
Abstract
Tuberculosis of the middle ear is a rare but treatable disease; however, delays in diagnosis and treatment usually lead to complications. Diagnosis is made difficult by most physicians being unfamiliar with the typical presenting features and special cultural and pathologic studies being required for diagnosis. A case report and literature review are presented, illustrating typical clinical, epidemiologic, and laboratory features, as well as complications and the treatment of tuberculous otitis media.
Keywords
Introduction
Tuberculous otitis media (TOM) is one of the rarest extrapulmonary forms of tuberculosis. Most patients show silent otorrhea, moderately severe hearing loss, ipsilateral facial paralysis, and multiple perforations with granulation tissue. With the advent and development of antibiotics, however, symptoms are nonspecific. Diagnosis of TOM is challenging due to a scant incidence, variable signs and symptoms, and the fact that specific tests for tuberculosis are not routinely requested. Delayed diagnosis leads to delayed treatment onset, and, thus, increases risk of complications such as facial paralysis or irreversible hearing loss. A case report and literature review are presented to illustrate typical clinical, epidemiologic, and laboratory features, as well as complications and treatment of TOM.
Case Report
A 27-year-old woman first presented to our hospital with complaints of decreased hearing and refractory purulent bilateral discharge for 6 months. She was diagnosed with suppurative chronic otitis media at another institute and received regular antimicrobial eardrops for 6 months. Examination at our hospital revealed stenosis of the external auditory canal of both ears, allowing no visualization of the tympanic membrane. Computed tomography images showed inflammation of the mastoid and the middle ear cavity with no destruction of the ossicular chain (Figure 1A and B). A drainage culture of the drainage was negative. Pure tone audiometry assessment showed moderate bilateral conductive hearing loss. Drainage was enhanced under endoscope and retroauricular injection of methylprednisolone was performed per month. Otorrhea reduced but still occurred intermittently. One year later, she was admitted for fever, cough, and persistent headache for one month to another hospital, and a diagnosis of pulmonary tuberculosis and tuberculous meningitis (TBM) was made. She was started on antitubercular drugs and complete resolution of otorrhea and external ear canal stenosis was noted after 2 months. Hearing, however, reduced significantly following another 5 days. Bilateral profound hearing loss was confirmed by pure tone audiometry. Examination showed no signs of remnant tympanic membrane of both ears and computed tomography demonstrated disrupted ossicles (Figure 1C and D). A 25-decibel improvement was noted at low frequencies in the right ear at the 4-month follow-up as the tympanic membrane regenerated (Figure 2).
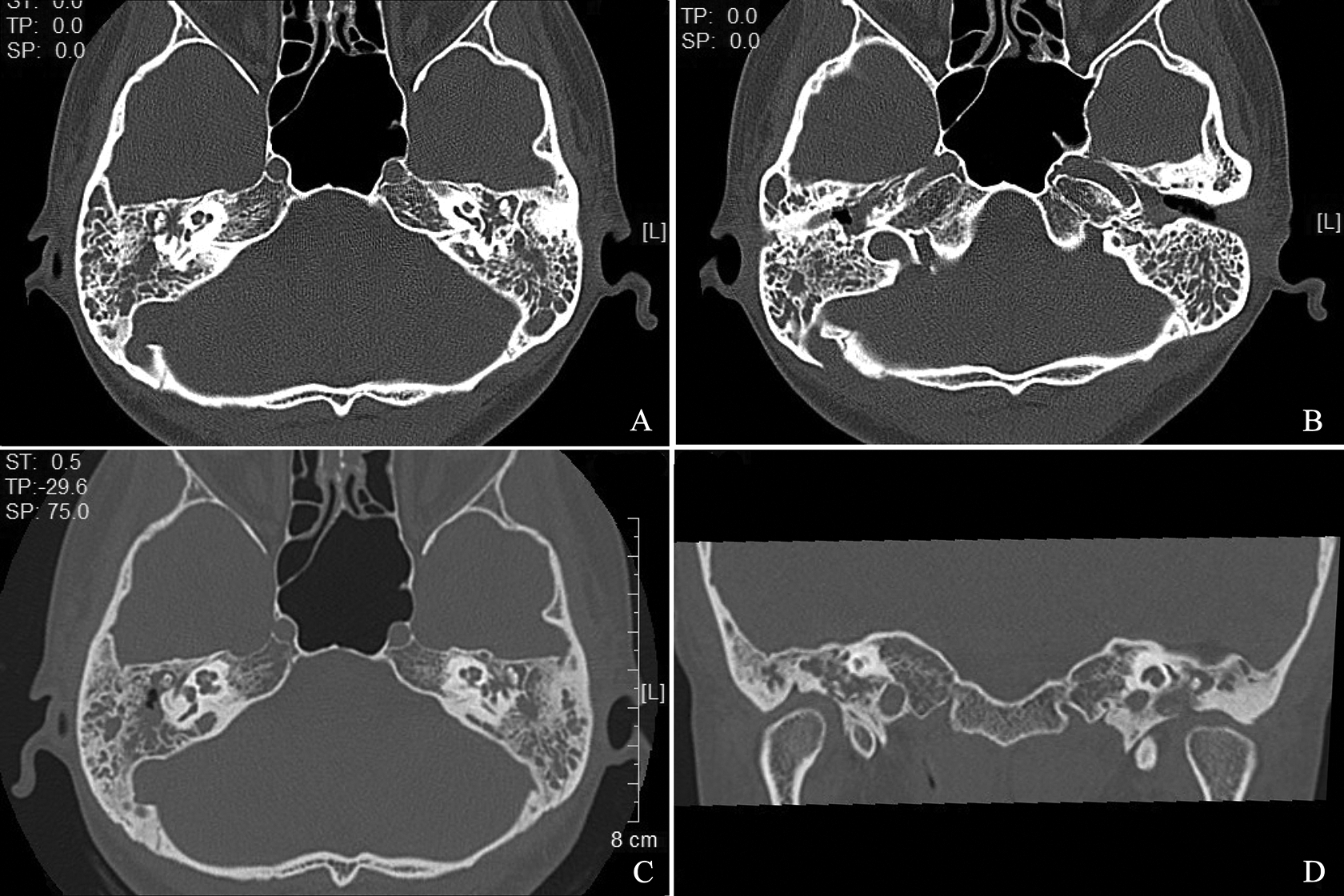
A and B, Characteristic computed tomography images showing soft tissue occupation of the mastoid and the middle ear cavity with complete ossicles at the early stage. C and D, Axial and coronal images showing bilateral disrupted ossicles after 1.5 years.
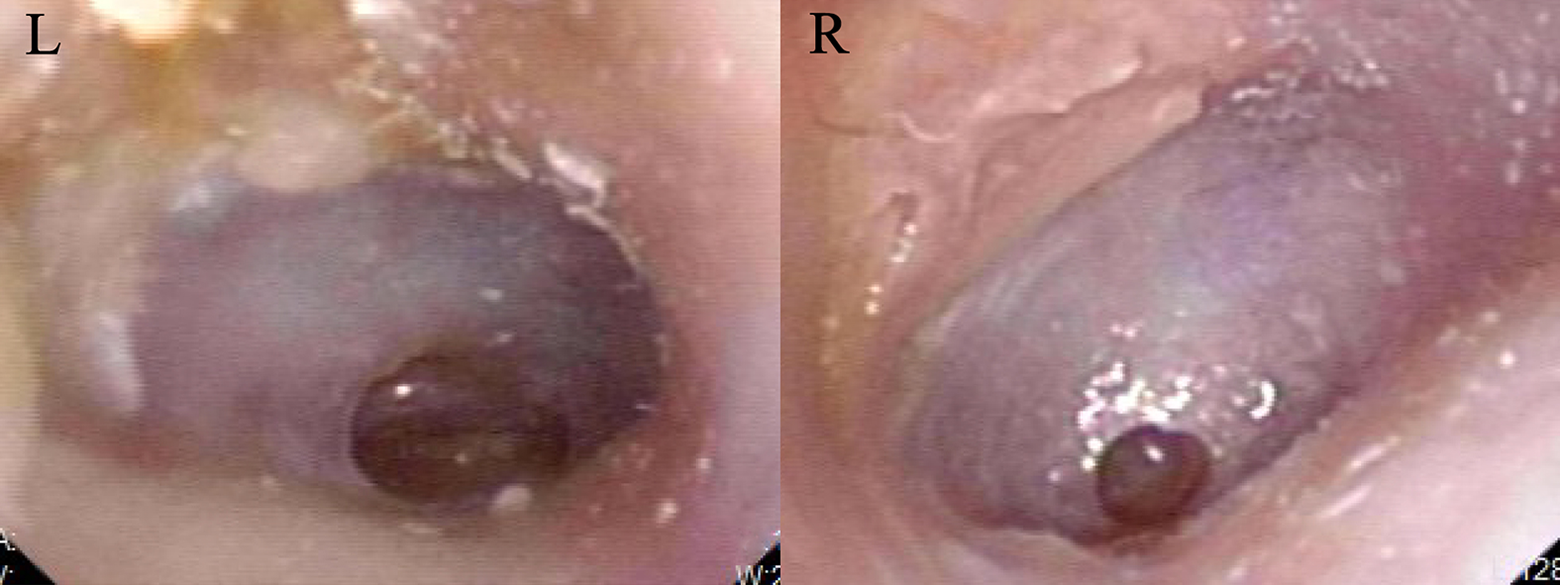
Pictures showing bilateral tympanic membrane regeneration at the 4-month follow-up after profound sensorineural hearing loss.
Discussion
Tuberculosis of the middle ear was first demonstrated by Eschle in 1883. 1 Due to the wide use of antituberculosis medication, the incidence has been decreasing, accounting for between 0.05% and 0.9% of chronic infections of the middle ear. 2
Tuberculous bacilli make their way to the middle ear and mastoid through the Eustachian tube, the blood stream, and rarely, through the external auditory meatus. 1,3
The full triad of painless otorrhea, multiple tympanic perforations, and facial palsy is rarely noted today. Most patients present with intermittent otorrhea and hearing loss with no major distinction from nonspecific chronic otitis media. 4 Hearing loss, sometimes profound, is almost permanent unless treatment is given at an early stage, which makes early diagnosis crucial. Moreover, the degree of hearing loss seems to be disproportionate to the apparent damage especially in early cases. 3 Facial nerve paralysis is usually noted in children. Suspicion of TOM should be raised when facial paralysis complicates chronic otorrhea and cholesteatoma is excluded. 4 A history of pulmonary tuberculosis or tuberculosis contacts is a good indicator of the disease. However, an absence of such history does not preclude the diagnosis. A review of the 20th-century English-language literature 1 indicated that 42% of patients with TOM have no evidence of pulmonary tuberculosis, and, conversely, most reports from tuberculosis sanatoriums indicated a rate of 2% for tuberculous ear involvement in patients with active pulmonary tuberculosis. Primary tuberculosis is usually symptomless but Mycobacterium tuberculosis that reaches the draining hilar lymph nodes may be seeded into the bloodstream, leading to widespread infection.
The diagnosis is based on microbiological or histological identification of M tuberculosis, or the presence of characteristic tuberculous granulomas with caseous necrosis, epithelioid cells, or Langerhans giant cells. 2 However, definitive identification of M tuberculosis is not always easy to achieve due to dispersed tuberculous granulomas (absent from some areas) in the otic mucosa, as well as low bacillus concentrations in tuberculous lesions of the ear. 5,6 When there are strong clinical grounds for suspicion but diagnostic tests are consistently negative, a diagnosis ex juvantibus should be given and TOM treatment should be discussed with the patient. 6 Purified protein derivative (PPD) tests can be indicative of tuberculous otitis but have a poor predictive value and patients with a negative PPD test may still have TOM. Conversely, patients with chronic otitis media due to other pathogens may have positive PPD tests. 3 Molecular methods, especially if polymerase chain reaction based, have high reliability, sensitivity, and specificity, enabling rapid detection of mycobacterial DNA directly in clinical samples. 7
Tuberculous otitis media may give rise to facial paralysis, labyrinthitis, petrositis, lateral sinus thrombophlebitis, meningitis, and brain abscess. The most common mode of spread of tuberculosis to the central nervous system is hematogenous. The focus of infection may be either in the primary site of the lungs or the infected middle ear. The mode of meningeal involvement can also be due to direct extension from the middle ear through the round and oval window, the tegmen tympani, or mastoid. The close proximity of all these structures also aids in the rapid spread of infection. 8,9
Tuberculous meningitis is especially common in young children and people with untreated HIV infection, and it kills or disables roughly half of the people affected. 10 As Paul reported, TBM represented 1.9% of all TOM, with most cases occurring in the context of miliary tuberculosis. The course of TBM is typically subacute or chronic, with many days or weeks of headache, fever and vomiting, culminating in loss of consciousness, focal neurological deficit, and death, unless anti-TB chemotherapy is instituted. 11 Cerebrospinal fluid (CSF) examination, the most reliable TBM diagnostic tests, typically shows raised white cells counts (0.05 × 109 − 1.00 × 109/L), with both neutrophils and lymphocytes; raised protein (0.5-2.5 g/L); and ratio of CSF to plasma glucose <0.5 in 95% of cases. 11
The relationship between meningitis and sensorineural hearing loss (SNHL) has long been studied. Meningitis is a major etiological factor for postnatal, acquired SNHL. In children, it is estimated that 5% to 7% with TBM will develop SNHL. 12 The mechanism of TBM causing SNHL is unclear but may result from hematogenous, lymphatic, perineural, or direct spread to the inner ear structures, as with bacterial meningitis. 13
Kuan et al conducted a temporal bone study and concluded that the modiolus and cochlear aqueduct are the main routes for the spread of infection from the meninges to the inner ear. The progression of hearing loss resembles that of bacterial meningitis and shares attributes of retrocochlear SNHL. 12
The main treatment of tuberculosis and uncomplicated TOM is with 4 antitubercular drugs (isoniazid, rifampicin, ethambutol, and pyrazinamide) for at least 2 months, consolidated by treatment with 2 drugs (rifampicin and isoniazid) for another 4 months. When complicated by TBM, the consolidation period should be extended to 7 to 10 months. Multidrug resistant tuberculosis is a growing problem, with poor patient compliance or improper dosing frequently leading to drug resistance. Fluoroquinolones are highly effective anti-TB agents with good penetration of the blood–brain barrier and form a pillar of treatment for multidrug-resistant TB. 14 Treatment with anti-TB forms the back bone of TB therapy. Surgery is typically carried out to perform biopsies, remove bony sequestra, or treat complications.
Tuberculosis of the middle ear, a form of extrapulmonary tuberculosis, is today an uncommon disease. Diagnosis is a challenge. The clinician must maintain a high index of suspicion and must be aware of those features which tend to distinguish the tuberculous ear. Early diagnosis and treatment are crucial, preventing irreversible complications.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by Joint Funds for the innovation of Science and Technology, Fujian Province (Grant Number: 2019Y9131).