
Abstract
Objectives:
To explore the diagnostic value and pathological correlation of narrow band imaging (NBI) classification in laryngeal lesions.
Methods:
A total of 112 patients (123 lesions) with laryngeal lesions from July 2018 to May 2019 were selected in this study. All patients were examined by NBI and white light imaging endoscopy. The NBI endoscopy was applied to classify the observed lesion sites according to intraepithelial papillary capillary loop pattern. The gold standard of diagnosis was pathological results. To evaluate the consistency of NBI classification and pathological results.
Results:
The sensitivity, specificity, positive predictive value, and negative predictive value of the diagnosis for benign, precancerous, and malignant lesions under the NBI endoscopy were 90.91%, 81.19%, 74.07%, 85.42%; 41.67%, 92.93%, 58.82%, 86.79%; and 93.51%, 65.22%, 91.14%, 68.18%, respectively. There was a high consistency between NBI classification and pathological results (κ = 0.679, P < .001).
Conclusions:
The NBI classification can improve the accuracy of the diagnosis of laryngeal lesions. It is important for early diagnosis and treatment of vocal cord leukoplakia and laryngeal cancer.
Introduction
Vocal cord leukoplakia refers to the white plaque like protuberance on the surface of vocal cord mucosa caused by long-term stimulation factors such as smoking, alcohol consumption, excessive use of voice, laryngopharyngeal reflux, and human papilloma virus infection. The main symptom is hoarseness. 1 Vocal cord leukoplakia is characterized by great pathological differences and a certain tendency of malignant transformation. 2 Part of vocal cord leukoplakia turns into laryngeal cancer. Laryngeal cancer is common malignant tumors of head and neck with poor prognosis. Lymph node metastasis can occur in the early stage due to concealed location and strong invasion. 3 Therefore, it is a great significance for the choice of clinical treatment and prognosis to make a more precise histopathologic diagnosis of laryngeal cancer in the early stage. Narrow band imaging (NBI) endoscopy can identify malignant lesions on the mucosal surface by observing the morphology of intraepithelial papillary capillary loop (IPCL). In recent years, NBI endoscopy has been gradually applied to the diagnosis of laryngeal lesions. This study systematically reviewed 112 patients with laryngeal lesions, intending to evaluate the application value of NBI endoscopy in the diagnosis of different pathological types of laryngeal lesions by comparing the consistency between the NBI classification and pathological results.
Materials and Methods
Clinical Materials
A total of 112 patients with laryngeal lesions (123 lesions) from July 2018 to May 2019 in the outpatient department of Nanjing Drum Tower Hospital were selected, including 104 males and 8 females, aging from 41 to 91 years. One hundred and twenty three cases of laryngeal lesions clinically suspicious for malignancy including 9 cases of glottic laryngeal carcinoma, 11 cases of supraglottic laryngeal carcinoma, 3 cases of laryngeal papilloma, 19 cases of laryngeal high-grade intraepithelial neoplasia, and 81 cases of vocal cord leukoplakia (22 cases of vocal cord chronic inflammation/epithelial proliferation/dyskeratosis/hyperkeratosis, 21 cases of vocal cord low-grade intraepithelial neoplasia, 38 cases of vocal cord high-grade intraepithelial neoplasia according to final histopathology results) were observed. Each lesion was first observed by white light imaging (WLI) endoscopy and then observed by NBI endoscopy. All patients underwent pathological examination. This study was approved by the medical ethics committee of the hospital, and all patients signed the informed consent form of flexible fiberoptic laryngoscopy and biopsy.
Equipments
ENT treatment unit, NBI flexible fiberoptic laryngoscopy produced by Olympus company (VT and VT2 models, pipe with pliers), matching laryngeal forceps (FB-52C-1 model), CLV-S40Pro cold light source, Sony LCD monitor, OTV-S7Pro camera system, and computer image-text and printers were used. The laryngoscopy of VT2 model has NBI function, which can be switched to as needed at any time.
Methods of Examination
Patients were placed in sitting position. Before endoscopic examination, bilateral nasal mucosa was anesthetized with 1% tetracaine and 1% ephedrine, 1% tetracaine also was used to surface anesthesia of oropharyngeal and laryngopharyngeal mucosa. The oropharynx, hypopharynx, and larynx were examined by WLI model and NBI model through the patient’s nasal cavity, respectively, representative pictures were collected at the same time.
Classification of NBI
The laryngeal lesions were classified into 7 types according to IPCL morphology under NBI endoscopy (Figure 1)
4
: Type I: There are no IPCL, oblique vessels and dendritic vessels are visible. It is mainly seen in normal mucosa and vocal cord polyps, cysts, granulation, and scarred mucosa. Type II: The morphology of IPCL is almost invisible, but oblique vessels and dendritic vessels are clear, obviously congestion. It is mainly seen in inflammation. Type III: The morphology of IPCL is invisible and the mucosa is white. Whether the oblique and dendritic vessels are visible depends on the thickness of white spot. It is mainly seen in vocal cord leukoplakia. Type IV: The morphology of IPCL is visible, regularly arranged, sparser density, and slightly dilated, which is characterized by small brown spots. Oblique vessels and dendritic vessels are invisible. It is mainly seen in low-grade intraepithelial neoplasia. Type Va: The diameter and density of the IPCL are increased, showing irregular shape of solid or hollow larger brown spots. It is mainly seen in high-grade intraepithelial neoplasia and carcinoma in situ. Type Vb: The morphology of IPCL is damaged, expanded, extended, and distorted. The irregular point shape of IPCL is extended to the twisted line shape, which is like snake, earthworm, or tadpole. The main pathology is invasive carcinoma. Type Vc: The structure of IPCL disappeared and new tumor blood vessels generated. Different shapes, irregular and uneven density of abnormal vessels are visible at the surface of tumor. Type I-III lesions are considered as benign, type IV lesions are considered as precancerous, and type Va-c lesions are considered as malignant.
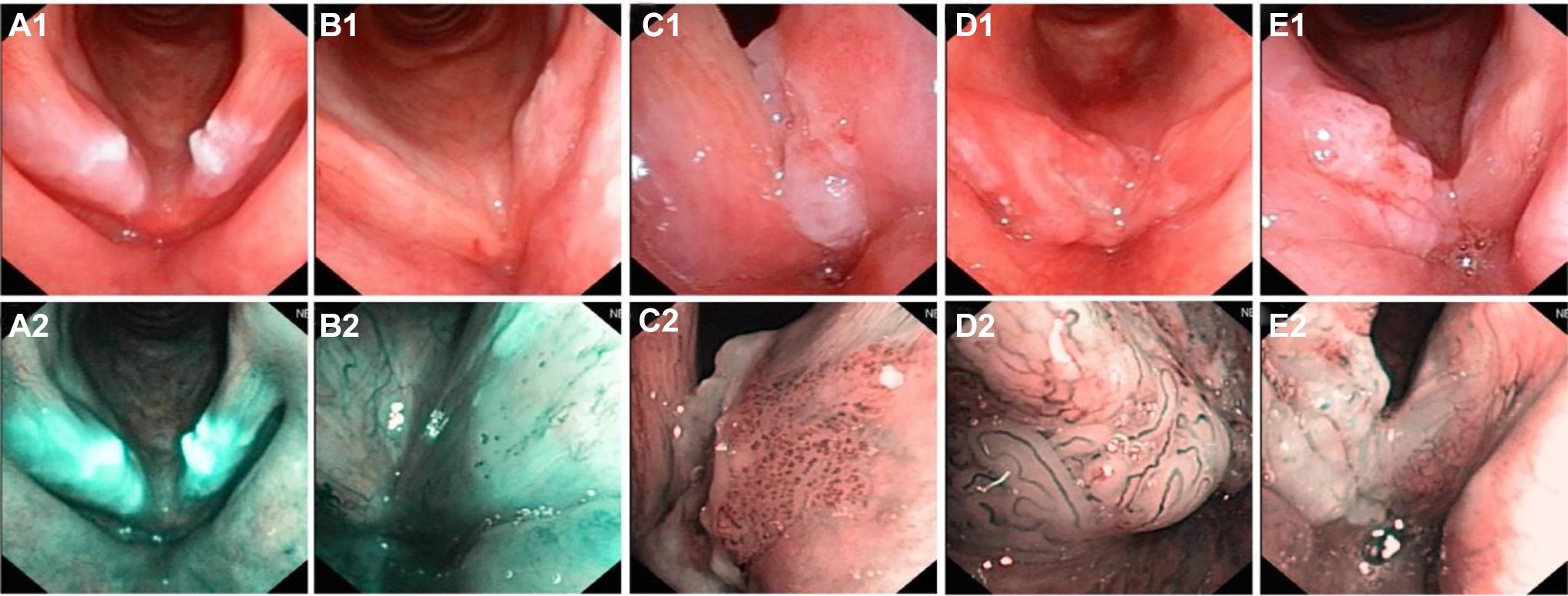
Narrow band imaging classification of pharyngolaryngeal lesions according to IPCL patterns. (A1-A2) type III: They are common in vocal leukoplakia, most pathologic findings are chronic inflammation with epithelial proliferation, dyskeratosis, hyperkeratosis. (B1-B2) type IV: Most of pathological type is low-grade intraepithelial neoplasia. (C1-C2) type Va: High-grade intraepithelial neoplasia and carcinoma in situ are common. (D1-D2) type Vb: Invasive carcinoma is the main pathological type. (E1-E2) type Vc: The pathological type is invasive carcinoma.
Pathologic Diagnosis
All patients were biopsied under NBI endoscopy and sent to pathology department for pathological examination. Pathological results were considered as the diagnostic gold standard. According to the classification standard of head and neck tumors revised by World Health Organization in 2017, 5 they were classified into chronic inflammation of mucosa or squamous epithelial hyperplasia (keratosis, hyperkeratosis, and dyskeratosis), low-grade intraepithelial neoplasia, high-grade intraepithelial neoplasia, carcinoma in situ, and invasive carcinoma. Some benign lesions with cancer tendency may turn into cancer if not cured in time called precancerous lesions, papilloma and low-grade intraepithelial neoplasia were classified as precancerous lesions in this study.
Statistical Analysis
SPSS 22.0 software was used for statistical analysis in the study. The sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of the diagnosis of laryngeal lesions under NBI endoscopy were calculated. The κ test was used to verify the consistency between NBI classification and pathological results; κ <0.4 indicated low consistency, 0.4 to 0.6 indicated moderate consistency, and kappa >0.6 indicated high consistency. P < .05 was considered statistically significant.
Results
Diagnostic Value of NBI Endoscopy for Laryngeal Lesions
There were 22 benign lesions, 24 precancerous lesions, and 77 malignant lesions according to the pathological results. There were also 27 benign lesions, 17 precancerous lesions, and 79 malignant lesions according to the NBI diagnosis. The total detection rate of laryngeal lesions under NBI endoscopy was 82.93% (102/123). The sensitivity, specificity, PPV, and NPV of the diagnosis for benign lesions under the NBI endoscopy were 90.91%, 81.19%, 74.07%, and 85.42%, respectively. The sensitivity, specificity, PPV, and NPV of the diagnosis for precancerous lesions under the NBI endoscopy were 41.67%, 92.93%, 58.82%, and 86.79%, respectively. The sensitivity, specificity, PPV and NPV of the diagnosis for malignant lesions under the NBI endoscopy were 93.51%, 65.22%, 91.14%, and 68.18%, respectively (Table 1).
Diagnostic Value of NBI Endoscopy for Laryngeal Lesions.a
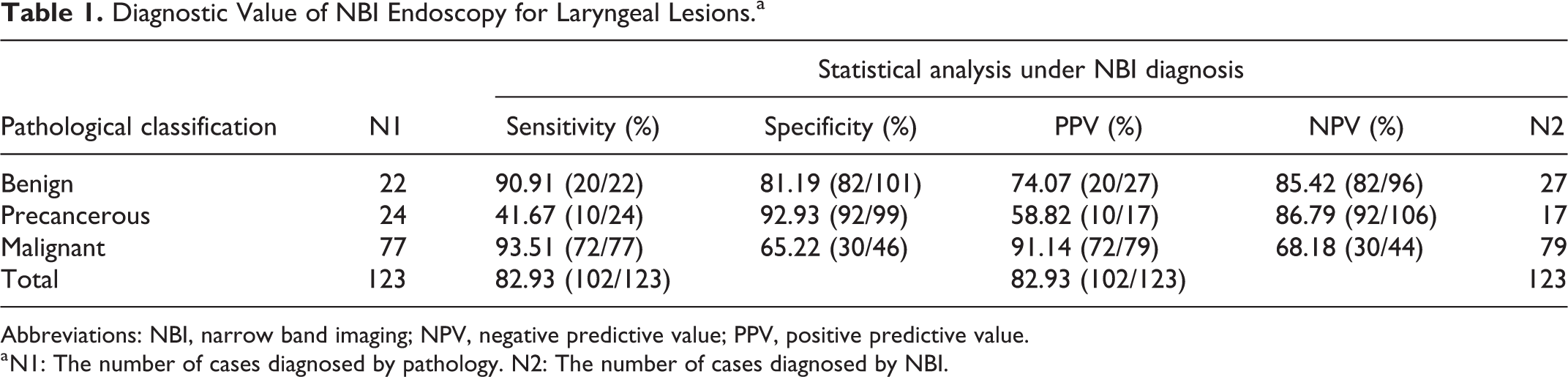
Abbreviations: NBI, narrow band imaging; NPV, negative predictive value; PPV, positive predictive value.
a N1: The number of cases diagnosed by pathology. N2: The number of cases diagnosed by NBI.
Correlation Between NBI Classification and Pathological Diagnosis
According to the pathological results and NBI classification, 22 cases of laryngeal lesions were related to chronic inflammation with epithelial proliferation/dyskeratosis/hyperkeratosis, 3 cases of laryngeal lesions were related to papilloma, 21 cases of laryngeal lesions were related to low-grade intraepithelial neoplasia, 57 cases of laryngeal lesions were related to high-grade intraepithelial neoplasia/ carcinoma in situ, 20 cases of laryngeal lesions were related to invasive carcinoma, 27 cases of laryngeal lesions were classified as type III, 17 cases of laryngeal lesions were classified as type IV, 44 cases of laryngeal lesions were classified as type Va, 27 cases of laryngeal lesions were classified as type Vb, and 8 cases of laryngeal lesions were classified as type Vc (Table 2). The κ test showed that there was a high consistency between NBI classification and pathological results (κ = 0.679, P < .001).
Correlation Between NBI Classification and Pathological Diagnosis.
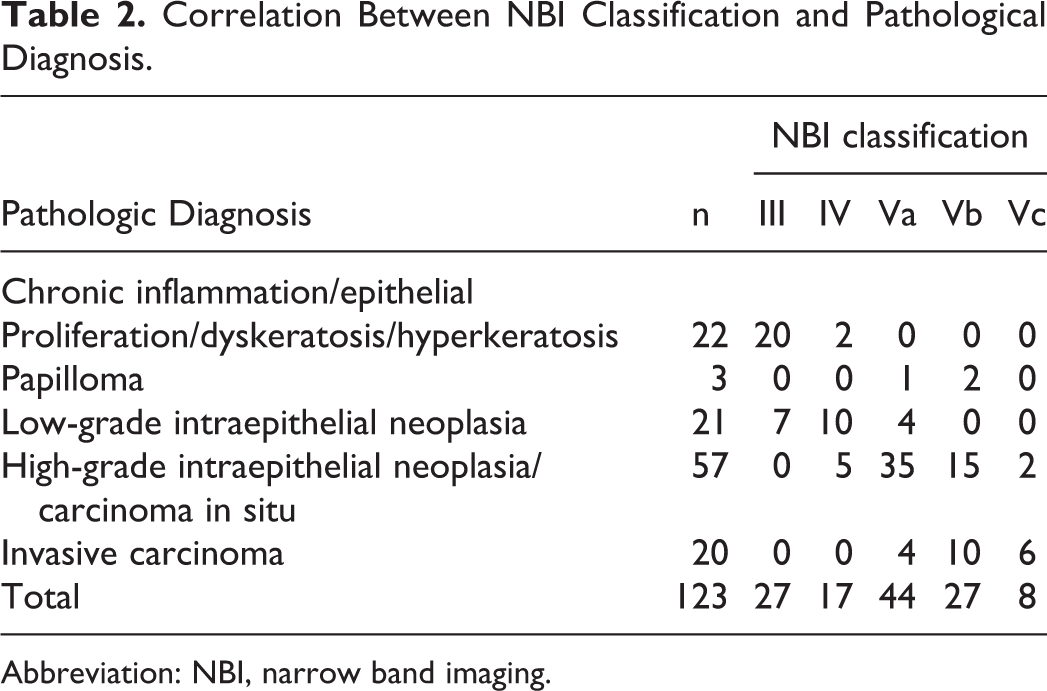
Abbreviation: NBI, narrow band imaging.
Discussion
Vocal cord leukoplakia is one of the common diseases of throat. The pathological types of vocal cord leukoplakia are various, including benign lesions, precancerous lesions, and malignant lesions, which are considered as precancerous lesions of laryngeal cancer. 6 Recently, the incidence of vocal cord leukoplakia gradually increased. At present, the primary diagnosis of vocal cord leukoplakia mainly depends on histopathological biopsy under flexible fiberoptic laryngoscopy. The treatment of vocal cord leukoplakia is closely related to the diagnosis.2,7 Laryngeal cancer is also common severe diseases of head and neck, 95% are squamous cell carcinoma. Despite there are many advanced methods of examination, most patients are diagnosed with advanced disease, the 5-year survival rate is low. Therefore, the early diagnosis of laryngeal lesions is particularly important. However, the WLI endoscopy is difficult to detect subtle lesions on the mucosal surface due to the limitations of resolution and contrast. 8
As a new endoscopic examination method, NBI endoscopy played an important auxiliary role in the diagnosis of head and neck cancers in the past years.8-10 The NBI endoscopy filtered out the red light with the longest wavelength (695 nm) among the red, green, and blue light of WLI endoscopy through light filtration technology, only blue light with a wavelength of 415 nm and green light with a wavelength of 540 nm are released.11,12 Since the absorbable wavelength of hemoglobin was about 415 nm, blue light could be well absorbed by hemoglobin, so that NBI endoscopy could clearly show the changes in the morphology and structure of capillaries on the surface of the mucosa and submucosa. In NBI mode, the submucosa vessels were dark green, while the submucosa dendritic vessels were tan. Dendritic vessels were communicated with each other, dividing into oblique vessels, which further sent out the terminal branches of capillaries, called IPCL. 13 Normally, IPCL was almost invisible.
In our study, there were 123 cases of laryngeal lesions (77 malignant, 22 benign, 24 precancerous). The diagnostic accuracy of NBI endoscopy was 82.93%. The sensitivity of the diagnosis for benign lesions, precancerous lesions, and malignant lesions under the NBI endoscopy were 90.91%, 41.67%, and 93.51% respectively. The results indicated that NBI endoscopy could improve the accuracy of diagnosis in laryngeal lesions and help us to choose the appropriate treatment in the early stage, especially for malignant lesions. The κ test showed that there was a high consistency between NBI classification and pathological results (κ = 0.679, P < .001). The NBI classification had a good guidance for us to evaluate the benign and malignant lesions.
On the contrary, we noted that the sensitivity of the diagnosis for precancerous lesions under the NBI endoscopy was low. In this study, papilloma and low-grade intraepithelial neoplasia were classified as precancerous lesions with special clinical characteristics. Three cases of papilloma under NBI endoscopy showing type V lesions according to IPCL pattern, but the pathological results were 2 of benign and 1 of low-grade intraepithelial neoplasia, this may lead to misdiagnosis, and the NBI classification may not be suitable for the diagnosis of papilloma. Besides, we conducted tissue biopsy in the outpatient departments, the clipped tissue was not deep enough, which may lead to the difference between the pathological results and the real results.
Despite more and more studies have reported that the diagnostic value of NBI endoscopy for laryngeal lesions were higher than WLI endoscopy, there was still controversial. Ni et al reported that the sensitivity and specificity of NBI endoscopy for malignant leukoplakia were 82.6% and 92.8%. 14 But some other studies indicated that severely keratosis lesions may blocked the underlying malignant lesions, which was lead to a false negative. 15 During the application of NBI endoscopy to observe the vocal cords leukoplakia, some lesions had thicker leukoplakia and wider coverage, while the penetration of NBI was weak, which was affected the observation of the vascular morphology at the surface of mucosa.
Therefore, we should make reasonable use of the advantages of NBI endoscopy to help us diagnose laryngeal lesions.
Conclusion
In brief, NBI endoscopy as a new noninvasive endoscopy technology, it is easy to operate and can better show the subtle lesions and abnormal vessels of mucosa. The NBI classification can improve the accuracy of the early diagnosis of laryngeal lesions. There was a high consistency between NBI classification and pathological results. The NBI endoscopy also has some limitations, it cannot completely replace pathological examination. There are also differences in the accuracy of each study in the diagnosis of lesions. More high-quality studies are needed to further confirm the diagnostic value of NBI endoscopy in laryngeal lesions.
Footnotes
Authors’ Note
Chuanyao Lin and Sisi Zhang are the co-first authors. There was no patient identifiable information in our study. This article does not contain any studies with human participants or animals performed by any of the authors.
Acknowledgments
The authors gratefully thank to the support of The Project of Invigorating Health Care through Science, Technology and Education.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from Jiangsu Provincial Medical Youth Talent of the Project of Invigorating Health Care through Science, Technology and Education (QNRC2016002); National Science Foundation for Young Scientists of China (No. 81700913); The Project of Invigorating Health Care through Science, Technology and Education (ZDXKB2016015).