
Abstract
Purpose:
This study explores the changes in hearing thresholds in pregnancy.
Materials and Methods:
A prospective hospital-based observational study was performed with a total of 69 patients in the age-group of 18 to 40 years. Patients underwent hearing assessment twice during the study period. Conventional pure tone audiometry and impedance audiometry were performed, first during the antepartum period (28-32 weeks of gestational age) and second time during the postpartum period (6 weeks postpartum).
Results:
Significant difference was seen between the average of air conduction threshold values at speech frequencies when antepartum values were compared with postpartum values.
Conclusion:
The alterations in hearing sensitivity in pregnant females which improved during the postpartum period can be attributed to pregnancy.
Introduction
As per World Health Organization (WHO) estimates 2018, hearing loss is the fourth highest cause of disability globally with 6.1% of the world’s population having disabling hearing loss. 1 The effect of gender on hearing has been studied in past. 2 The mentioned effect has been hypothesized to be based on the hormone levels in the female body. The hormone levels in the females undergo changes depending on the stage of life. There are changes in the female body which are physiological and secondary to changes in the level of sex hormones (estrogen and progesterone). These cyclical changes are observed during pregnancy, menstrual cycle, and menopause. The alterations in the level of sex hormones affect the sensory nervous system which can affect hearing thresholds. 3 -5 Other theories like a difference in the anatomical length of the auditory pathway have also been put forward to explain the gender-related difference in hearing sensitivity. 6 The sex hormones also cause fluid retention in the female during pregnancy which accounts for an increase of 6.5 L of extracellular fluid and 1.2 L of intracellular fluid. 7 -9 Carlin and Alfirevic observed that in pregnant women, plasma volume increases by 10% above baseline nonpregnancy levels by 7 weeks of gestational age and plateaus at 32 weeks of gestational age at 45% to 50% above baseline. 10 This fluid retention and shift in osmolality can affect the inner ear and cause alteration in hearing sensitivity in pregnancy especially at low frequencies similar to what is seen in Meniere disease. 7 A case report by Uchida et al showed that the symptoms of a patient with Meniere disease worsened during pregnancy which also points toward the same pathophysiological mechanism associated with both the conditions. 11 There have been studies in past which observed similar changes in hearing threshold values in pregnancy. Kanadys and Oleszczuk observed a case of sudden sensorineural hearing loss in an uncomplicated pregnancy which they believed was due to the hypercoagulable state which occurs normally during pregnancy, which could lead to vascular occlusion in the microcirculation of inner ear. 12 Lavy in 1998 reported 2 cases of sudden sensorineural hearing loss and again, the cause was hypothesized to be increased levels of sex hormones leading to a hypercoagulable state and thus increasing the thrombogenic risk and possibly affecting the cochlear microcirculation. 5 Tandon et al and Sharma et al in 2 separate studies observed that normal pregnancy has some depressant effect on the auditory conduction pathway and these observations were based on a study conducted on a group of pregnant women. 6,13
In 2001, Stenberg et al tried mapping the estrogen receptors (ERs) in the human inner ear and found ERα to be present in the spiral ganglion and ERβ in the stria vascularis, both of the locations being important in auditory conductive pathway. 14 Kilicdag et al observed that postmenopausal women in normal population have better hearing with administered estrogen replacement therapy and suggested a possible protective effect of estrogen on hearing function. 15
We also found studies which refute any association of pregnancy and hearing loss. Tsunoda et al conducted pure tone audiometry (PTA) and tympanometry in a group of 56 pregnant women and found the hearing to be normal in all. 16 In view of polarized results obtained on search of the effect of pregnancy on hearing, we did this study to see the changes in hearing threshold values with pregnancy.
Materials and Methods
The study sample comprised 69 pregnant women attending the antenatal clinic between 28 and 33 weeks of gestational age. The patients were recruited from the Department of Obstetrics and Gynaecology, Lady Hardinge Medical College, New Delhi, with the period of study being November 2016 to March 2018.
The inclusion criteria was adhered to, which included pregnant women with single live fetus with gestational age of 28 to 33 weeks. Patients with diabetes mellitus or hypertension prior to pregnancy, ear diseases, previous history of sensorineural hearing loss, history of ototoxic drug intake, and history of previous ear surgery were excluded from the study.
Once included in the study, all the patients underwent a detailed history and examination as per predesigned proformas. The PTA was performed in a sound-proof room with minimal ambient or background noise. The PTA was done on Labat Audiolab Audiometer (Labat Asia Private Limited, Mohali [Punjab], India). HDA 300 Sennheiser earphones (Sennheiser, Germany) were used for measuring air conduction (AC) threshold values, and the bone conduction (BC) was tested by RadioEar B-71 Bone transducer (RadioEar, Middelfart, Denmark). Modified Hughson-Westlake method was used for conducting PTA. Impedance audiometry was done using MAICO MI44 impedance audiometer (MAICO diagnostics, Berlin, Germany).
Of the 69 pregnant women, 20 were lost to follow-up during the postpartum period because of the cultural factor involved wherein females are sometimes not allowed to leave the house in the immediate postpartum period. The comparison was thus done for the remaining test patients available. The AC and BC threshold values were compared between antepartum period and postpartum period. The AC threshold values were calculated for the following frequencies: 0.25, 0.5, 1, 2, 4, and 8 kHz, whereas for BC threshold values, frequencies used were 0.25, 0.5, 1, 2, and 4 kHz.
Categorical variables were presented in numbers and percentages, and continuous variables were presented as mean (standard deviation) and median. The observed data followed a normal distribution. The antepartum and postpartum observations were tested for significance by employing the z test for 2 sample means using the MS Excel statistical tool and a P value of less than .05 was considered statistically significant.
Results
There were statistically no significant differences in the baseline characteristics such as age, gestational age, gravida, and time period of follow-up. The demographic profile of the test patients is shown in a tabular form in Table 1.
Demographic Profile of Study Group.a
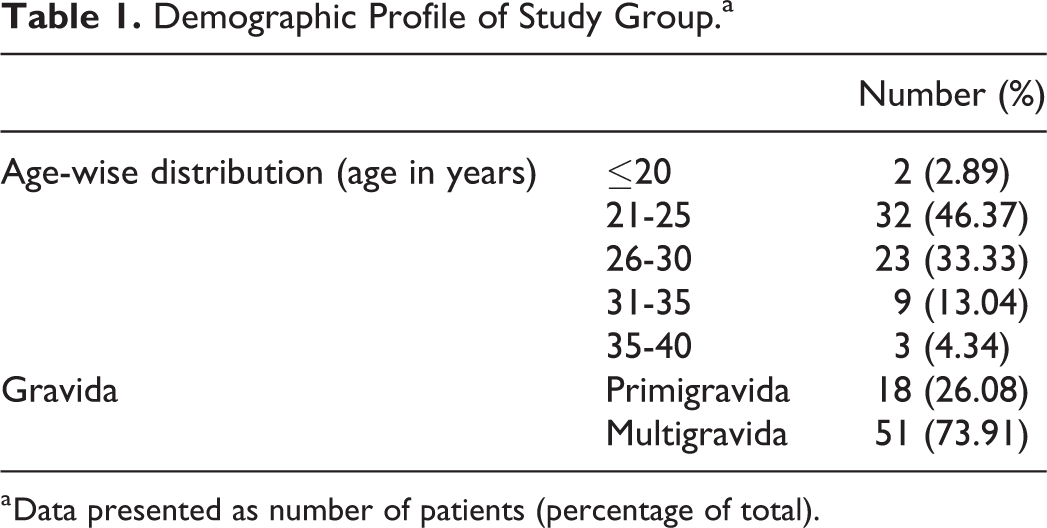
a Data presented as number of patients (percentage of total).
The antepartum hearing threshold values were compared with the postpartum values and a comparison has been presented in the form of graphs (Figures 1 –4). It was seen that although the hearing level was within the normal range in both antepartum and postpartum periods, there was a change seen with hearing improving postdelivery. The average of antepartum hearing threshold values was also compared with the postpartum values, and the changes seen were statistically significant (P value < .05). The findings are presented in a tabular form (Table 2).
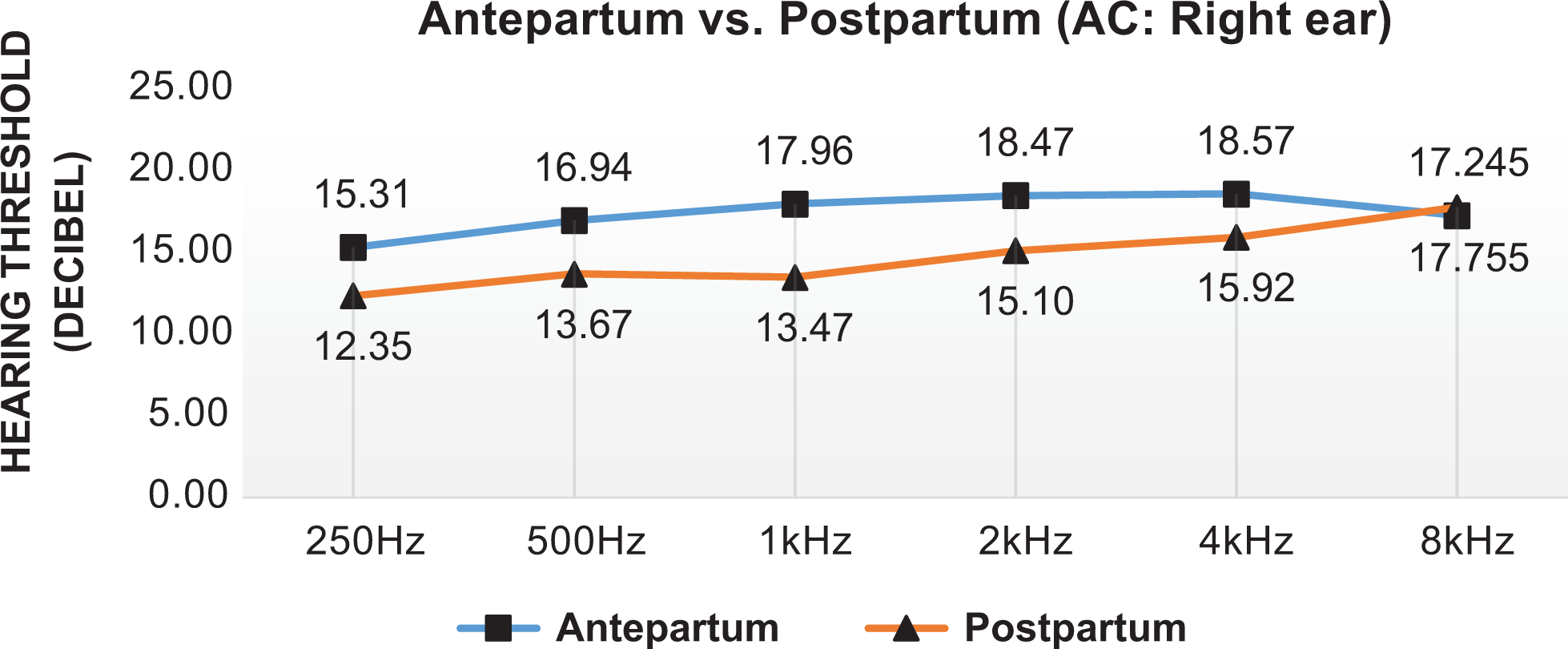
Air conduction hearing threshold: Right ear (Antepartum vs postpartum).
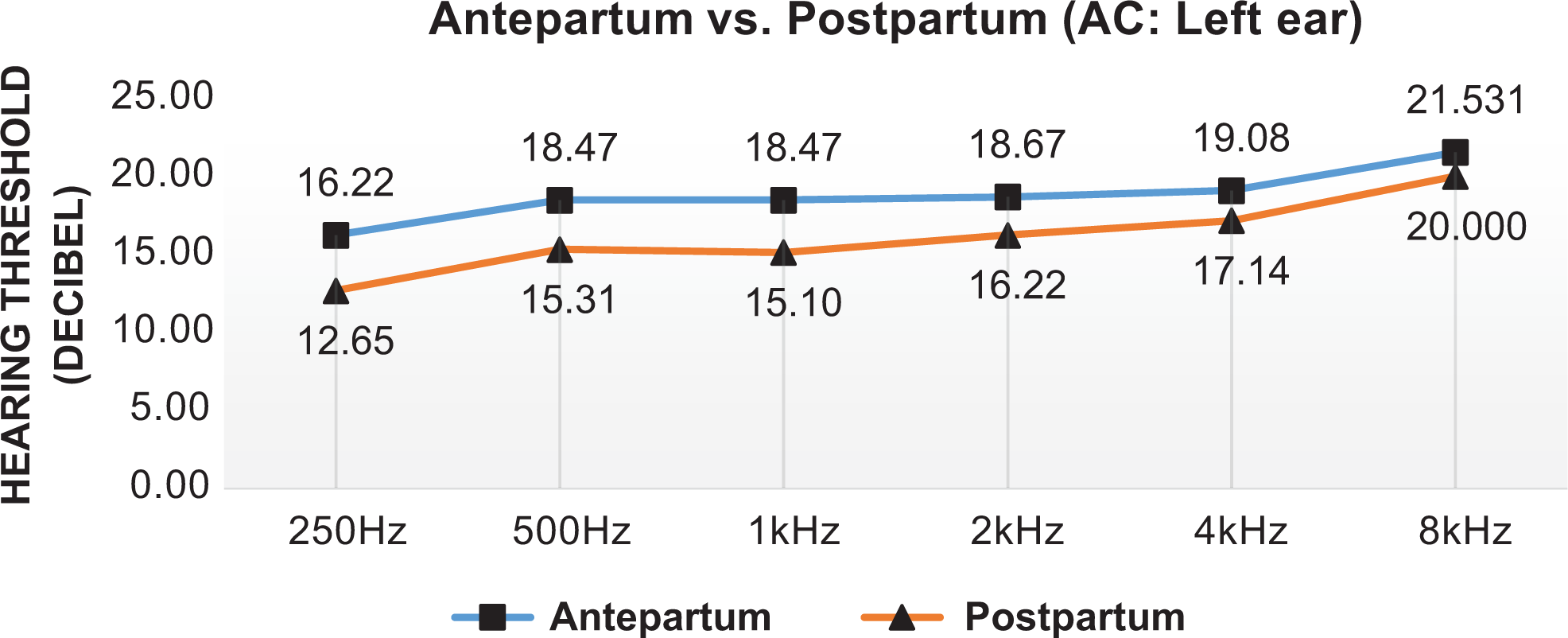
Air conduction hearing threshold: Left ear (Antepartum vs postpartum).
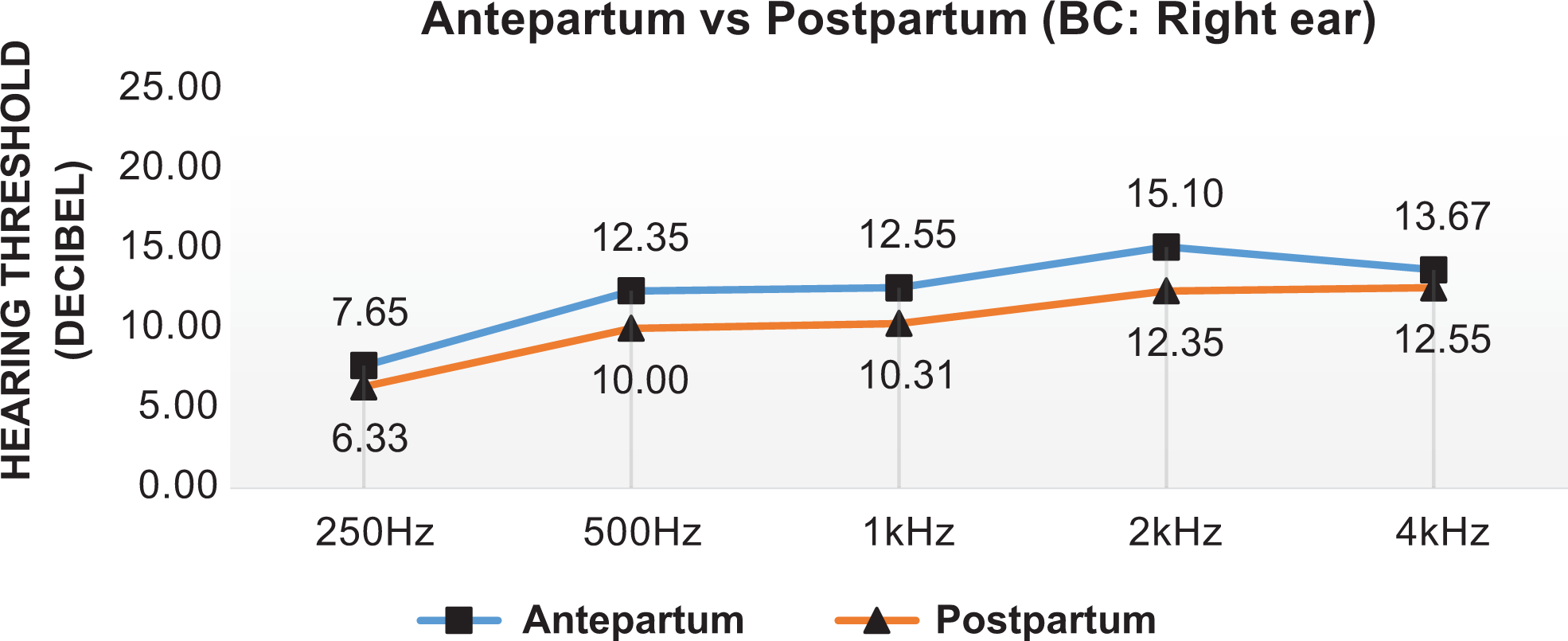
Bone conduction hearing threshold: Right ear (Antepartum vs postpartum).
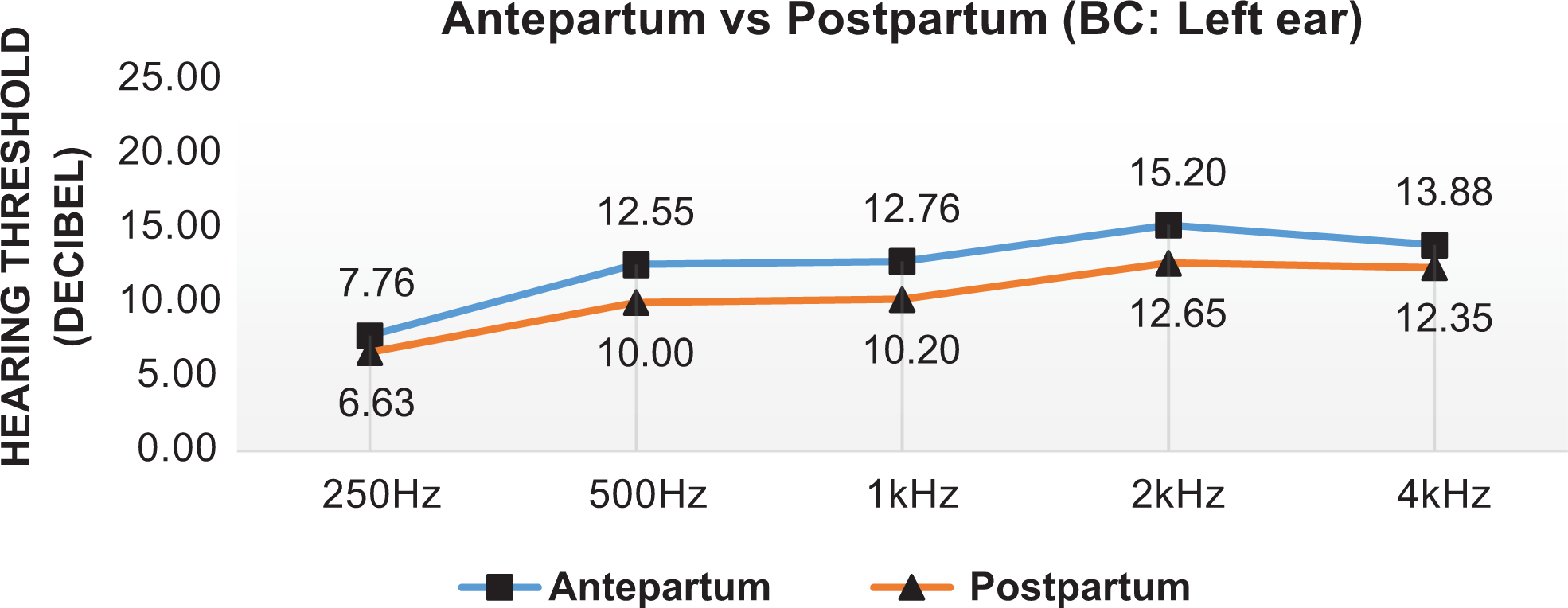
Bone conduction hearing threshold: Left ear (Antepartum vs postpartum).
Average of AC Threshold Values at 0.5, 1, and 2 kHz (Antepartum vs Postpartum).
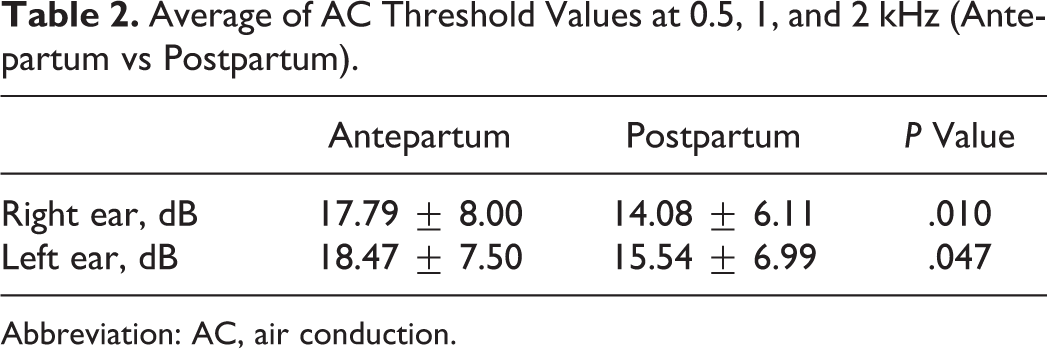
Abbreviation: AC, air conduction.
Impedance audiometry was done for both ears, during antepartum and 6 weeks postpartum. The right ear showed type A curve for the majority of the patients in the antepartum period (92.75%) while in the postpartum period, the percentage changed to 97.87%. A similar pattern was observed for left ear as well (Table 3).
Impedance Audiometry (Tympanogram).
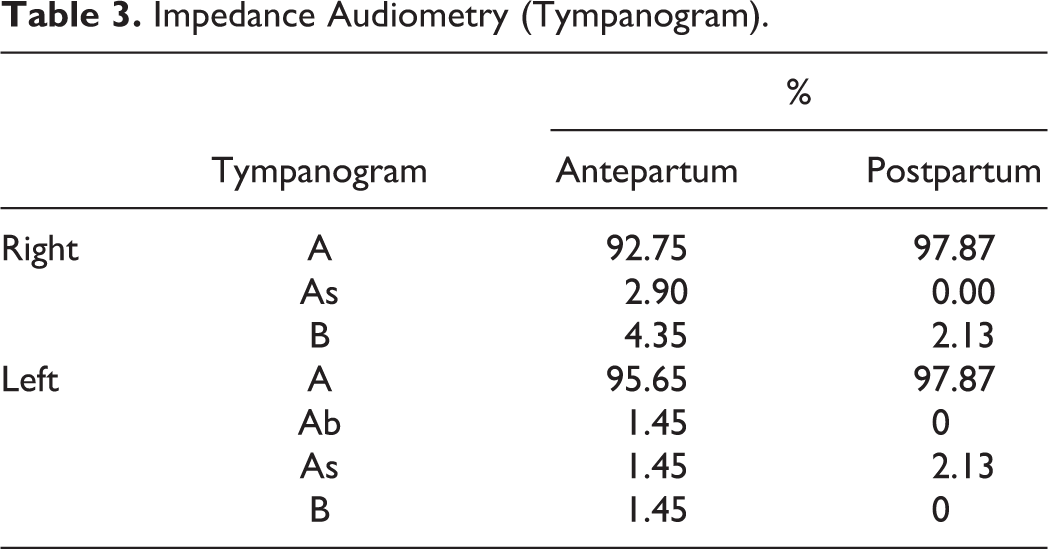
The presence of acoustic reflex was also checked in all the patients, and the number of cases and controls showing presence of reflex increased from 68.12% to 78.72% for right ear. A similar change was seen for left ear where the percentage of patients with reflexes present increased from 69.57% to 80.85%.
Discussion
Hearing loss is a major health problem affecting the quality of life and performance at workplace. Most important causes of hearing loss are presbycusis, followed by noise exposure, ototoxic drugs, and viral infections. 17
We observed that the hearing threshold values showed an improvement postdelivery, with some of the changes being statistically significant. The main observation of the study was a decrease in the hearing threshold values postdelivery. Although the difference in AC threshold values was statistically significant (P value < .05) at 500 Hz and 1 kHz, it could not be categorized as hearing loss as per WHO standards. These findings are in-line with the results obtained by Sennaroglu and Belgin who claimed that there is a decrease in low frequency hearing level during pregnancy. 7 We also observed that the changes were significant only at low frequencies. The average hearing level calculated by taking the average of AC threshold values at 500 Hz, 1, and 2 kHz also showed change in the hearing level for both the ears, which was statistically significant but within normal limits of hearing. Tsunoda et al investigated ear problems in a group of pregnant women and found that PTA and impedance audiometry showed normal hearing in all cases. 16 However, they did not mention the findings at different frequencies, which was addressed in our study. The low tone hearing threshold shift mimics the pattern seen in Meniere disease but in pregnancy, the values remain within normal limits. The cause of the abovementioned change can be due to salt and water retention which is seen during pregnancy. Similar to the changes seen in PTA, we also observed changes in impedance audiometry in which we observed that the percentage of patients having type A audiogram increased. Tsunoda et al had shown similar results which can be explained based on the fact that changes in pregnancy like fluid retention take place gradually resulting in adaptation of the body which prevents collapse of eustachian tube opening. 16
In conclusion, it can be suggested that pregnancy is associated with changes in hearing threshold level which though significant and are not severe enough to be called as hearing loss. More studies with larger sample size will help us in a better understanding of this topic.
Footnotes
Authors’ Note
An informed consent was taken from all the participants in the study, duly signed in the presence of a witness.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.