
Abstract
Eosinophilic angiocentric fibrosis (EAF) is a rare and slowly progressive disease, which usually involves the sino-nasal structures and upper respiratory tract. It is a fibroinflammatory lesion with an unclear etiology. Recent literature suggests a relation to rheumatic or immunological disorders. Therefore, immunophenotypic workup is critical when suspected. We report a case of a 32-year-old man complaining of nasal obstruction lasting more than 2 years. Nasal endoscopy and computed tomography showed a deviated septum with bilateral soft tissue swelling. During the septoturbinoplasty, a submucosal mass with severe adhesion was observed beneath the septal flap. The mass was completely removed. Dense stromal fibrosis with eosinophil-rich inflammatory cell infiltration was found on histologic examination and the patient was diagnosed with EAF. In addition, we reviewed the pathologic diagnostic criteria, differential diagnosis, and management of EAF.
Introduction
Eosinophilic angiocentric fibrosis (EAF) is a rare, indolent disease that slowly invades the sinonasal region and upper respiratory tract. It was first described as “intranasal granuloma faciale” 1 and the nomenclature of EAF was first used as the histological description. 2 The histological characteristics of EAF are dense fibrotic stroma with perivascular onion skin-like fibrosis and dense infiltration with eosinophils, lymphocytes, and plasma cells. 3 Eosinophilic angiocentric fibrosis is also known for its relation to rheumatic or immunologically related systemic diseases. Recent reports suggest that EAF belongs to the category of immunoglobulin G4 (IgG4)-related diseases. 4,5 However, few of the existing EAF cases revealed IgG and IgG4 plasma cells in histology. Therefore, categorization of EAF as IgG4-related disease is still controversial. Here, we report a case of nasal septum EAF and review literature regarding the clinical presentation, procedure of diagnosis, histopathological characteristics, treatment, and further work up for autoimmune diseases. Informed written consent was obtained from the patient for publication of this case report and accompanying images. This case was reviewed and approved by the ethics committee of our hospital.
Case Report
A 32-year-old Asian male patient presented to our department with severe nasal obstruction and occasional rhinorrhea for over 2 years. Both nasal obstruction and rhinorrhea improved slightly when he used intranasal steroid sprays or anti-histamine medications, but the condition had reached a stage where it required a more intense treatment. On endoscopic examination, the nasal septum was deviated severely to the right, coming into contact with the right inferior turbinate (Figure 1). Both sides of the nasal septum showed soft tissue swelling. In a serum specific IgE test (ImmunoCAP), the patient was found to be allergic to animal epithelium, grass pollen, and house dust. A nonenhanced computed tomography scan revealed a homogeneous soft tissue swelling in the nasal septum and isoattenuating to nasal mucosa (Figure 2). Other paranasal sinuses were free and patent. Chest radiographs revealed no nodules or any other abnormalities.
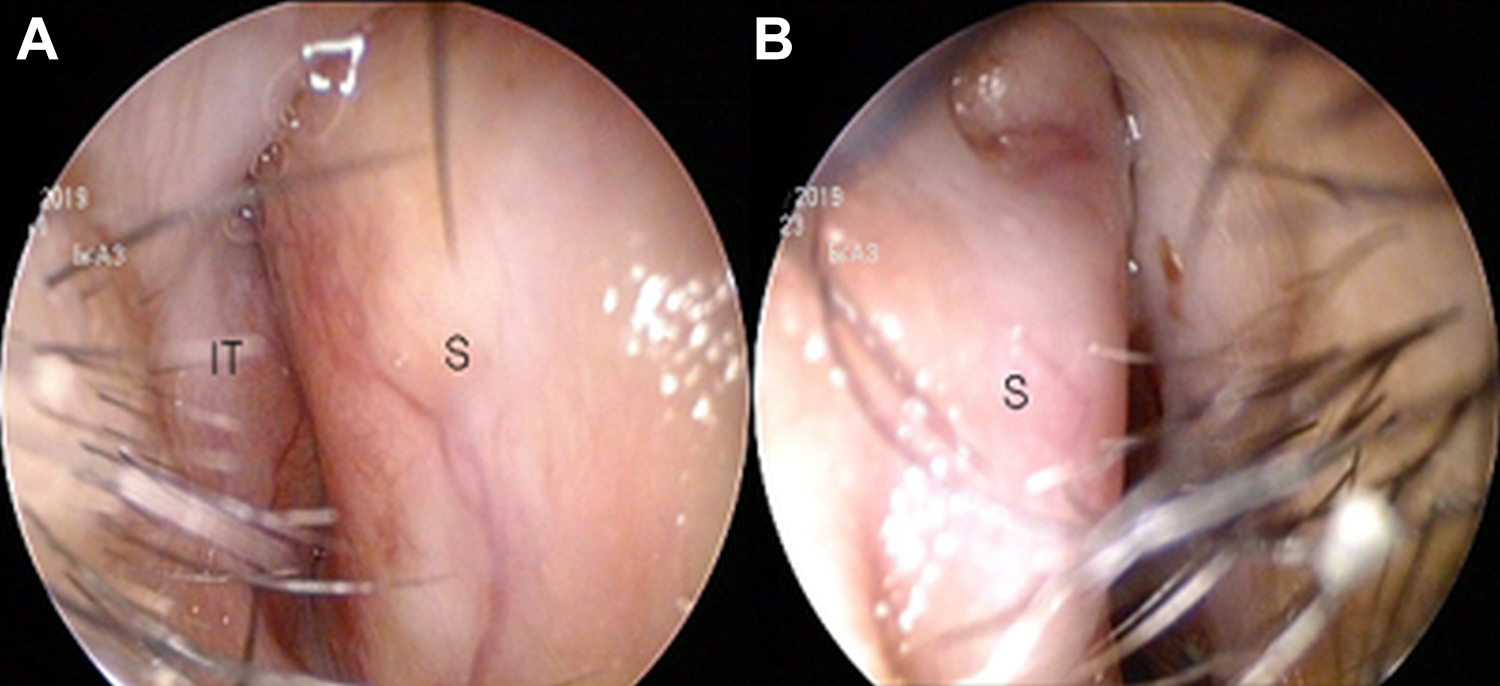
Preoperative endoscopic findings of the nasal cavity. The right nasal cavity was occluded by septal deviation. Both sides, right (A) and left (B), of the nasal septum showed swelling. (S, nasal septum; IT, inferior turbinate).
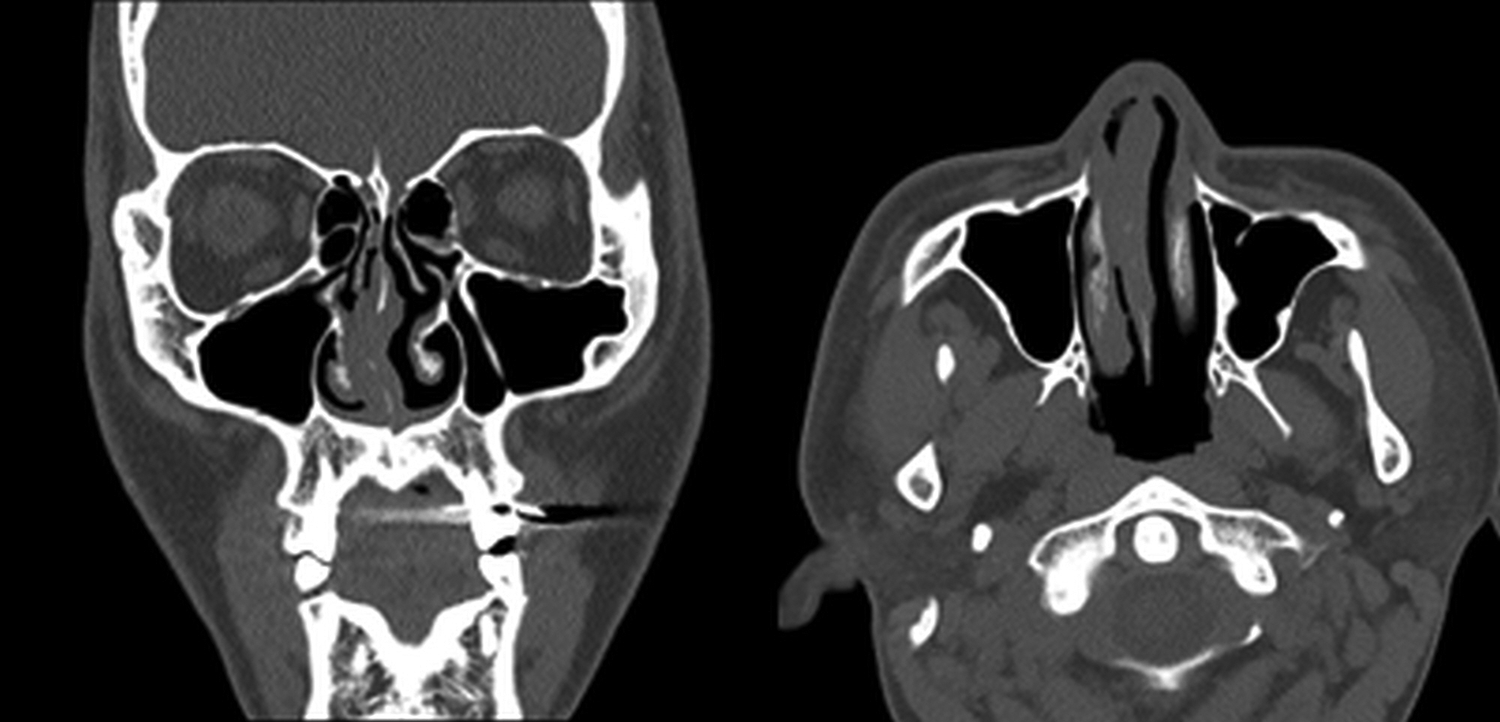
Preoperative coronal and axial computed tomography of the nasal cavity. Severe deviation to the right and swelling of the nasal septum.
The patient underwent septoplasty with bilateral turbinoplasty under general anesthesia. During the operation, a diffuse submucosal firm mass with severe adhesion to the surrounding mucosal tissue was exposed behind the normal caudal septum (Figure 3). The mass like lesion penetrated through the septal bone area and was well distinguished from the normal caudal septal cartilage (Figure 3). Finally, almost all of the submucosal soft tissue was removed and septoplasty was completed. During turbinate reduction surgery, the medial anterior submucosal portion of both turbinates revealed similar characteristics to the septal mass.

Intraoperative endoscopic view. The anterior part of septal cartilage was well dissected, and a diffuse submucosal firm mass was exposed behind the caudal part of septal cartilage. The mass was well distinguished from the normal septal cartilage. (S, caudal septal cartilage; F, septal mucosal flap).
Histological examination of the resected fragments of septal tissue revealed dense concentric fibrosis, featuring the “onion-skin” like perivascular whirling pattern (Figure 4A). Scattered eosinophils were present within the fibrotic tissue (Figure 4B). These histologic findings were the classic features of EAF. Immunohistochemistry staining showed that IgG staining was mainly positive in plasma cells, but the ratio of IgG4 to IgG positive plasma cells was lower than 10% (Figure 4C, D). The patient had no previous medical or smoking history, except for pustular type psoriasis. For psoriasis, the patient had been treated mainly with cyclosporine A and ustekinumab subcutaneous injections. We speculated that the patient’s pustular type psoriasis inferred the possibility of other rheumatic or immunologically related systemic diseases. However, rheumatoid and immunologic laboratory tests (Serum IgG, IgG4, IgA, IgM, IgE, C3, C4, C-reactive protein, erythrocyte sedimentation rate [ESR], eosinophil count, anti-nuclear antibody, anti-double stranded DNA, rheumatoid factor, and plasminogen activator inhibitor-1) did not provide any evidence of autoimmune disease.
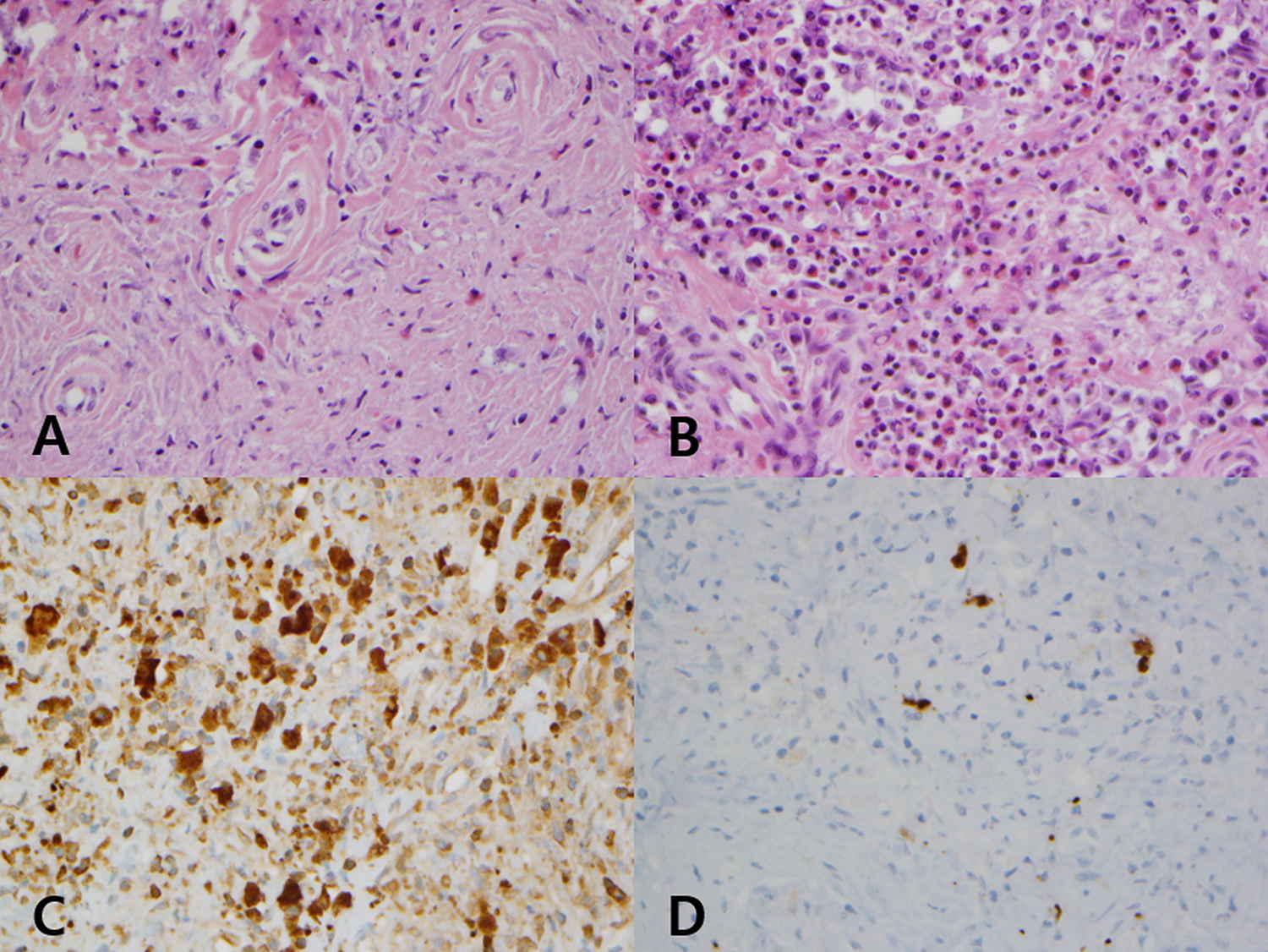
Histopathological features of the mass. A, Perivascular fibrosis with eosinophilic and lymphocytic infiltration (hematoxylin and eosin staining, ×400). B, Eosinophil-rich inflammatory cell infiltration (hematoxylin and eosin staining, ×400). C, Plasma cells showed reactivity to IgG; more than 50 IgG (+) plasma cells/HPF (IgG immunohistochemical staining, ×400). (D) IgG4 (+)/IgG (+) plasma cells < 10% (IgG4 immunohistochemical staining, ×400).
In the postoperative follow-up consultation, the patient’s nasal cavity was patent without any septum or turbinate swelling. Except for antihistamines, no other medications have been needed after the operation, and except for steroid nasal spray, no corticosteroid therapy has been considered either.
Discussion
To the best of our knowledge, this is the first case of nasal septum EAF with rheumatic or immunological analysis reported in Asia. Few cases of nasal septum EAF have been reported to date. The average age of diagnosis is 48 years (range 19-72 years) and there is no sexual predilection. Eosinophilic angiocentric fibrosis usually affects the upper airways, such as the lateral nasal wall, sinus, and septum. Symptoms are usually derived from the local destruction, or mass effect of the lesion. Therefore, patients exhibit clinical symptoms of nasal obstruction, epistaxis, and dyspnea. Nasal septum EAF cases are especially rare, even more so than sinus EAF cases. 6
As to the cause of EAF, autoimmune, allergic, and traumatic factors have been proposed. Recently some authors have proposed that EAF should be included in the spectrum of IgG4-related disease since they share both clinical and histologic characteristics. 4,5 These include dense lymphoplasmacytic infiltration, storiform-type fibrosis, the presence of tumefactive lesions, or the involvement of fibrotic organ diseases. For the diagnosis of IgG4-related diseases, immunohistochemistry staining for IgG and IgG4 is important. An increase in IgG4-related plasma cells is required and the ratio of IgG4: IgG should be over 40%. In addition, in 50% of the patients with IgG4-related disease, the serum IgG4 level was elevated. 4,5
The diagnosis of EAF mainly depends on the presence of the classic histological findings, such as an eosinophil-rich perivascular fibrosing inflammatory lesion or dense perivascular “onion-skin” fibrosis. 3 If suspected, it is important to perform IgG and IgG4 immunohistochemistry to evaluate for IgG4-related disease. In our case, although EAF could be diagnosed by histologic diagnosis and clinical history, IgG4-related disease was ruled out because the immunohistochemistry staining results did not satisfy the diagnostic conditions for IgG4-related disease. According to a recent systematic review, 7 similarities between EAF and IgG4-related disease are most noticeable during the early stages of disease and the chronic cases failed to show IgG4 positivity or IgG4 serum levels. Therefore, it appears that the IgG4 levels of this patient could have normalized because the progression of septal swelling and long history of psoriasis indicate a chronic process.
Differential diagnoses for EAF are diffuse, including many rheumatic or immunologically related systemic diseases, such as granulomatosis with polyangiitis (previously called Wegener’s granulomatosis), Churg-Strauss syndrome, Kimura’s disease, and Granuloma Faciale. 3,5,8,9 In the case of Granulomatosis with polyangiitis or Churg-Strauss syndrome, features of systemic vasculitis are present, and antineutrophil cytoplasmic antibodies should be checked for. Histologic features such as giant cells, granulomas, and necrosis present the possibility of systemic vasculitis. 3,10 -12 In the case of Kimura’s disease, clinical features include subcutaneous nodules, lymphadenopathy, and salivary gland enlargement, and eosinophils, IgE, and ESR should be examined. On histological examination, dense lymphoid aggregation with prominent germinal centers and the lack of whirling fibrosis are prominent differences from EAF. 3,10 -12 Granuloma faciale usually has clinical features of facial skin plaques and nodules, but mucosal involvement is rare. In addition, polymorphous infiltration of eosinophil, neutrophil, and lymphoid cells into the dermis is a prominent histologic feature. 9 In our case, the histologic features, clinical features, and other laboratory results showed no relation to these rheumatic or immunological disorders.
The treatment of EAF usually includes complete excision or debulking surgery. If the first is not possible, an intralesional steroid therapy or a combination of both complete excision or debulking surgery is performed. According to a recent systematic review, the prognosis was more favorable in patients with EAF when complete resection was achieved, without relation to steroid therapy. 13 The prognosis was worse in patients who had only undergone steroid therapy or incomplete lesion resection. Rituximab showed improvement in both laboratory data and tumefactive lesions, when used in EAF cases diagnosed as being in the IgG4-related disease category. 4
Although there has been no malignant transformation reported in EAF cases, long-term follow-up is needed because of the slow progressive nature and high risk of recurrence of EAF lesions. 14,15 In our case, the patient is still in the follow-up period and no complaints have been raised since surgery.
In conclusion, even though EAF is considered a rare, slowly progressive and benign disease, it should be considered by physicians when a rather common nasal septum swelling or submucosal soft tissue mass is encountered, especially during or before septoplasty. Histopathological confirmation to rule out EAF is essential and when diagnosed, it is important to perform a laboratory work up for autoimmune conditions, especially for an IgG4-related disease.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.