
Abstract
The study is aimed to assess the scope of endoscopic stapedotomy in overcoming technical challenges faced during conventional stapedotomy using operating microscope. Sixty-four patients with clinical and audiological diagnosis of otosclerosis were randomly assigned into one of the 2 groups—one underwent conventional stapedotomy using operating microscope, while the other group underwent endoscopic stapedotomy, the operating surgeon being the same for both groups, for all cases. The 2 groups were observed in terms of extent of the postero-superior canal bone curettage/drilling, chorda tympani repositioning, visualization of footplate area, surgical time from first incision to ear packing, post-operative morbidity in terms of post-operative pain, vertigo, hearing outcome, and changes in taste sensation. It was observed that irrespective of the width of the external auditory canal, endoscopic approach offered better access to the footplate area requiring lesser bone removal and chorda tympani repositioning. The operating time, post-operative pain, and changes in taste sensation were significantly less in the endoscopic group. However, no difference was noted in terms of the post-operative hearing outcome and incidence of vertigo. Endoscopic stapedotomy has clear advantages in terms of the technicality and accessibility to the working area as well as faster recovery.
Introduction
Stapedotomy has been practiced as a surgical modality for the treatment of otosclerosis. The conventional tool for the surgery has been the operating microscope. The operating microscope renders the surgeon the advantage of use of both hands for instrumentation and hence greater stability which is of utmost importance in a surgery as delicate as stapes surgery. However, it has certain limitations. The field of view through an operating microscope is narrower as compared to an endoscope. This is because the focal length of the operating microscopes commonly used in otology is around 250 mm. This essentially has a number of implications. Certain working areas that do not lie directly in the line of our visual axis cannot be readily visualized by microscope. This means any tissue lying in front has to be repositioned or removed to ensure adequate visualization. This adds to the operative morbidity and longer operating times. 1,2 This study aims to assess the role of endoscopes in stapes surgery in overcoming the technical limitations faced with operating microscopes.
Patients and Methods
Patient Selection and Inclusion Criteria
Sixty-four patients diagnosed to have otosclerosis were included in this randomized controlled trial. The inclusion criteria were a history of progressive hearing loss in both ears without any ear discharge or past history of ear surgery, otoscopy within normal limits, conductive hearing loss with an air–bone gap more ≥30dB on pure tone audiometry, absent stapedial reflex, a normal anatomy, and absence of middle ear pathology on High Resolution Computed Tomography scan of temporal bone. Those patients with history or clinical evidence of middle ear disease or surgery or an only hearing ear were excluded. The selected patients were randomly assigned into 2 groups—one undergoing stapedotomy using conventional operating microscope and the other by endoscopic approach. The randomization sequence was generated by table of random numbers and allocation was concealed using sealed opaque envelopes. The details of the procedure were explained and written informed consent was obtained. However, the patients were not aware of the exact technique of surgery (endoscopic/microscopic) they underwent.
Surgery
All the cases were done by the same operating surgeon, using Zeiss operating microscope and Karl Storz (4 mm diameter, 18 cm length) rigid endoscopes (0°, 30°). The operative steps followed were the same in both groups, apart from a few additional modifications for the endoscopic approach. The surgeries were carried out under local anaesthesia with 2% lidocaine with adrenaline (1:1 00 000). Four quadrant infiltration was given. Incision was made 4 mm lateral to the annulus and curved superiorly just anterior to the lateral process of malleus. The incision was extended inferiorly up to 6-o’ clock position. Tympanomeatal flap was gently raised till the level of the annulus. Use of cotton balls soaked in undiluted adrenaline at this stage helps in flap elevation, ensures flap protection from suction damage, and minimizes bleeding and soiling of the scope in case of endoscopic approach. Upon reaching the annulus, careful dissection is done so as to identify and preserve the chorda tympani nerve. Endoscopes, especially 30° (Karl Storz 4 mm diameter, 18 cm length), usually provided a clear view of the working area that includes the pyramidal eminence, stapedius tendon, incudostapedial joint, footplate area, and horizontal portion of facial nerve, minimizing the need of bone work involving the postero-superior canal wall. Bone curettage/drilling of the postero-superior canal was however necessary in case of microscopic approach to aid visualization. Minimal manipulation of chorda tympani was done as far as practicable. Diagnosis was confirmed intraoperatively by gentle palpation of the ossicles with a fine-tipped microinstrument. In cases of endoscopic approach, stapedius tendon was sharply cut with a 45° curved micro-scissors and incudostapedial joint dislocated thereafter. Posterior crus was sharply cut and anterior crus gently fractured to deliver out the stapes. We could readily access these difficult areas using long, curved pick in endoscopic stapedotomy, even when the postero-superior canal was completely intact. A control fenestra was made over the posterior third of the footplate. In difficult situations with extremely hard footplate, contra-angled handpiece with 0.8 mm diamond burr was used to drill the footplate area. Thereafter, the fenestra was enlarged and a 0.5 mm Teflon stapes piston was fitted and crimped in all cases. Soft tissue seal obtained from a small post aural puncture wound was used to plug the fenestra. Tympanomeatal flap was repositioned back in its place. Gelfoam was placed in the canal to stabilize the flap. Routine post-operative medications were given. Oral paracetamol was used for post-operative analgesia in all patients.
Study Parameters and Result Analysis
The parameters documented in the 2 groups were extent of the postero-superior canal bone curettage/drilling, chorda tympani repositioning, visualization of the footplate area, surgical time from first incision to ear packing, post-operative morbidity in terms of post-operative pain by Numerical Rating Scale, vertigo, hearing outcome, and changes in taste sensation.
We have classified the view of incudostapedial complex from the margin of the annulus into 4 groups (Figure 1):

Schematic representation of grades of visibility of the incudostapedial complex.
Grade I = Only I-S joint is visible
Grade II = I-S joint + Stapedius (partial)
Grade III = I-S joint + Stapedius (complete)
Grade IV = I-S joint + Stapedius (complete) + Pyramidal eminence (till base)
We have measured the extent of postero-superior bony wall removal with the help of picks of various sizes (2, 3, and 4 mm). The measurement was done between the incudostapedial joint and posterior canal wall. The results were classified into 4 categories depending upon the amount of bone removed: I (0 to <2 mm), II (2 to <3 mm), III (3 to <4 mm) and IV (≥4 mm).
Hearing results were calculated from air and bone conduction thresholds measured pre- and postoperatively at 500, 1, and 2 kHz for all patients. Subjective vertigo and change in taste sensation experienced by the patients at the end of first week and 4 weeks postoperatively, respectively, were documented.
Data were summarized as mean and standard deviation for continuous and median and range for ordinal variables and counts and percentages for categorical variables. Paired t test was done for paired samples which are normally distributed. P value ≤.05 was considered statistically significant.
Results
Demographic Characteristics
Sixty (93.75%) patients were females and the rest were males. Mean age of the patients in the endoscopic group was 40 years, while that in the microscopic group was 38.5 years.
Extent of Postero-superior Canal Wall Removal
This was classified into 4 categories depending on the amount of bone removed: I (0 to <2 mm), II (2 to <3 mm), III (3 to <4 mm), and IV (>4 mm); 62.5% (20/32) of the patients undergoing microscopic stapedotomy belonged to class IV, requiring >4 mm of the postero-superior canal wall bone to be removed for adequate exposure, while 68.75% (22/32) of the patients of the endoscopic stapedotomy group belonged to class I, requiring <2 mm of bone removal (Figure 2).
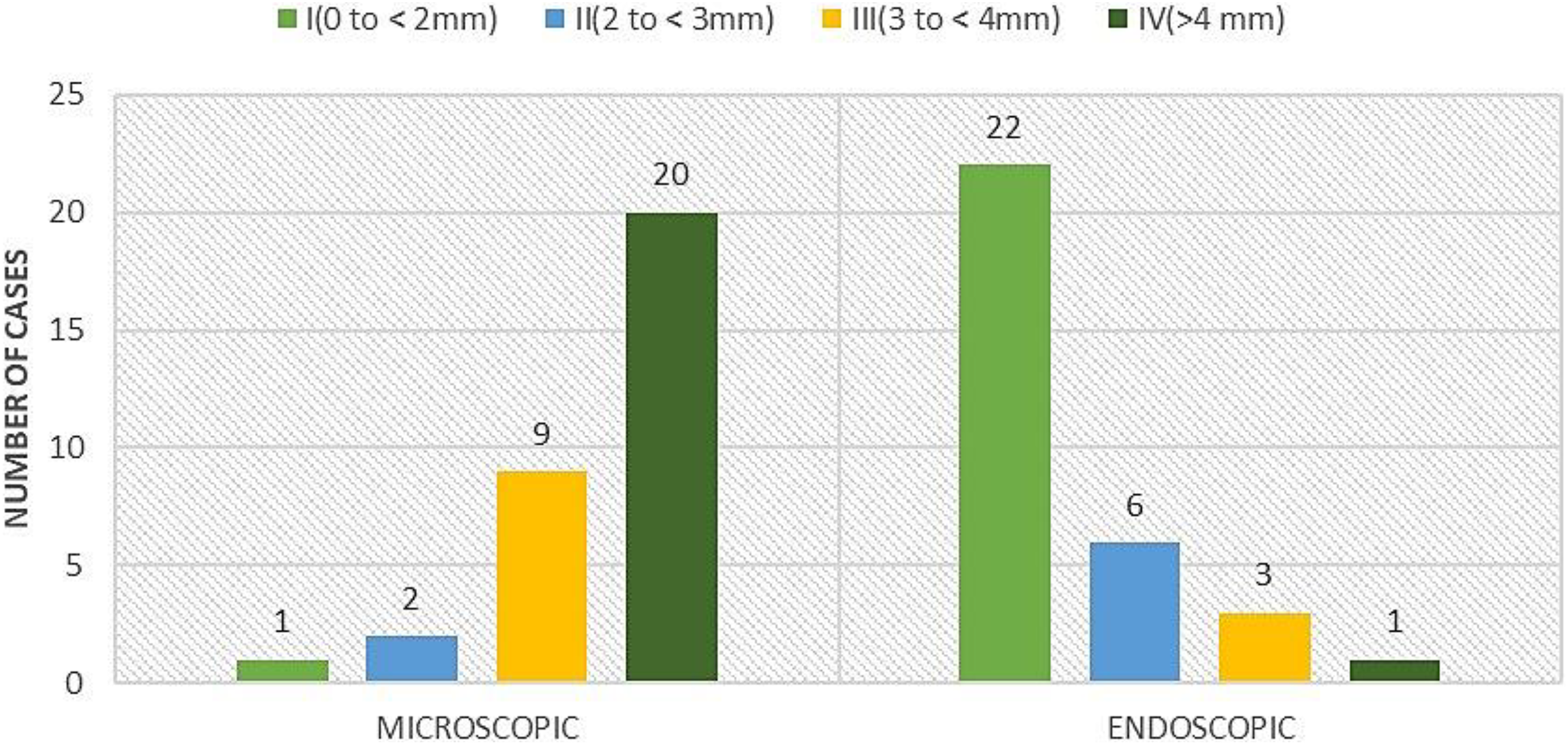
Graphical representation of the extent of postero-superior canal wall removal.
Chorda Tympani Handling
Minimal handling of the chorda tympani nerve was required in 81.25% (26/32) of the patients during endoscopic stapedotomy, while 93.75% (30/32) of the patients required moderate to extensive chorda manipulation during microscopic stapedotomy.
Visibility of Incudostapedial Complex
Anterior crus of stapes was visible in none of the patients in the microscopic group, while in 87.5% (28/32), it was clearly visualized, especially with the use of a 30° endoscope. 78.12% (25/32) of the patients undergoing surgery using microscopic technique were found to have grade I visibility, whereas 75% (24/32) of patients belonging to endoscopic group had grade III visibility (Figure 3).
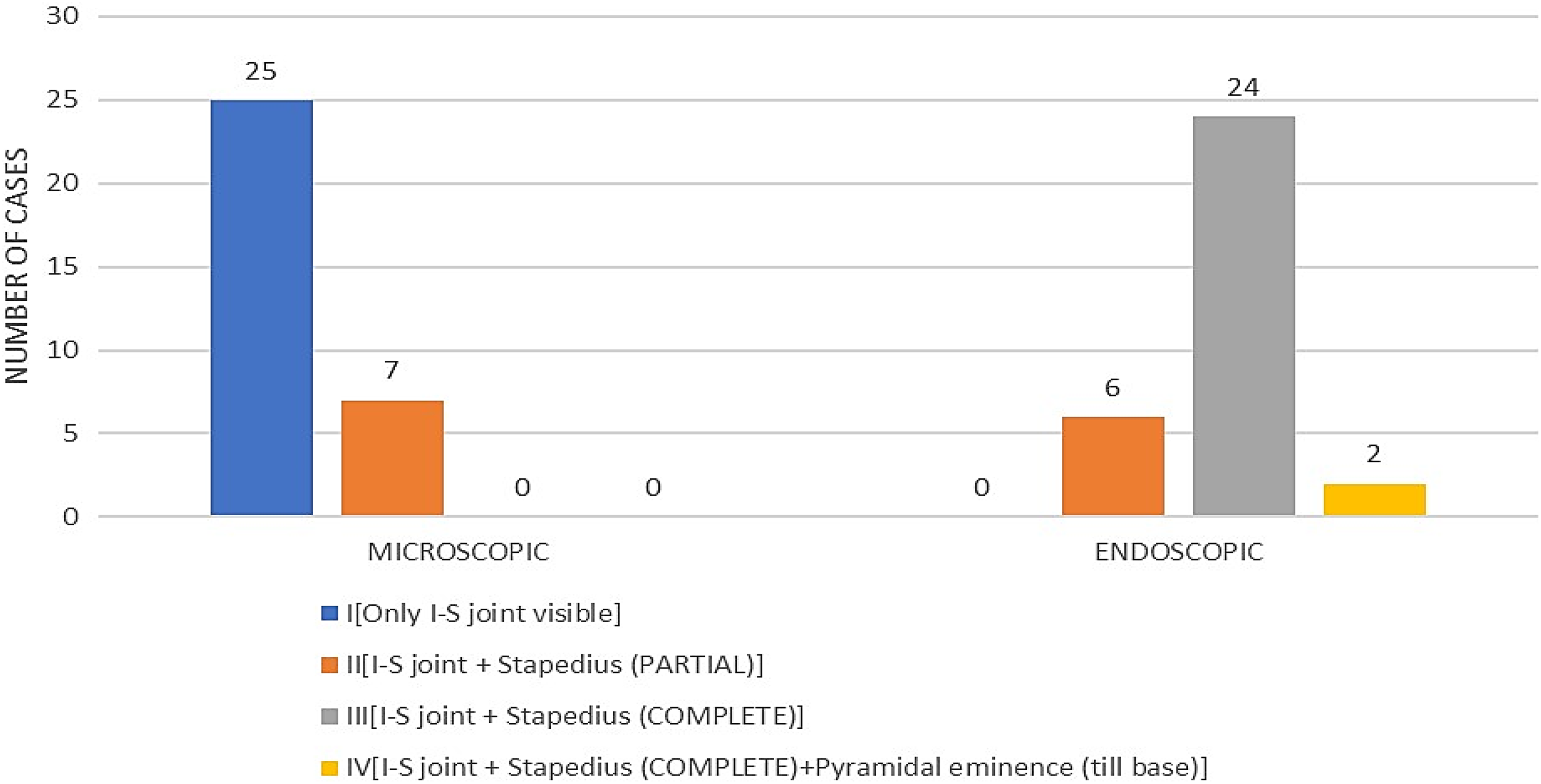
Graphical representation of grades of visibility of the incudostapedial complex.
Mean Surgical Time
In the endoscopic group, stapedotomy was 56.03 ± 3.45 minutes while that for microscopic group was 87.87 ± 4.31 minutes. This was found to be a statistically significant value (<.05; Table 1).
Mean Surgical Time in Minutes, Mean Post-operative Air–Bone Gap, and Post-operative Taste Change.
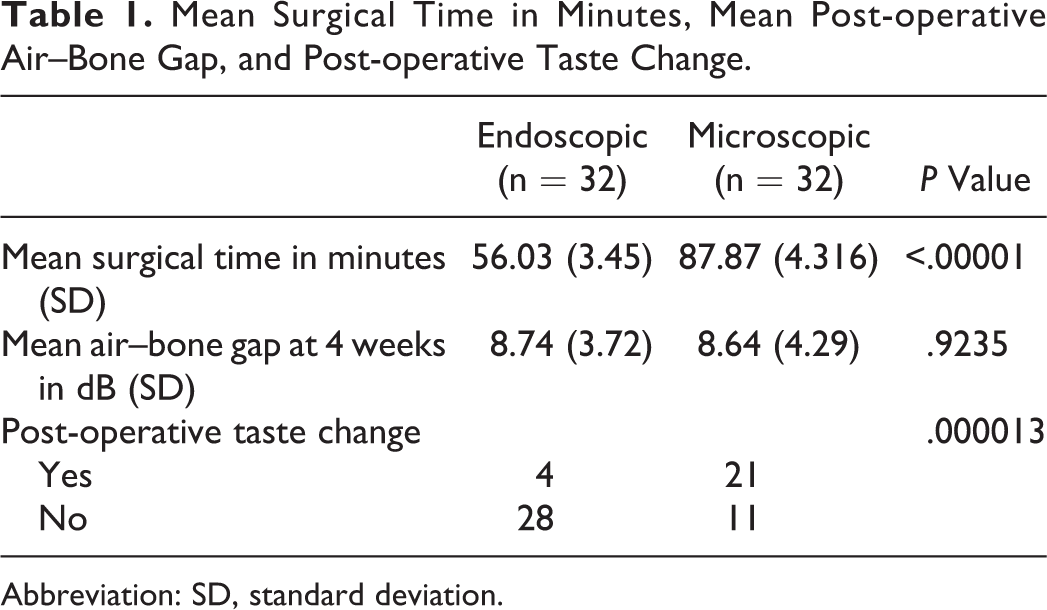
Abbreviation: SD, standard deviation.
Post-operative Pain
In both groups, post-operative pain was assessed using the Numerical Rating Scale at 6 hours postoperatively. The median pain score in the endoscopic group was 4 (range: 2-7) and that in the microscopic group was 6 (range: 4-8), and this was found to be statistically significant (P < .05; Figure 4).
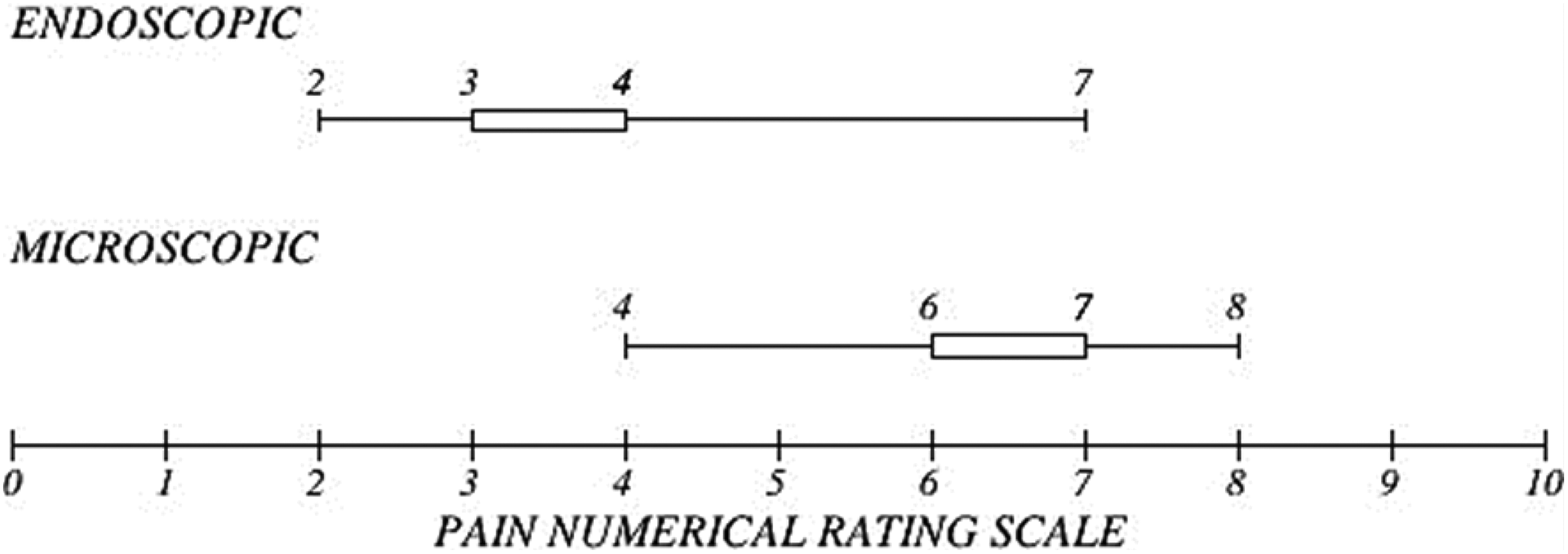
Graphical representation of post-operative pain score; lower (right) edge of the box depicts median pain score and the whiskers depict the range (minimum to maximum pain score from left to right).
Air–Bone Gap Closure and Post-operative Vertigo
However, no significant difference was found between the 2 groups in terms of vertigo experienced by the patients at the end of first week and the air–bone gap closure between the 2 groups when followed up at the end of 4 weeks postoperatively (Table 1).
Alteration in Taste Sensation
Of 32, 21 (65.62%) patients of the microscopic stapedotomy group reported change in their taste sensation when followed up at the end of 4 weeks after surgery, whereas 12.5% (4/32) reported the same in the endoscopic group (Figure 5). This was found to be statistically significant (P = .000013; Table 1).
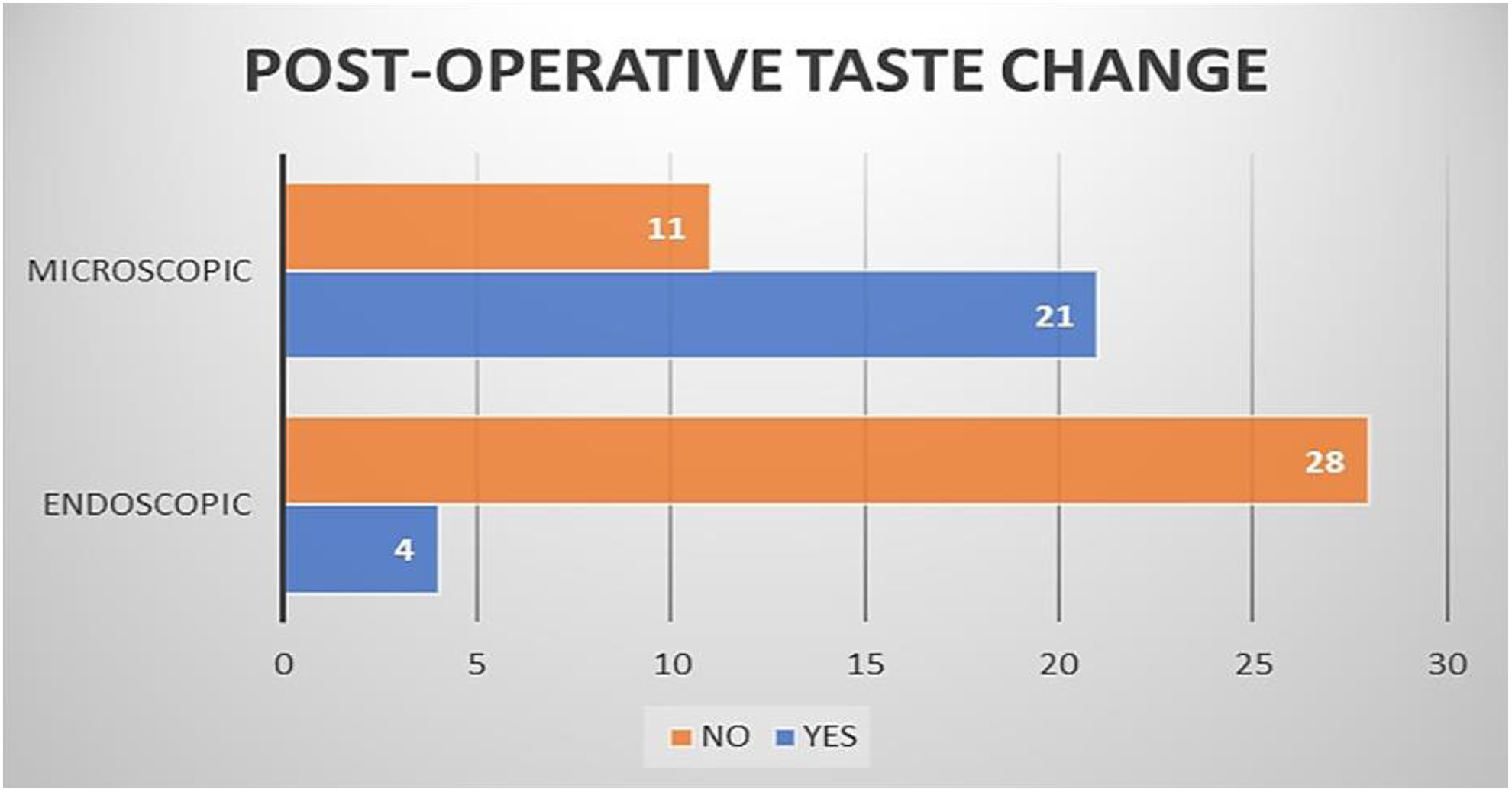
Graphical representation of post-operative taste change.
Discussion
Endoscopic ear surgery (EES) has evolved immensely over the past few decades. Endoscopes in middle ear surgery have made it possible to reach certain remote areas which were otherwise inaccessible via the straight axis vision of microscopes. Endoscopic ear surgery for cholesteatoma has been well-documented in the literature. 3 -5 However, the use of endoscopes in stapes surgery is a relatively new domain and hence not extensively explored yet.
The primary difference between stapes surgery and surgery for cholesteatoma is that most of the middle ear structures remain normal in case of an otherwise uncomplicated otosclerosis. Hence, any conservative surgical modality, without the need to disturb the rest of the structures, seems rational (Figure 6)
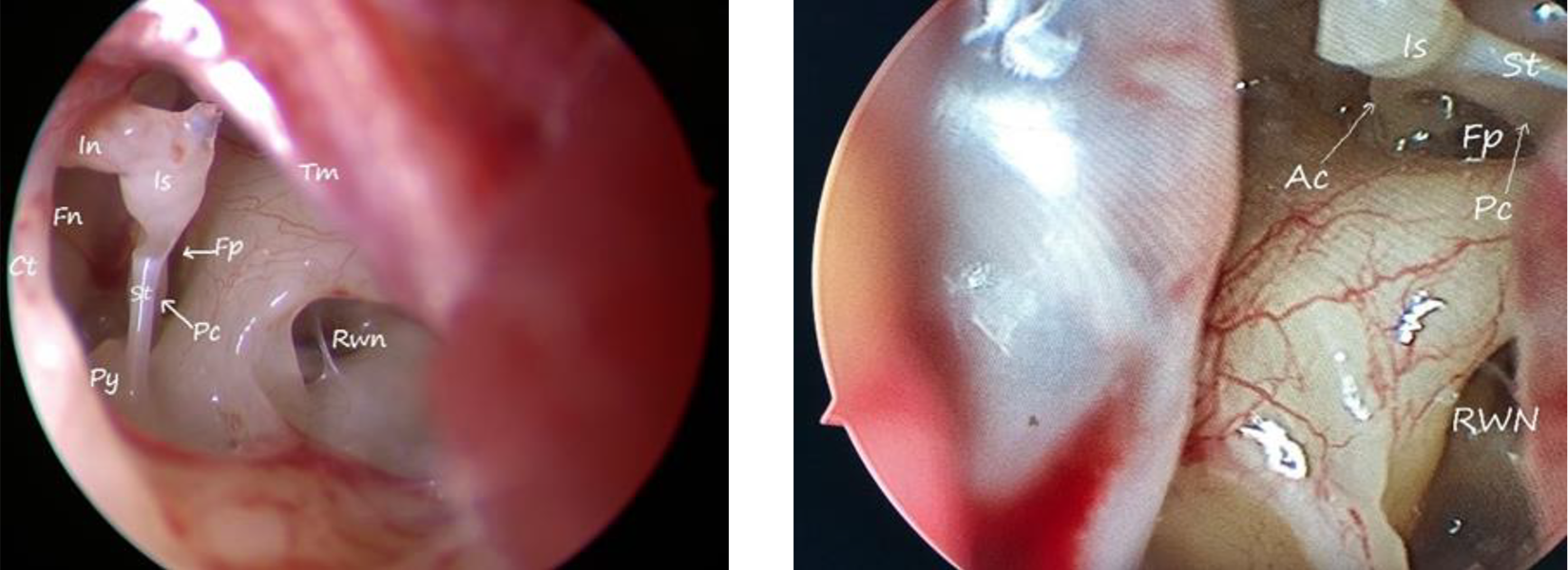
(Left to right): Endoscopic view of the middle ear. Ac indicates anterior crus; ct, chorda tympani nerve; fn, facial nerve; fp, footplate; in, incus; is, incudostapedial joint; pc, posterior crus; py, pyramidal eminence; rwn, round window niche; st, stapedius; tm, tympanic membrane.
In stapes surgery, the postero-superior bony canal wall often hinders the view of the middle ear working area and calls for bony canal wall removal for better visualization. However, with endoscopes, wider panoramic view is attained without sacrifice of any soft tissue lying ahead. The extent of postero-superior bony wall removal was measured with the help of picks of various sizes (2, 3, and 4 mm). This technique of measurement has been previously documented in the literature. 6 It was found that endoscopic stapedotomy required less bone removal. 7 This indicates that the incidence of complications associated with extensive bone curettage/drilling, for example, a possible iatrogenic trauma to ossicular chain and extensive chorda manipulation or decompression, was minimal. 8 -10
Extent of chorda tympani manipulation is another major issue in stapes surgery. In conventional microscopic stapedotomy, the chorda tympani is stretched inferiorly and further manipulation of the incudostapedial complex is carried out through the window that is created between the stretched chorda and the postero-superior canal wall. In endoscopic stapes surgery, this is not necessary as angled endoscopes (30°) provide wider panoramic view and use of angled instruments provides adequate access to the working area and avoids unnecessary chorda handling. 11,12
Adequate exposure is the key to any surgical procedure. In stapes surgery, visibility of the footplate area is of utmost importance to ensure precise insertion of the piston and minimal insult to the delicate inner ear structures. In cases of difficult anatomy, for example, overhanging facial nerve, access to footplate is more restricted in microscopic stapedotomy, which can be overcome by the use of angled scopes. We have classified the visibility of incudostapedial complex into 4 categories (as described previously). Such classification has not been documented before in literature. It was found that endoscopes, by virtue of their wide field of view, provide far superior visibility as compared to microscopes. The anterior crus of the stapes could be kept under direct vision while working with endoscopes, but this is rarely possible in case of microscopic stapedotomy. 13 This could potentially result in a blind fracture of the anterior crus (Figure 7).
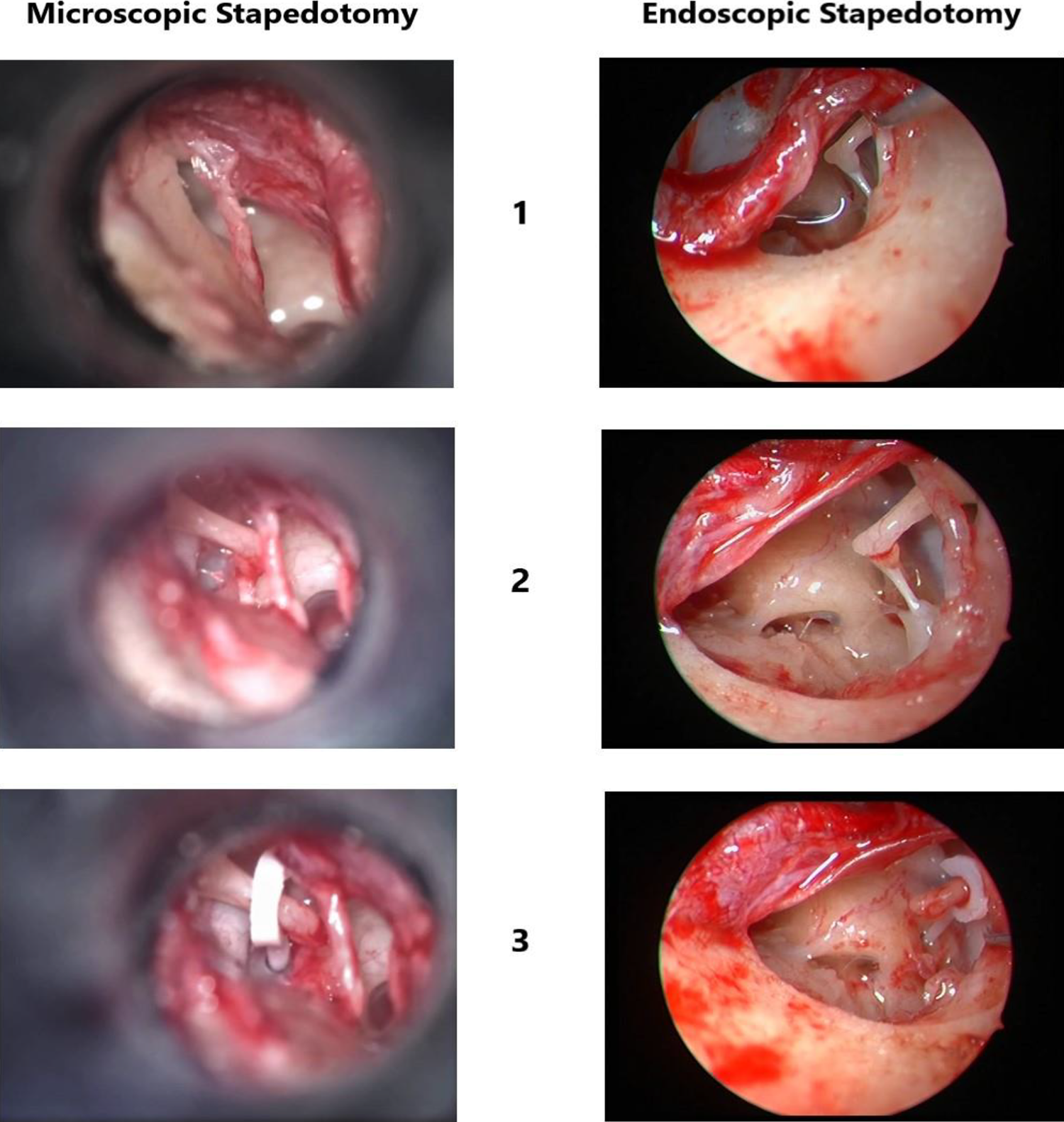
Comparison between microscopic and endoscopic stapedotomy—1: exposure after flap elevation; 2: after post-superior canal wall curettage; 3: final view after piston insertion.
In contrary to other studies, in our study, the surgical time taken was longer in microscopic stapedotomy than when performed with endoscopes. 7,14,15 This could possibly be attributed to greater time spent to curette/drill the posterior bony wall and more chorda maneuvering to obtain a clear field of view.
Regarding post-operative pain, it was found that the patients undergoing microscopic stapedotomy complained of greater pain post-operatively. Similar results were found by Hunter and Rivas and Harikumar and Arun Kumar. 15,16
In both the groups, the air–bone gap was closed to <10 dB postoperatively and no significant differences were found in this respect. Similarly, the subjective complaints of dizziness or vertigo as reported postoperatively at the end of the first week were same in both groups. These results were found to be consistent with that in the literature. 4,14,17
Alterations in taste sensation are frequently reported by patients undergoing stapes surgery. This is directly related to the extent of manipulation of the chorda tympani nerve during surgery. 12,18 This may range from minimal handling to even severing the nerve in difficult anatomical situations for the sake of access to the footplate area. However, this was rarely required; as in our study, in endoscopic stapedotomy, we used angled endoscopes, which provided a clear view of the working area when accessed from inferior to superior direction from the hypotympanum, and specialized angled instruments to perform the surgery. But this was not possible in the microscopic group, where chorda had to be manipulated as per the working conditions. And hence, post-operative taste change was reported to be higher in the microscopic group.
There are certain limitations to our study which include a small sample size and short follow-up period. Hence, certain differences may not appear significant even if they do exist. Moreover, there remains a possibility of a certain degree of bias as the surgeons could not be blinded.
Endoscopic stapedotomy, though seems to be at a better standpoint according to the chosen criteria, does have certain limitations. Microscopes owing to their binocular vision provides a better depth perception when compared to endoscopes. This is particularly important while working over the footplate area. However, with the advent of 3-D videoendoscopic systems, this may not be a limitation anymore. 19 Secondly, endoscopic surgery necessarily requires a blood-free clear working field; as this being a single-handed technique, concomitant suctioning of the working field is not possible. Moreover, in cases of massive bleeding obscuring the view or an intraoperative perilymph gusher, one may have to shift to a microscope or abandon the procedure. 20 Finally, stapes surgery itself being a surgery of precision and finesse, endoscopic stapedotomy has a steep learning curve and hence it may not be an appropriate surgery to start with for beginners. 21
Conclusion
Endoscopic stapedotomy appears to be a better alternative to conventional microscopic stapedotomy with advantages in terms of lesser bone removal, chorda tympani handling, better visibility of the footplate area, lesser operating time, less post-operative pain, and minimal post-operative taste alteration, provided the surgeon is well versed with conventional techniques and has sufficient expertise in EES.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.