
Abstract
Background:
Otosclerosis is a disease of the osseous labyrinth. The disease causes 5% to 9% of all cases of hearing loss and 18% to 22% of conductive hearing loss. The treatment of choice is a surgery. The hearing improvement after the operation is determined by various factors.
Aims/Objectives:
The aim of the analysis is to determinate changes in hearing after stapedoplasty in view of surgery side in the patients operated on otosclerosis by right-handed surgeons.
Material and Methods:
The analysis involved patients hospitalized and operated on otosclerosis between 2012 and 2018. Only patients with their first middle ear surgery due to otosclerosis were included in the study. The patients were operated by 2 right-handed surgeons who used the same surgical technique and had similar experience in otosclerosis surgery. The study included patients who were divided into 2 groups: with self-tightening prosthesis and with manually tightening prosthesis.
Results:
The procedure performed by right-handed operators on the left side using prostheses requiring manual fixation on the incus was associated with poorer audiometric results compared to the results of surgeries on the right side. In patients with the self-tightening prostheses, the audiometric improvement of hearing was bilaterally comparable independently from operation side.
Conclusion:
(1) The dependence of hearing improvement on the surgery side was demonstrated in cases of surgeries performed on the left ear by right-handed surgeons, particularly with manually tightening prosthesis. (2) Self-tightening prostheses in stapedotomy limit the human factor, reducing the risk of complications after otosclerosis surgery and provide repeatable hearing improvement.
Keywords
Introduction
Otosclerosis is a disease of the osseous labyrinth, caused by abnormal bone homeostasis. The disease causes 5% to 9% of all cases of hearing loss and 18% to 22% of conductive hearing loss. The prevalence in the European population is 0.3% to 0.4%. Women develop the disease twice as often as men. The disease can be genetically determined, it can be the result of a measles virus infection, biochemical, immunological, and hormonal disorders.
The treatment of choice in otosclerosis is a microsurgery of the ear—stapedotomy, aimed to restore the 2-window hearing. Stapedotomy leads to hearing improvement in more than 90% individuals. Results of surgery in the course of otosclerosis depend on, for example, bone conduction thresholds, air-bone gap (ABG) values. Stapedotomy decreases conductive component of hearing loss and increases contribution of middle ear in bone conduction (Carhart’s effect). In hearing improvement after stapedotomy, no less important is a human factor, strongly dependent with surgeon. Precision and repeatability play important role to achieve the best results and avoid complications.1,2
The purpose of the study is to present results of stapedotomy depending on operation side in procedures performed by a right-handed operator.
Methods
The analysis involved patients hospitalized and operated on between 2012 and 2018. Only patients with their first middle ear surgery due to otosclerosis were included in the study.
The study included patients who were divided into 2 groups A and B, based on the type of prosthesis used in the course of surgery, and then divided into subgroups in terms of the operated side (Table 1): – Group A (N:160 persons) operated between 2012 and 2018 using a prosthesis made of polytetrafluoroethylene piston permanently connected to a platinum element: a 0.1-mm diameter wire, and the need to tighten the clip with microforceps after placing a long process of incus. – Group B (N:35), who underwent surgery in the years 2017 to 2018, who had a self-tightening prosthesis of titanium placed during the surgery.
Subgroups of Patients Depending on the Type of Prosthesis and Operated Side.
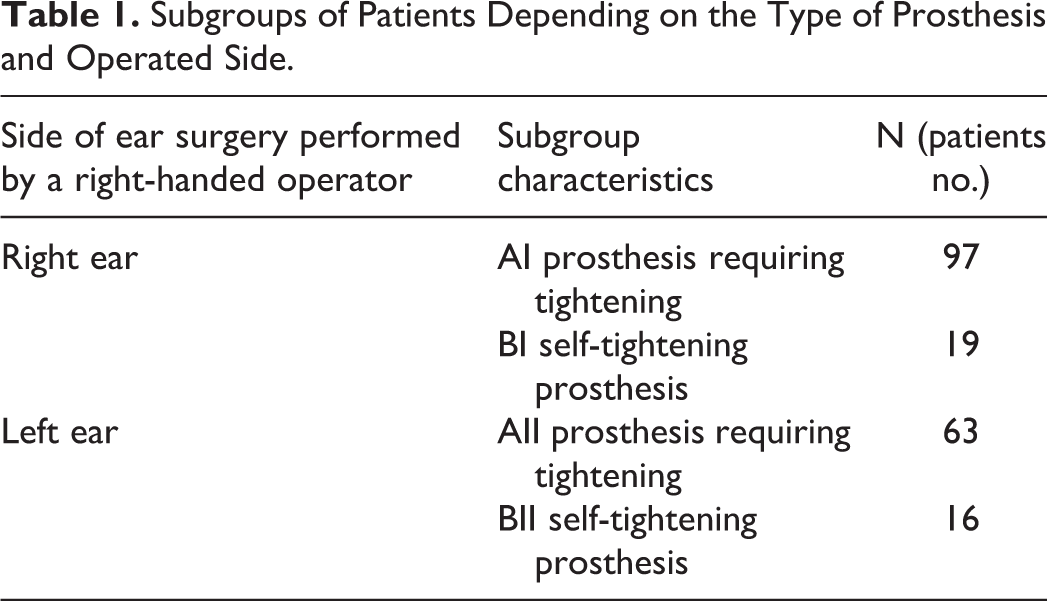
The analysis was performed in a comparative manner covering patients from each of the created subgroups broken down between operation sides and type of prosthesis (AI, AII, BI, BII). All operated patients were subject to a follow-up with a 1-year time interval.
The patients were operated by 2 right-handed surgeons who used the same surgical technique and had similar experience in otosclerosis surgery. The surgeons evaluated in the study performed surgery due to otosclerosis 2 to 3 times a week. Each one had at least 15 years’ experience in middle ear surgery and 10 years’ experience in the stapes surgery.
Each surgeon informed that in everyday activity and during surgery observe a distinct advantage of the right hand when operating in subtle maneuvring.
The stapedotomy procedure consists in removing the suprastructure of the stapes and making a small aperture in the plate into which a piston-type prosthesis is inserted, suspended on a mobile incus.
In this study, we were looking for the answer to the question whether the surgery result is related to the side operated by right-handed operators. Whether the precision of the surgery is the same on the right and left side, especially at the stage of standard attachment of the prosthesis to the incus and tightening the element on the long process of the incus, comparing the right and left ears in case of right-handed surgeons.
In all patients, an otorhinolaryngological interview and physical examination, as well as a set of audiological tests were performed, including acumetric examination, tuning fork tests, and pure tone audiometry.
In the presented study, the mean ABG and mean bone conduction thresholds value were calculated as the arithmetic mean for speech frequency (500, 1000, 2000, and 4000 Hz) before and 12 months after the surgery. 3 Subsequently, changes in postsurgical value of the mean bone conduction changes and mean postsurgical value of the ABG were calculated for discussed frequencies. The data obtained during the study work were analyzed statistically.
The first test used to analyze hearing improvement was the Fisher exact test, also known as the variance analysis test in the literature. In this study, the null hypothesis means that the mean values of the parameters concerned are statistically equal. The alternative hypothesis is the inverse statement that the mean values are not equal. The test of multiple-field contingency tables—the c2 test—was used to verify nonparametric hypotheses.
The strength of the relationship is shown using the Cramér’s V, the value of which is always between 0 and 1. In this study, the significance level of 5% (α = .05) was assumed to be sufficient, meaning that the risk of error in rejecting the hypothesis in case it is true is 5%. Statistically significant results were provided for P < .05. 4
The Ethics Committee approved the study. The informed consent was reached from each individual included to the study.
Results
In the analysis of variance after the treatment, the following results of changes in mean ABG were obtained, P < .05 (Tables 2 and 3).
Change in Mean Air-Bone Gap (ABG) for the Right and Left Ear in Groups AI and AII.

Abbreviations: ΔABG 12, change in the air-bone gap 12 months after surgery; F quotient, variance quotient; LE, left ear; N, group size; P, significance level; RE, right ear; SD, standard deviation; t, result of Student t test.
Change in Mean Air-Bone Gap (ABG) for the Right and Left Ear in Groups BI and BII.

Abbreviations: ΔABG 12, change in the air-bone gap 12 months after surgery; F quotient, variance quotient; LE, left ear; N, group size; P, significance level; RE, right ear; SD, standard deviation; t, result of Student t test.
Group A was statistically significantly different from the results of changes in the mean ABG between the right and left ear. The mean ABG in group A II for the left ear was statistically inferior compared to the mean value for the right ear (AI). The same analysis in patients from group B did not show any statistical difference between subgroups (BI, BII).
The following results were obtained by analyzing changes in the mean bone conduction thresholds value after 12 months of follow-up, depending on the operated side for 500, 1000, 2000, and 4000 Hz frequencies in groups A and B (Tables 4 and 5).
Change in the Mean Bone Conduction Thresholds Value for the Right and Left Ear in Groups AI and AII.
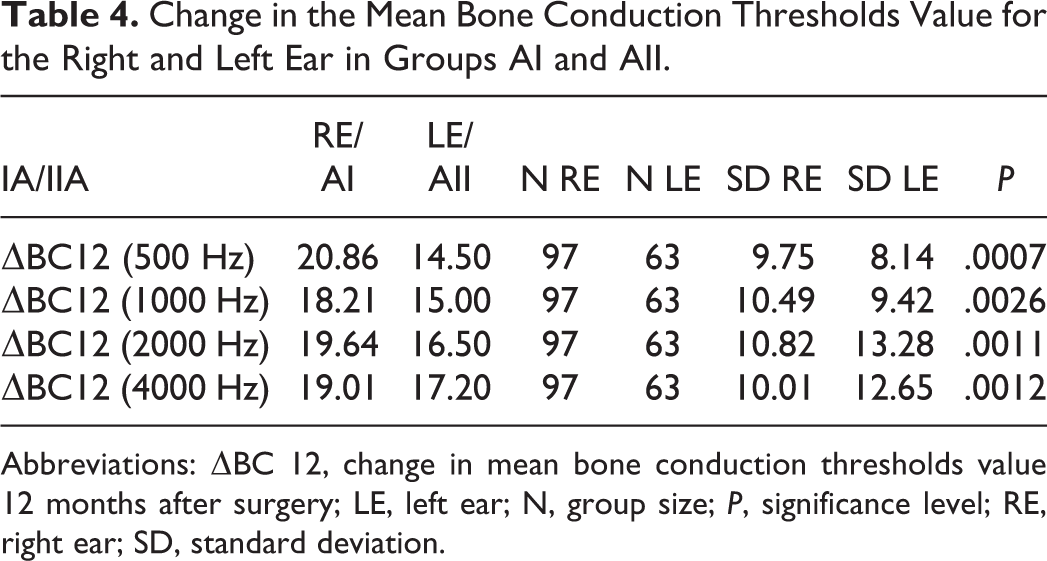
Abbreviations: ΔBC 12, change in mean bone conduction thresholds value 12 months after surgery; LE, left ear; N, group size; P, significance level; RE, right ear; SD, standard deviation.
Change in the Mean Bone Conduction Thresholds Value for the Right and Left Ear in Groups BI and BII.
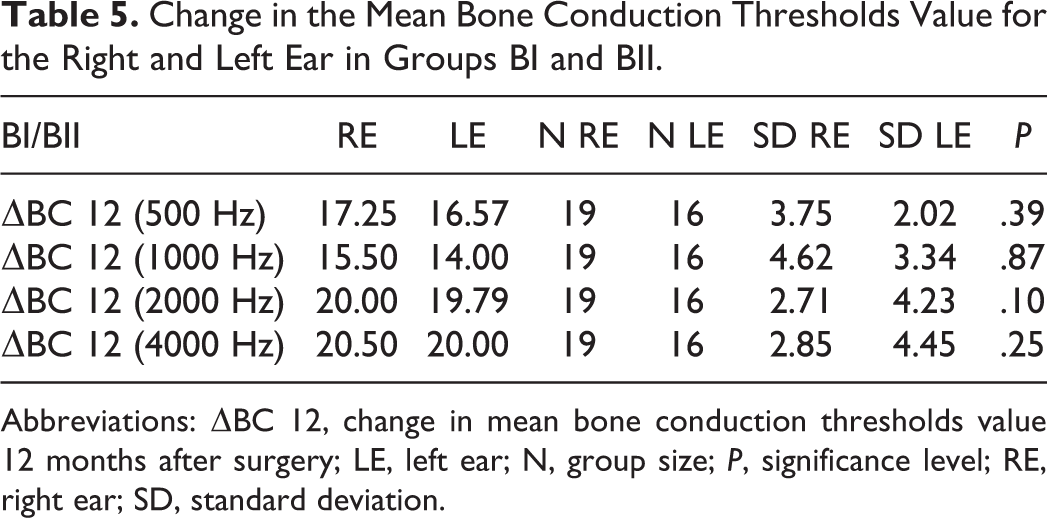
Abbreviations: ΔBC 12, change in mean bone conduction thresholds value 12 months after surgery; LE, left ear; N, group size; P, significance level; RE, right ear; SD, standard deviation.
A statistical difference was found in groups AI and AII between the change values of mean threshold bone conduction values for frequencies 500, 1000, 2000, and 4000 Hz and the right and the left ear. The change in the mean threshold bone conduction value for the left ear was statistically lower than the mean for the right ear. No statistical difference was observed in patients in group B (BI, BII). The change in the mean bone conduction thresholds value between the right and left ear was statistically equal within these groups 12 months after the surgery.
Discussion
Immobilizing the base of the stapes in the otosclerosis reduces the intensity of the acoustic signal reaching the nervous and sensory system causing hearing loss. According to the current state of knowledge, a correctly performed surgery is one effective treatment method for otosclerosis.5-7 Currently used prostheses are piston-type. Stimulation of the cochlea with a traditional piston prosthesis is not perfect.8-10 The main disadvantage of such a prosthesis is the generation of too weak pressure wave in the perilymph. This is due to the approximately 16 times smaller surface area of the vibrating piston (∼0.2-0.3 mm2, ø: 0.4/0.6 mm) compared to the surface area of the stapes plate (∼3.2 mm2). Piston-type prostheses available for otosurgeons can be fixed by operators by manually tightening the loop on the long process of the incus or using a self-tightening element.11,12 The stapes prostheses are self-tightening, being retained on the long process of the incus, and thanks to this structure, the clamping stage—one of the most difficult and unpredictable stages of stapes plastic surgery—is eliminated.
The standard attachment on the incus, with no “dangerous tightening,” seems to make the operation principle of the self-tightening element the optimal solution. Prostheses made of the so-called shape-memory alloys, meaning those susceptible to curing with laser light, seem to be an alternative, currently in the phase of initial tests. This material allows for more precise attachment of the prosthesis, the so-called fixation. There are some controversies raised by nickel—considered to be toxic to the inner ear—which is the material used in the composition of the prosthesis.13,14 Other authors characterized self-crimping prostheses as very friendly for the surgeons with low rate of intraoperative complications. In those studies described, audiological results were similar as for cases with manual fixation of the prosthesis.15-17
In our observation, the procedure performed by right-handed operators on the left side using prostheses requiring manual fixation on the incus (group A) was associated with poorer audiometric results compared to the results of surgeries on patients in group B (using the self-tightening prosthesis).
According to available literature, there are no functional differences in results of surgeries in the course of otosclerosis when comparing right and left side. Some otosurgeons preferred precise stapedotomy on the side of their dominant hand as more comfortable than on the opposite side. 18 Preliminary reports show audiometric results poorer in cases with stapedotomy using manually tightening prostheses on the opposite side than surgeon’s dominant hand. Above observation was not confirmed in individuals with self-tightening prostheses that decreased negative impact of human factor on audiometric result in mentioned step of otosurgery. In discussed study, group of patients with self-tightening prostheses was small and require further analysis.
The results of the study allow us to point out that the postoperative results obtained in patients with otosclerosis, discussed in numerous studies by other authors, are influenced not only by the optimal selection of patients for surgery, the type of sealing of the oval window niche, length, diameter, and weight of the fitted prosthesis (low-weight prostheses transmit high-frequency sounds well, whereas heavier prostheses transmit low frequencies better), but also by availability and precision at the prosthesis fixation stage on the long process of the incus. 19
The foregoing observations included in the results illustrate the dependence of hearing improvement on the surgery side in case of surgeries performed on the left by right-handed surgeons, particularly at the prosthesis tightening stage, and the precision of performing this surgery part on the left. At the same time, this limits the human factor, thus reducing the risk of complications and failures after otosclerosis surgery (Figure 1).
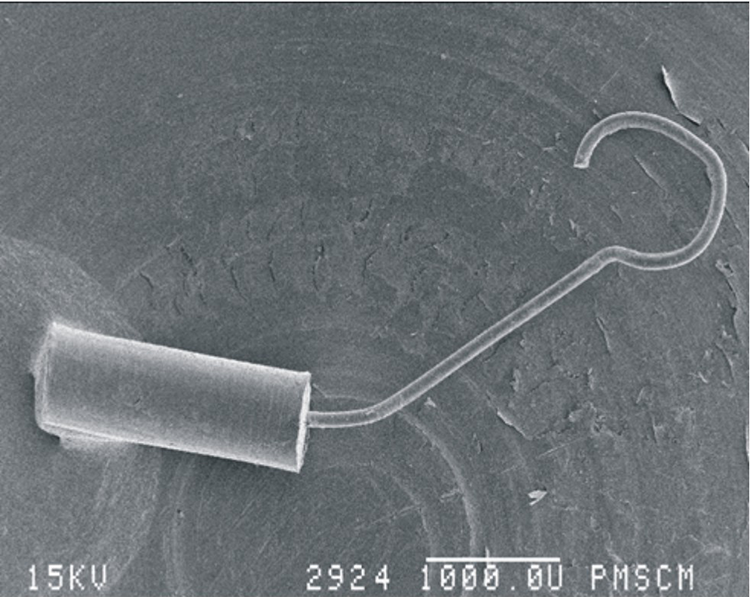
Image of a piston-type prosthesis removed from the middle ear space. The prosthesis slipped from the long process of the incus on a distant day after surgery, magnification ×22.
This conclusion is original and very important from a practical point of view for right-handed surgeons and should be confirm by further studies.
The authors recommend use of a self-tightening prostheses for right handed surgeons during left-sided stapedotomy. If this is not accessible, the authors suggest performing surgery on the left ear as the first procedure of the day, to reduce fatigue and its negative impact on surgical precision.
It is also important to provide correct support for the left hand to ensure the highest degree of precision possible. The surgeon should attach the prosthesis to the incus as the first maneuver during prosthesis placement.
Conclusions
The dependence of hearing improvement on the surgery side was demonstrated in cases of surgeries performed on the left ear by right-handed surgeons, particularly with manually tightening prosthesis.
Self-tightening prostheses in stapedotomy limit the human factor, reducing the risk of complications after otosclerosis surgery and provide repeatable hearing improvement.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by statutory funds of the Department of Otolaryngology of the Jagiellonian University, Krakow, Poland.