
Abstract

A 50-year-old female presented with stable right-sided hearing loss of more than 6 months’ duration, noted during conversations. Otoscopy showed intact tympanic membranes bilaterally, with aerated middle ear spaces and no Schwartze sign. An audiogram revealed a right-sided moderately severe mixed hearing loss with a Carhart notch and a left low-frequency sensorineural hearing loss, with 88% discrimination on the right and 80% on the left. A contrast-enhanced magnetic resonance imaging (MRI) of the internal auditory canals was negative for any retrocochlear tumor. A temporal bone computerized tomography (CT) scan revealed a lucency in the fissula ante fenestram bilaterally, which led to the presumptive diagnosis of otosclerosis. Importantly, there was no evidence of an enlarged cochlear aqueduct or any communication between the fundus of the internal auditory canal and the vestibule. After discussion of her options, she chose to undergo a right transmeatal stapedectomy. Upon completion of the stapedotomy, a brisk cerebrospinal fluid (CSF) oozer was encountered, which was managed by placement of a Nitinol prosthesis with a secure crimp to the incus, followed by a circumferential tragal perichondrial graft, Gelfoam packing, and secure packing of the external canal. Neurosurgical consultation was obtained and a lumbar drain was placed for 3 days. She had initial vertigo which progressively improved, and she was discharged uneventfully.
During her office visits on postoperative days 5 and 11, she had no signs of CSF rhinorrhea but felt slightly off-balance. There was hemotympanum on the right side but no pulsations were noted. One month following surgery, she had no CSF rhinorrhea and no vertigo, but she did have some right clear otorrhea and felt that her hearing did not improve compared to prior to surgery. Her right tympanomeatal flap was elevated, bulging, and slightly pulsatile, and the right tympanic membrane itself was opaque, consistent with a middle ear effusion (Figure 1). At that point, it was presumed that there was a persistent CSF leak into the middle ear space from the stapedotomy and a middle ear exploration with revision repair of the fistula was planned, along with lumbar drain placement. However, the patient began to have less right otorrhea, and 7 days later, the patient returned to the office with cessation of the right otorrhea. Her right TM flap was minimally bulging and no longer pulsatile (Figure 2). Surgery was therefore deferred, and 3 weeks later, the patient returned with an upper respiratory illness which included rhinorrhea. However, the flap and the tympanic membrane were flat, with recovery of landmarks (Figure 3). She returned again a week later with her first postoperative audiogram which demonstrated closure of her air-bone gaps to within 5 dB, with 100% word discrimination. Eight months postoperatively, she returned for an audiogram which confirmed complete closure of the air-bone gaps at 1 and 2 kHz, still with 100% discrimination. Her right tympanic membrane had returned to normal appearance except for some displacement of the fibrous annulus (Figure 4).
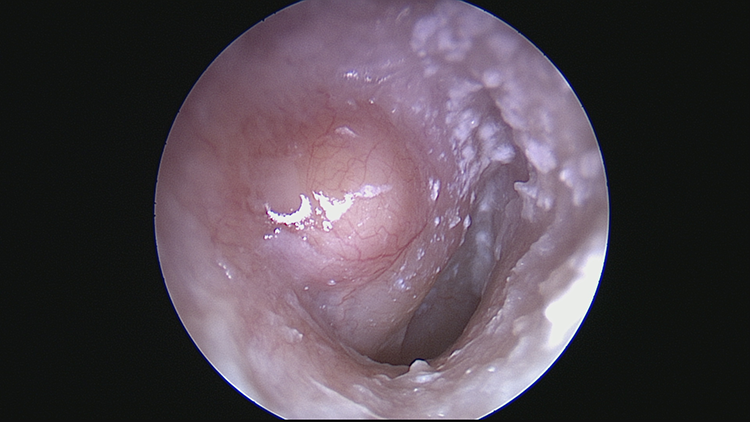
Right ear 1 month following surgery. The tympanomeatal flap was elevated, bulging, and slightly pulsatile. The right tympanic membrane itself was opaque, consistent with a middle ear effusion.
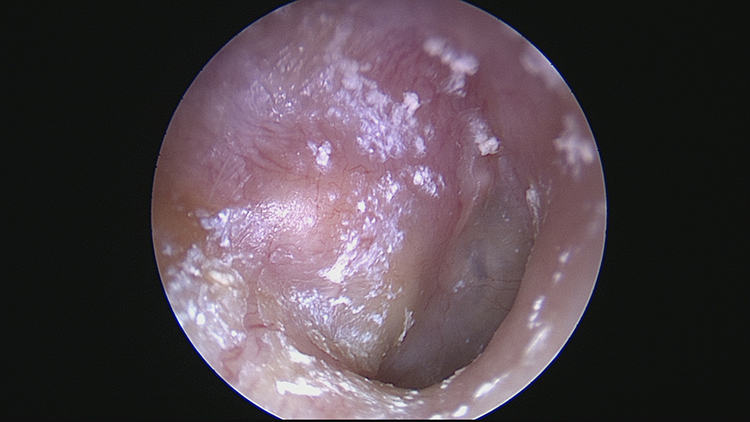
Seven days following the first postoperative visit. Her right tympanomeatal flap was minimally bulging and no longer pulsatile.
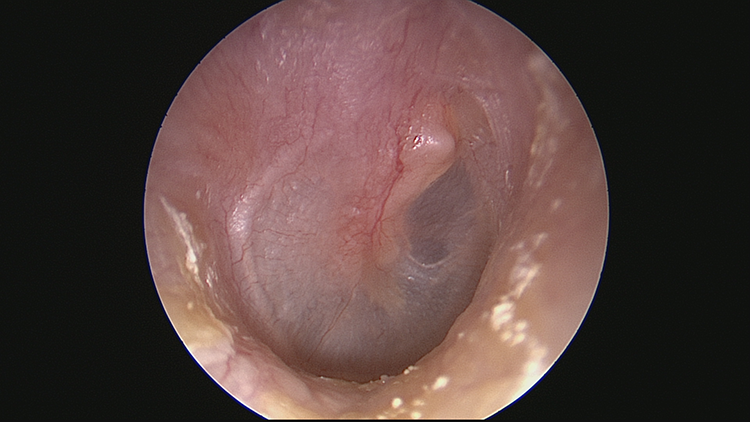
Right ear 2 months following surgery. The right tympanomeatal flap and the tympanic membrane were flat, with recovery of landmarks.
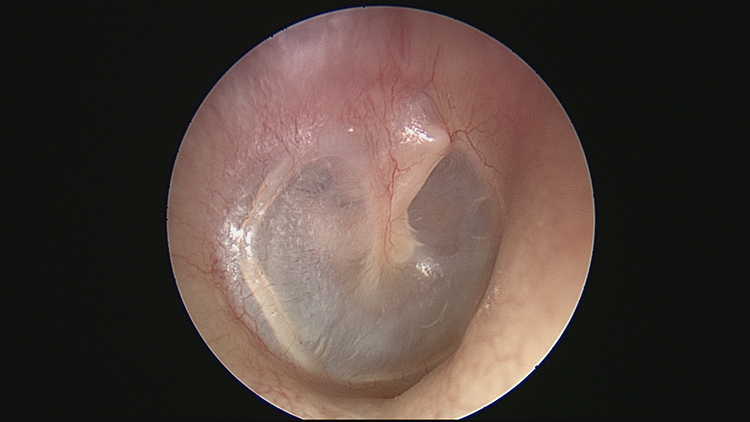
Right ear 8 months following surgery. Her right tympanic membrane had returned to normal appearance except for some displacement of the fibrous annulus.
This patient had a pseudomeningocele-like presentation after a CSF oozer following her stapedotomy. A pseudomeningocele is defined as a cystic collection of CSF fluid in an extradural space with direct communication to the CSF space. 1 A pseudomeningocele does not have a surrounding membrane but instead is contained by the surrounding soft tissue space. 2 Pseudomeningoceles can develop after trauma, iatrogenic injury, or a spontaneous opening of the dura resulting in a CSF leak into the surrounding soft tissues. 2
Otologic pseudomeningoceles are very rare, with only a couple of case reports found on review of the literature. One case presented with a post-traumatic cystic mass following head trauma: In this case, a tegmen defect that was repaired with a temporalis fascia–cartilage graft. 2 Another case presented with a cystic mass in the external auditory canal from a tegmen defect from a prior mastoidectomy: This patient had intermittent clear otorrhea and multiple episodes of meningitis. 3 In our case, a pseudomeningocele-like presentation arose from a post-stapedectomy oval window fistula and presented with a bulging and pulsating tympanomeatal flap with CSF otorrhea.
The diagnosis of an otologic pseudomeningocele is dependent on history, clinical examination, and imaging. The history may include a prior history of otologic surgery or head trauma with associated hearing loss and clear otorrhea. The exam may reveal a cystic mass within the external auditory canal or the tympanic membrane with a possible middle ear effusion. An MRI can also be essential in differentiating a pseudomeningocele from a meningoencephalocele which is a herniation of meningeal and/or encephalic issue. 4 Meningoencephaloceles can present as a non-enhancing mass that is isointense to brain tissue on MRI. 4 Computerized tomography imaging can reveal bony defects in the tegmen.3,4 In our patient, no further imaging was obtained prior to planning for middle ear exploration due to the known location and cause of the CSF leak.
The primary pathology which led to the pseudomeningocele-like presentation was a CSF oozer following the stapedotomy. Cerebrospinal fluid oozer/gusher during stapedectomy is a rare complication in which there is a sudden fluid outflow that occurs after stapedotomy. 5 A CSF gusher is a high flow of CSF that fills the middle ear suddenly, while an oozer is a slower and less profuse flow. 5 The syndrome is thought to be X-linked and can have characteristic CT findings of enlarged IAC, widening of the labyrinthine facial nerve canal, absent bony modiolus, or abnormal vestibular aqueduct. 5 However, the CT exam may be normal, particularly in females who are believed to have a milder form of X-linked stapes gusher syndrome. 6 One study found no CT abnormalities in 8 and bulbous IACs in 3 female carriers. 6 Similarly, in males a normal CT scan can be present, as 1 study showed 5 patients with perilymphatic gusher during stapedectomy with a normal CT scan and 1 patient with wide cochlear aqueduct. 5 In our case, the preoperative CT was normal, reinforcing the fact that a normal CT examination does not by itself rule out the possibility of a CSF oozer/gusher during stapedectomy. The recommended management for CSF oozer/gusher is packing with fascia/fat, potential placement of the prosthesis if the flow is slow, head of bed elevation, and consultation to neurosurgery for potential lumbar drain placement. 5
Management of pseudomeningoceles depends on the location and size of the dural defect. If present in the tegmen, a middle cranial fossa (MCF) approach or transmastoid approach may be used to obtain access. 7 An MCF approach may allow for broader exposure for larger defects but requires temporal lobe retraction with more possible complications. 7 A transmastoid approach can be used due to its lower risk of complications, but it may limit exposure for larger defects. 7 There is little evidence to show whether MCF or transmastoid is superior. Once the defect has been identified, the extradural portion of the cystic mass can be removed and the defect can be repaired with bone, fascia, cartilage, or a combination of the above.2,4 There has also been use of bone cement for repair of tegmen defects using a transmastoid approach. 7 In our patient, we immediately identified the site of the leak intraoperatively and repaired it concurrently with a perichondrial graft. Although the patient did manifest with a pseudomeningocele-like presentation following repair, it spontaneously resolved without further intervention.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.