuracy of NBI in predicting malignancy within leukoplakia ranged from 81% to 97.8%, demonstrating to be an accurate method to predict the risk of malignant transformation of vocal fold leukoplakia.
Conclusion:
Narrow band imaging can help otolaryngologists in the decision-making process on the necessity to perform a biopsy and transoral surgery or long-term follow-up. Larger studies are necessary to confirm the high association of NBI evaluation of the epithelium surrounding the leukoplakia with the histological diagnosis.
Introduction
“Leukoplakia,” the Greek term for “white plaque,” is a generic medical term indicating the occurrence of keratin on the epithelial surface.1,2 Leukoplakia is a precancerous lesion considered to be within the range of histopathological results from parakeratosis, through stages of dysplasia to invasive cancer. 3 Isenberg et al, 1 in their systematic review on of 2188 biopsies of leukoplakia, showed that no dysplasia was identified in 53.6% of cases, mild or moderate dysplasia in 33.5%, and high-grade dysplasia and carcinoma in situ in 15.2% of cases.
Preoperative examinations using white light imaging (WLI) endoscopy may not agree with postoperative biopsy results, thus leading to overtreatment or undertreatment in some cases. Consequently, the main recommendation for patients with leukoplakia is excisional biopsy and histopathological diagnosis.
Some recent studies have demonstrated that narrow band imaging (NBI) endoscopy can improve early diagnosis of benign and malignant laryngeal lesions4-6 and the optimal definition of the intraoperative surgical margins. 7
For these reasons, NBI endoscopy has been extensively applied in the diagnosis of laryngeal diseases.7,8 Narrow band imaging observes mucosal vascularization, allowing detection of superficial carcinomas and premalignant lesions by improving the contrast of the mucosal epithelium and submucosal vessel loops. However, leukoplakias may have the “umbrella effect,” in which the submucosal vascular pattern is hidden under the hyperkeratotic plaque and not directly visible. 9 In the last year, to overcome the umbrella effect, the NBI was used to classify submucosal microvascular pattern surrounding the plaque.
The aim of this review was to determine the accuracy of preoperative evaluation of vocal fold leukoplakia with NBI in comparison with histology, with a special focus on the role of the vascular changes around the plaque and the possible connection between NBI features and pathology diagnosis.
Materials and Methods
Search Strategy
A systematic review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. 10 Authors conducted a literature search on articles published until June 2020 using 3 different databases: PubMed, Embase, and Scopus.
The included articles in the systematic review were identified combining each of the following terms: “narrow band imaging” OR “NBI,” [AND] with each of these terms: “laryngeal leukoplakia,” OR “vocal fold leukoplakia,” OR “vocal cord leukoplakia.”
The inclusion criteria were: (1) patients with vocal cord leukoplakia evaluated with NBI endoscopy that underwent direct laryngoscopy with biopsy; (2) studies reporting complete data on the diagnostic sensibility of the NBI; and (3) abstracts available in English.
The exclusion criteria were: (1) studies with less than 10 patients and (2) non-original studies.
Title and abstract were watchfully examined independently by authors according to the inclusion and exclusion criteria, and the duplicates were removed. The full text of the included studies was reviewed with extraction of following data: (1) number of patients, (2) accuracy, (3) sensibility, and (4) specificity of NBI.
Results
Search Results
The search algorithm is outlined in Figure 1.
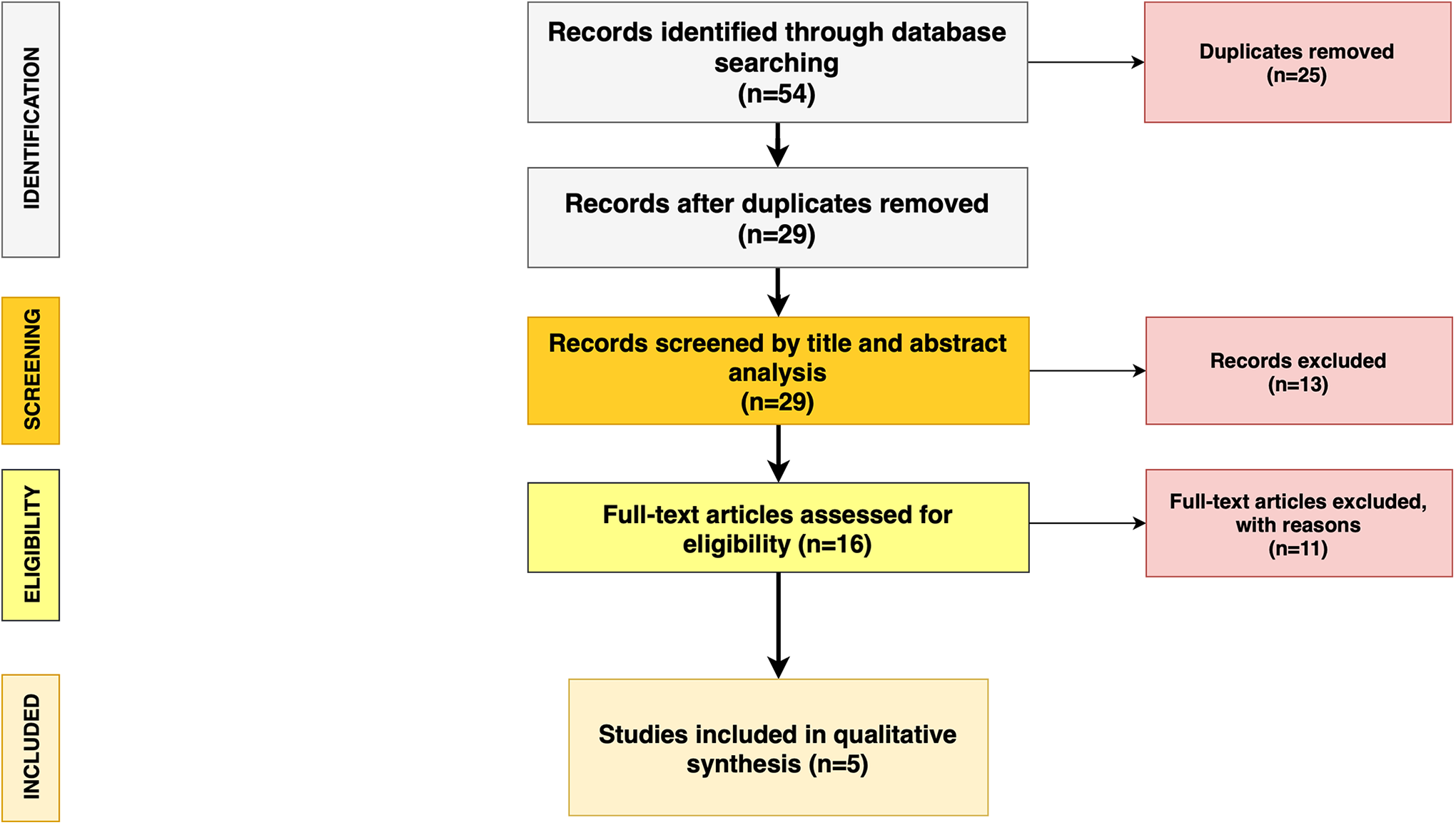
Preferred Reporting Items for Systematic Reviews and Meta-Analyses diagram followed in this review. The diagram shows the information flow through the different phases of the review and illustrates the number of records that were identified and included.
The initial search recognized 54 studies on PubMed, Embase, and Scopus. The removal of duplicates identified 29 publications. All the 29 papers were screened in title and abstract and 16 manuscripts were reviewed in full text. Five studies met the inclusion criteria.
Data Synthesis and Analysis
The data from each study were transcribed in tabular form (Tables 1 and 2).
Summary of Clinical Characteristics of 5 Studies Included in the Review.

Vocal Cord Leucoplakia Evaluated With Narrow Band Imaging Endoscopy and Direct Laryngoscopy With Biopsy.
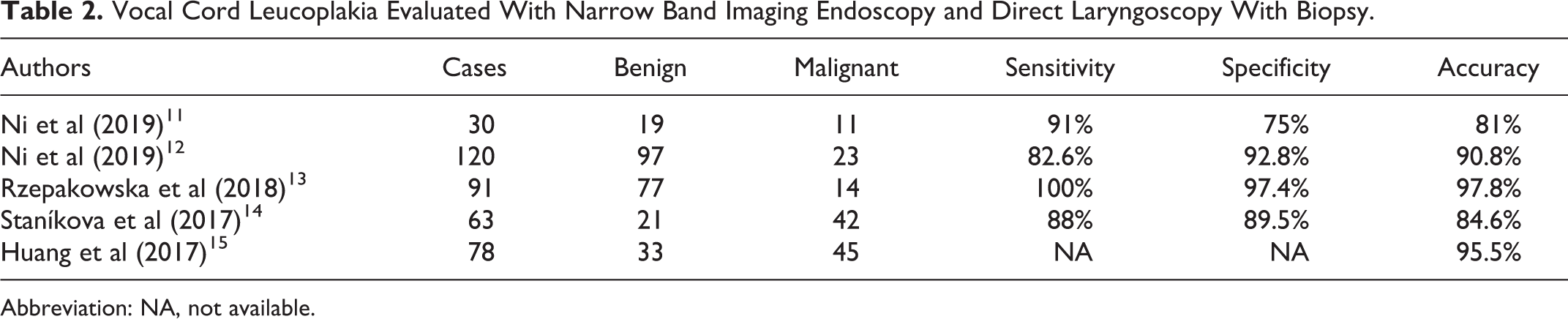
Abbreviation: NA, not available.
The articles that fully met the inclusion criteria were 5 case series, conducted between January 2010 and February 2018, and published between 2017 and 2019. The selected articles included 312 patients (86% males and 14% females), affected by 382 vocal cord leukoplakia, evaluated with NBI endoscopy and underwent direct laryngoscopy with biopsy.
Based on the studies included in the review, accuracy of NBI in predicting malignancy within leukoplakia ranged from 81% to 97.8% (Table 2), demonstrating to be an accurate method to predict the risk of malignant transformation of vocal fold leukoplakia.
Discussion
Laryngeal leukoplakia is a generic medical expression indicating a white patch or plaque on the vocal fold mucosa; the term is not specific for histological diagnosis. 1 In the last year, the incidence of vocal fold leukoplakia has increased. 16
Vocal fold leukoplakia is associated to alcohol abuse, tobacco smoking, viral infection, voice misuse, and laryngopharyngeal reflux.13,17
Leukoplakia comprises several histological features: benign, premalignant, and malignant lesions. 18 Benign leukoplakia is usually a limited and often reversible lesion, which can be controlled with follow-up or removed with transoral microsurgery. Differently, malignant leukoplakia lesions require immediate biopsy and, in some cases, radiotherapy or transoral laser surgery to prevent recurrence.3,19-21
Flexible or 70° rigid WLI endoscopy is the most common examination for the diagnosis of vocal cord leukoplakia, showing the main signs of malignant lesions: color, size, surface texture, hyperemia, thickness, edema, and symmetry of leukoplakia. 22 The independent factors associated with the risk of malignancy are nonhomogeneous lesion texture and existence of hyperaemia. 23 However, the preoperative diagnosis with WLI endoscopy may be discordant with the postoperative pathological finding, leading to overtreatment or undertreatment.
In the last 20 years, NBI endoscopy has become a central diagnostic device for laryngeal disease. 24 Narrow band imaging is based on the change of the standard WLI endoscope in which white light is transmitted through optical filters absorbing all but 2 wavelengths; 1 band between 400 and 430 nm centered at 415 nm and another between 525 and 555 nm centered at 540 nm. 5 The former wavelength penetrates the superficial mucosa and highlights submucosal capillaries as a brown color while the latter penetrates through the submucosal layer and identifies prominent vessels as cyan in color. 25 As other squamous cell carcinomas arising from the upper aerodigestive tract mucosa, laryngeal tumor is accompanied by neoangiogenesis.26,27
In the present review, we focused on the accuracy of preoperative evaluation of vocal fold leukoplakia with NBI in comparison with histology through a literature review that included 5 articles.
Stanikova et al 14 described the results of NBI assessment of the epithelium around the leukoplakia in 63 patients. They reached an accuracy level of 84.6% for the diagnosis of high-grade dysplasia and carcinoma with NBI. The principal difficulties have been observed in the assessment of the narrow-angled turning loop under the still translucent epithelium arising from deeper layers of the vocal cord. In their materials, intrapapillary capillary loop (IPCL) changes were observed in 6 cases, with moderate dysplasia confirmed histologically in 4 (66.7%) biopsies and carcinoma in situ in the other 2 (33.3%). 14
Huang et al 15 analyzed 57 patients with 78 lesions of leukoplakia using NBI and were able to predict the high-grade dysplasia and carcinoma in situ in 43 of 45 patients, resulting with the accuracy of 95.56% and significant correlation between NBI and histopathology (κ index 0.711). The principal limit of NBI was found with some leukoplakia that had a broad scope and the surrounding mucosa was not entirely visible. 15
Rzepakowska et al 13 published a prospective study that included 62 patients with 91 cases of leukoplakia on vocal folds and showed that accuracy of NBI in predicting malignancy within leukoplakia was 97.8%. Their observation discovered distinctive features of leukoplakia among patients. In some patients, the lesion appeared translucent, allowing the vessels beneath to be traced. In other cases, atypical vascular pattern of the surrounding mucosa suggested advance-stage dysplasia and they found this feature helpful in the differentiation of malignancy within leukoplakia.
Ni et al, 12 in order to improve the accuracy of the Ni classification, 28 further divided the vocal cord leukoplakia into several subtypes and proposed a new NBI classification focusing on laryngeal leukoplakia. This new classification focuses on the presence of perpendicular vascular pattern with large brown spots on the vocal mucosa around the leukoplakia. To facilitate the observation using the NBI filter, the locations and sizes of spots have been distinguished in 6 different types of leukoplakia. It is important to underline that the presence of the perpendicular vascular patterns is indicative of a malignant lesion.
The new system was proposed to resolve the difficulties brought by the above “umbrella effect” and improve the consistency between NBI endoscopic diagnosis and pathological diagnosis. The accuracy of this classification in judging the pathological nature of vocal cord leukoplakia was 90.8%, which is significantly better than that of the conventional WLI endoscopy (70%).
Consecutively, the same group 11 decided to explore the utility of their NBI classification in the diagnosis of laryngeal leukoplakia by junior and senior doctors with different levels of experience. They found that the NBI endoscopy could improve the diagnostic accuracy of less-experienced laryngologists.
In 2019, Rzepakowska et al 29 evaluated 57 patients with 84 lesions. Although this manuscript was not included in the current review as it did not respect all the inclusion criteria, we decided to comment it as their results are interesting. The authors analyzed the vocal fold vibratory function using laryngovideostroboscopy and observed the texture, color, thickness, and size of the leukoplakia with NBI, along with a valuation of the adjacent mucosa vascularization. The results established that the perpendicular vascular pattern and the limited or absent mucosal wave appear to be the most potent signs in distinguishing benign and malignant leukoplakia.
In the last years, NBI has been utilized even for the study of the oral cavity.30,31 Several studies30-33 focused on the use of NBI in oral lesions, demonstrating that the IPCL patterns shown by NBI can be helpful in characterizing oral leukoplakia with high-grade dysplasia or invasive carcinoma.
All the studies included in our review demonstrated that NBI endoscopy could be suggested as an accurate method in predicting the risk of malignant transformation within the vocal fold leukoplakia. Actually, accuracy of NBI in predicting malignancy within leukoplakia was from 81% to 97.8% (Table 2). In consideration of the “umbrella effect,” studies included in our review suggest to observe the entire vocal cord closely, with special attention to the atypical vascular pattern of the surrounding mucosa. 15
Reviewed studies also confirm the importance of evaluating IPCL when analyzing leukoplastic lesions. Intrapapillary capillary loop, a sign suggestive for malignancy, is a perpendicular vascular pattern characterized by large brown sports or twisted earthworm-like vessels distributed at the surface of the vocal cord outside the leukoplakia.32-34 Special attention to the atypical vascular pattern of the surrounding mucosa is fundamental for the diagnosis, as studies have demonstrated that the IPCL patterns shown by NBI can be helpful in detecting leukoplastic lesions with higher grade dysplasia or invasive carcinoma.16,35-37
Conclusion
The promising outcomes of this systematic review appear to support the use of NBI in the diagnostic workup of laryngeal leukoplakia.
Narrow band imaging can help otolaryngologists in the decision-making process on the necessity to perform a biopsy and transoral surgery or long-term follow-up. Larger studies are necessary to confirm the high association of NBI evaluation of the epithelium surrounding the leukoplakia with the histological diagnosis. The IPCL patterns shown by NBI can be helpful in detecting leukoplastic lesions.
One of the main limits of NBI is the correct evaluation of leukoplakia in patients who underwent transoral laser microsurgery and even more in those treated with radiotherapy, in which the chronic inflammatory changes of the mucosa make the valuation of the pattern vessels more challenging.
Footnotes
Authors’ Note
Flaminia Campo and Massimo Ralli contributed equally. The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.