
Abstract
Objective:
To evaluate the quality of information presented on YouTube regarding functional endoscopic sinus surgery (FESS) for patients.
Methods:
YouTube was searched using FESS-specific keywords under the setting of “relevance.” The first 50 videos from each keyword were reviewed and analyzed by 2 independent physician reviewers. Videos not related to FESS and duplicates were excluded. Outcome measures included the modified DISCERN score (range 0-5), the Journal of the American Medical Association (JAMA) benchmark criteria (range: 0-4), a novel scoring checklist for FESS assessing usefulness (range: 0-16), and the Video Power Index (VPI). Intraclass correlation coefficient (ICC) was calculated.
Results:
Of the 200 videos identified, 95 videos were analyzed after exclusions. Videos had an average VPI of 40.8 and SD 133.2. Average scores from the 3 objective checklists among all videos were low: modified DISCERN: 1.91, SD: 1.15; JAMA benchmark: 1.91, SD: 0.76; and FESS score: 3.54, SD: 1.77. The ICC between the 2 independent reviewers was excellent for all 3 checklists. We noted significant positive Pearson correlation between all 3 checklist scores (P < .001). In between-group comparisons of mean scores, there was significantly higher DISCERN and JAMA scores for videos from university/professional organizations, as compared to videos from medical advertising/for-profit companies and independent users. There were no significant differences in FESS scores noted between the 3 groups.
Conclusion:
There were overall low scores across the modified DISCERN, JAMA benchmark criteria, and FESS scoring checklists, reflecting the poor quality of YouTube videos as a source of patient information for FESS.
Background
With the advancement of the Internet and the availability of online resources, patients are increasingly referring to online materials for information regarding disease and surgical procedures. In fact, it is estimated that upward of 70% of adults use the Internet to obtain health and health-care-related information. 1 The 2018 Health Information National Trends Survey in the United States found that over a third of patients watched health-related videos on YouTube.2,3 YouTube is the most popular online open-access video-sharing platform, with over 2 billion videos viewed daily, coming from more than 30 million unique visitors.4,5
YouTube videos as a source for patient information and education have been evaluated in the domain of bariatric surgery, vascular surgery, and gynecology.3,6-8 In the field of otolaryngology–head and neck surgery (OHNS), functional endoscopic sinus surgery (FESS) is one of the most commonly performed operations, utilized for the treatment of sinonasal disease including chronic rhinosinusitis. It is estimated that in Canada, there are 10 000 to 15 000 FESS cases performed each year, with that number estimated to be 250 000 in the United States.9,10 A study on patients’ knowledge surrounding FESS found that upward of 30% looked to YouTube as a source of information. 11
Despite this, there has been no formal evaluation of the accuracy and completeness of information presented within popular YouTube videos for FESS. Given the powerful and popular nature of YouTube as an information source, it is imperative that we understand the accuracy and reliability of these sources. Herein, we aimed to quantitatively evaluate the quality of information presented on YouTube regarding preoperative, procedural, and postoperative aspects of FESS, with the goal to better inform the patients about YouTube’s role as a potential source of information.
Methods
Ethics
The research study received exemption from research ethics board review from the St Michael’s Hospital Research Ethics Board as YouTube videos are publicly available.
Search Strategy
The video search strategy employed herein was adapted from previous studies evaluating YouTube content.3,6-8,12 An Internet browser with its cache cleared was used to conduct a one-time search on www.youtube.com on January 21, 2020, using FESS-related keywords, including “FESS,” “functional endoscopic sinus surgery,” “endoscopic sinus surgery,” and “sinus surgery.” The default search setting of “relevance” was used to replicate a typical search attempt performed by the public on YouTube. As such, the first 50 results from each keyword search were reviewed and analyzed. Videos that were non-English, not related to FESS, or duplicates were excluded from the study.
Video Assessment
Two independent physician reviewers (V.W. and D.J.L.) assessed each video for eligibility and content. Discrepancies with regard to eligibility were addressed and discussed with the senior author (J.M.L.).
Outcome Measures
The primary outcome measure was the reliability of the videos. This was determined using 3 checklists: (1) modified DISCERN criteria, (2) the Journal of the American Medical Association (JAMA) benchmark criteria score, and (3) a novel FESS scoring system. These checklists are included as part of Tables 1 to 3, respectively.
Modified DISCERN Criteria.a
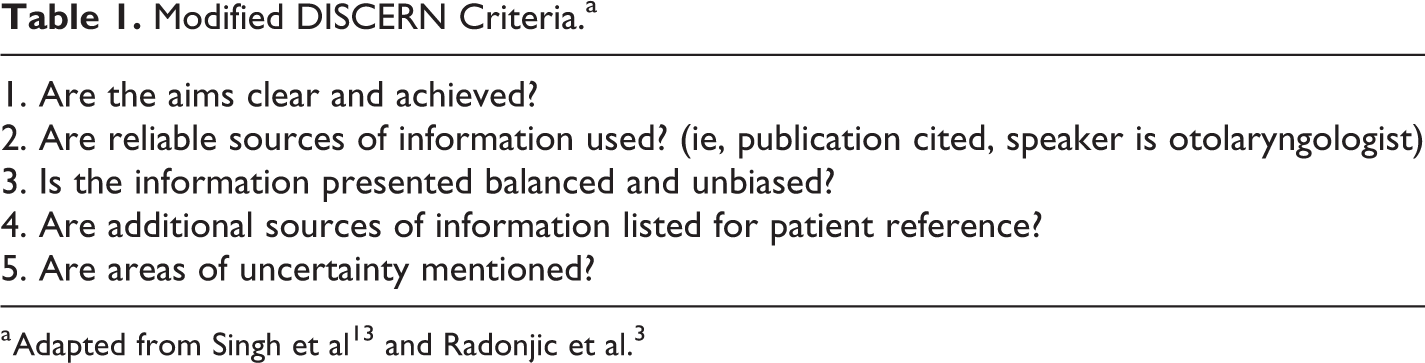
a Adapted from Singh et al13 and Radonjic et al.3
Modified Journal of the American Medical Association (JAMA) Benchmark Criteria.a

a Adapted from Radonjic et al. 3
Checklist for the Functional Endoscopic Sinus Surgery (FESS) Score.
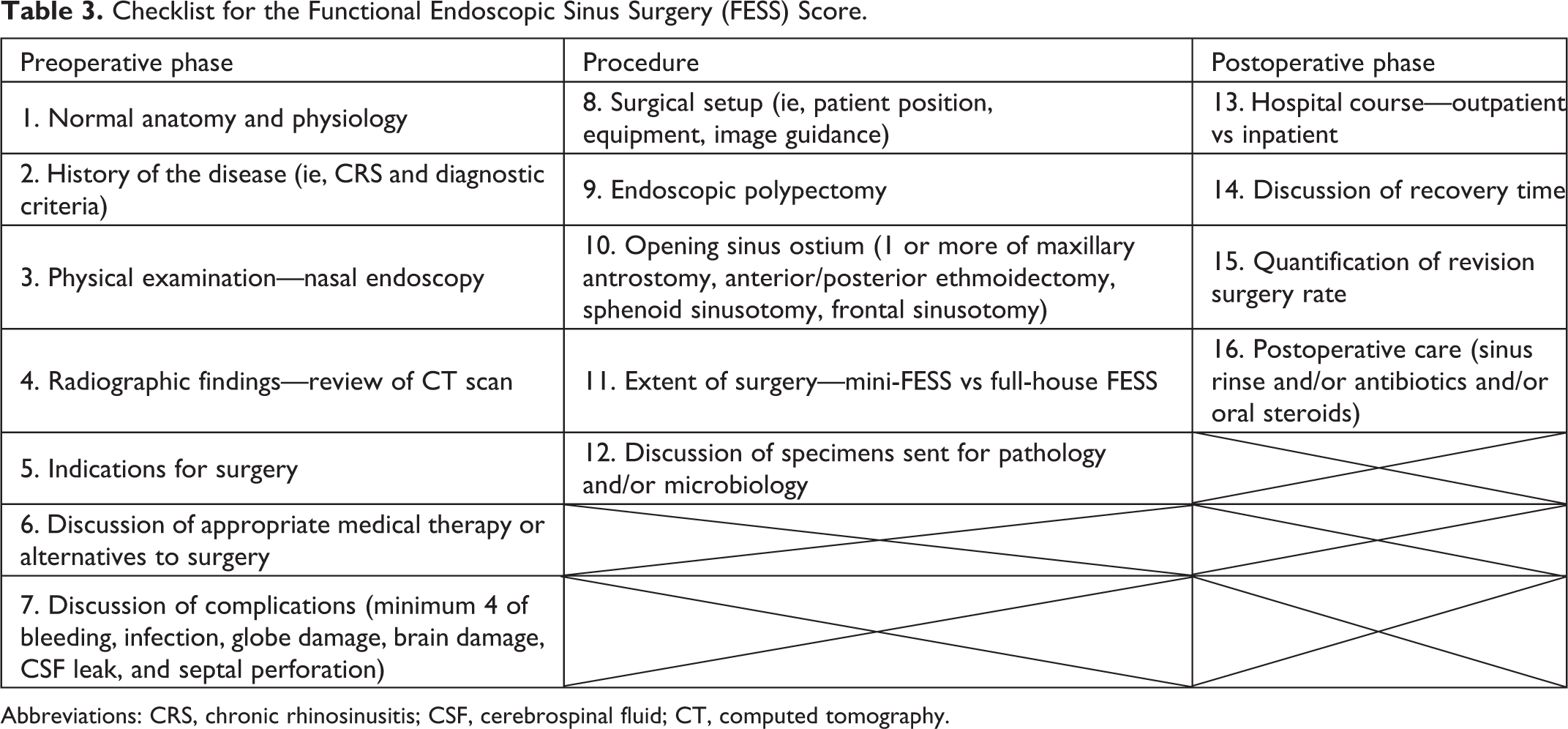
Abbreviations: CRS, chronic rhinosinusitis; CSF, cerebrospinal fluid; CT, computed tomography.
The modified DISCERN score was used to evaluate clarity of videos, reliability, bias, reference supplementation, and uncertainty of content. 13 The total score was 5 points, 1 assigned for each criteria, with higher points indicating more reliability of the videos. This is presented in Table 1. The DISCERN criterion is a brief questionnaire that has been used to assess the reliability and quality of written information. The JAMA benchmark criteria score evaluated for authorship, attribution, disclosure, and currency, with a maximum of 4 points, as given in Table 2. 14 Within the literature, both the modified DISCERN and JAMA benchmark criteria have been used in the evaluation of YouTube videos.3,15,16
As there was no available checklist in evaluating the quality of online information on FESS, a novel FESS scoring checklist was developed specifically for this study. We constructed this checklist for what a reasonable physician would need to counsel patients about the procedure. We utilized information and adapted parts of the novel FESS scoring system from the previous studies to assess YouTube videos on surgical procedures, along with a review of the current literature.3,12,17,18 Face and content validity was confirmed by 2 expert rhinologists (A.V. and J.M.L.). The novel FESS scoring checklist was marked, with a maximum of 16 points. The FESS scoring system was used to reflect the usefulness of the videos, with ratings of exceptional (13-16), useful (9-12), moderately useful (5-8), and poor (0-4). This is found in Table 3.
Secondary outcome measures included YouTube video metrics on each video, including website link, video title, duration, upload date, number of views, likes, dislikes, number of comments, and references to sources. Based on these metrics, the Video Power Index (VPI), which assesses video popularity, was also calculated: VPI = ([view ratio × like ratio]/100), where view ratio = views per day, and like ratio = (likes × 100)/(likes + dislikes).
Videos were also classified into 4 categories based on their source: university/professional organization, medical advertising/for-profit companies, independent user, and other (ie, news/media, governmental organization).
Statistical Analysis
All statistical analyses were performed using SPSS version 20, with statistical significance set at P < .05. Evaluation of inter-rater agreement was done using intraclass correlation coefficient (ICC). Descriptive statistics (mean, SD, median, frequency, percentage) was used for displaying the data. Categorical variables were reported as frequencies and relative frequencies. Continuous variables were reported as means and SD. Pearson correlation was calculated between checklists and VPI and expressed with 95% CI. Videos were categorized based on the sources of the videos and were also stratified based on usefulness via the FESS scoring checklist. Comparison of means was done using 1-way analysis of variance with Bonferroni correction.
Results
Of the 200 videos initially identified, 88 were duplicates and 17 were excluded based on the predefined exclusion criteria (Figure 1). The remaining 95 videos were available for analysis. The shortest video was 20 seconds, and the longest videos were 1 hour, 18 minutes, and 14 seconds. The videos combined for a total duration of 17 hours and 14 minutes. Video views ranged from 40 to 824 686, with a total of 6 417 472 views. Uploaded dates were from September 28, 2007, to October 14, 2019. Based on the categories, there were 23 (24.2%) videos from university/professional organizations, 13 (13.7%) from medical advertising/for-profit companies, 59 (62.1%) from independent users, and no videos from other sources (ie, news/media, governmental organization). Videos had an average VPI of 40.8, SD: 133.2.
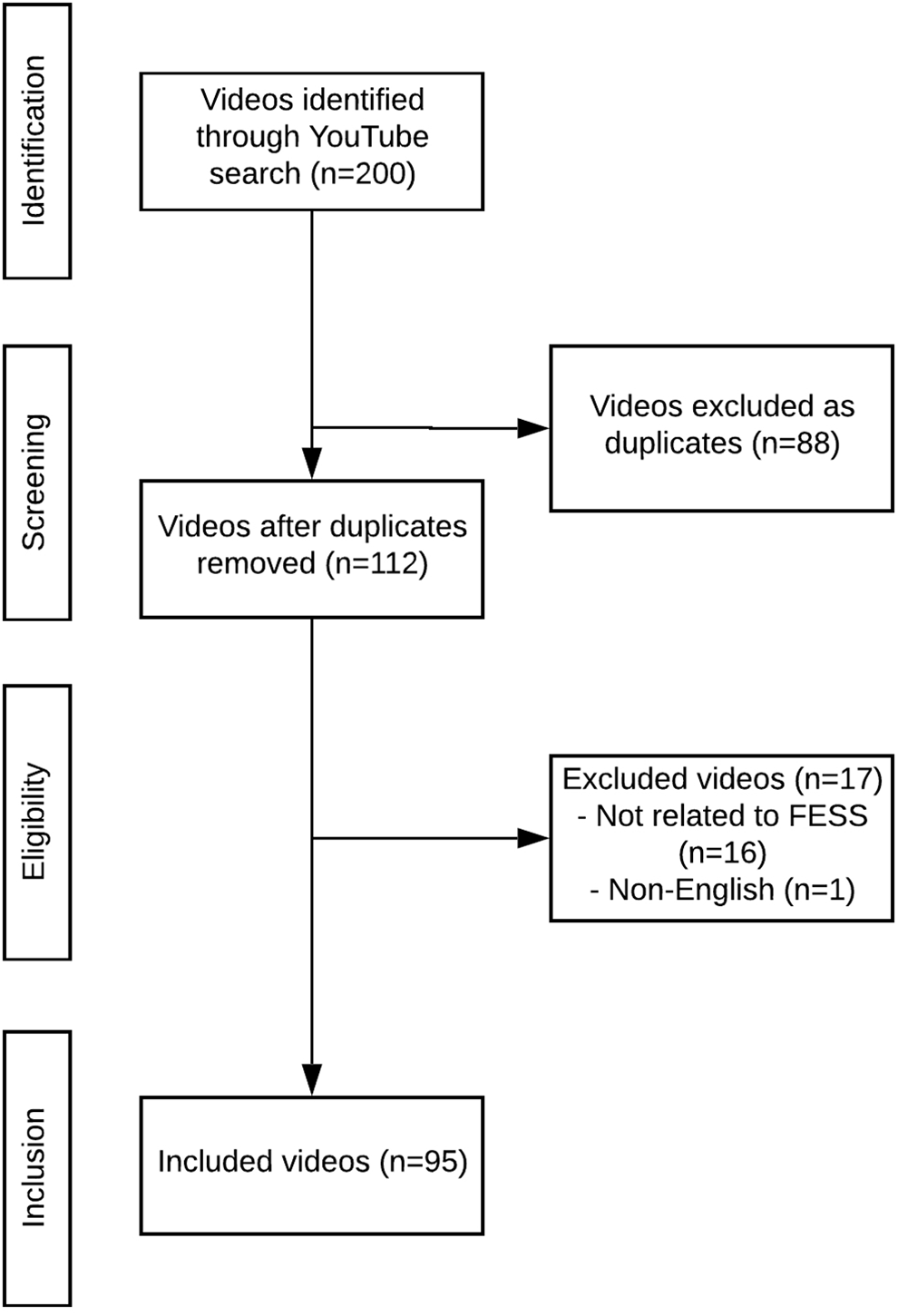
PRISMA flowchart for YouTube search.
Average scores from the 3 objective checklists among all videos were low: modified DISCERN score (1.91, SD: 1.15), JAMA benchmark score (1.91, SD: 0.76), and FESS score (3.54, SD: 1.77). Based on the predefined FESS score usefulness categories, 71 (74.7%) videos were considered poor, 21 (22.1%) moderately useful, and 3 (3.2%) useful. The ICC between the 2 independent reviewers was excellent for all 3 checklists: DISCERN (0.875, 95% CI, 0.812-0.916), JAMA benchmark criteria (0.847, 95% CI, 0.770-0.98), and FESS score (0.921, 95% CI, 0.881-0.947).
We noted statistically significant correlation between all 3 checklist scores (P < .001): DISCERN and JAMA: r = 0.745, DISCERN and FESS score: r = 0.434, and FESS and JAMA: r = 0.476. The VPI was not significantly correlated (P = 1.000), with DISCERN, JAMA, and FESS scores having Pearson correlations of r = −0.043, r = −0.045, and r = −0.088, respectively.
Comparisons of checklist scores based on the source of video categories are presented as part of Table 4. There were significant differences between groups with DISCERN and JAMA scores (P = .002 and P < .001, respectively). We did not see significant differences in the FESS score between all 3 categories (P = .675). In between-group comparisons, we only noted significantly higher DISCERN score from university/professional organizations, compared to videos from medical advertising/for-profit companies (0.91, 95% CI: 0.25-1.57, P = .003) and independent users (0.54, 95% CI: 0.07-1.01, P = .018). Higher JAMA scores were only noted for university/professional organizations videos, compared to those from medical advertising/for-profit companies (0.56, 95% CI: 0.13-0.98, P = .006) and independent users (0.55, 95% CI: 0.25-0.86, P < .001). There were no statistically significant differences seen in the mean scores from either 3 checklists between videos categorized as being from medical advertising/for-profit companies and independent users.
Between-Group Video Category Comparison of Checklist Scores and VPI.

Abbreviations: FESS, functional endoscopic sinus surgery; JAMA, Journal of the American Medical Association; VPI, Video Power Index.
When evaluating VPI scores, there were significant differences noted between groups (P = .002; Table 4). Comparing between groups, there was a significantly higher VPI for videos categorized as being from medical advertising/for-profit companies than independent users (mean difference: 100.7, 95% CI: 33.1-168.3, P = .001). No significant difference in VPI was noted for other comparisons between video sources.
Discussion
This study evaluated the quality and usefulness of information presented within popular YouTube videos on FESS for patients, with the use of independent physician evaluators and objective measurement tools. We found that of the 95 videos included for analysis, there was excellent inter-rater reliability across all 3 of the checklists. There were overall low scores across the modified DISCERN, JAMA benchmark criteria, and FESS scoring checklists, reflecting poor quality and low usefulness of YouTube as a source of patient information for FESS with currently available videos.
Within the surgical literature, studies evaluating YouTube as a source of patient information have in general found that the information presented was often varied and unreliable.3,6-8 Radonjic et al reported on the quality and usefulness of YouTube videos on patients with abdominal aortic aneurysm (AAA) and found low DISCERN (2.37, SD: 0.97), JAMA (1.74, SD: 0.84), and specific AAA (6.63, SD: 3.23) scores. 3 These findings are similar to the results from our study, and both point to the low quality of YouTube videos on surgical procedures/diseases as sources of useful information for patients. Specifically, within the field of OHNS, Haymes and Harries evaluated YouTube videos on the management of epistaxis and found that inappropriate and dangerous advice was offered within videos. The authors concluded that YouTube videos were not recommended as an information source for patients in managing epistaxis due to the varying degree of quality. 16 Another study examining YouTube videos as a source of patient information for rhinoplasty found that videos were of average quality and reliability. 15 Taken together, there is evidence suggesting overall low quality of YouTube videos as an information source for patients regarding surgical procedures and diseases.
We did not find any association between VPI, which is a reflection of the popularity of YouTube videos, and the 3 objective checklist scores. This would suggest that higher ratio of videos and activity/engagement (ie, likes, comments) on a video does not necessarily correlate with its objective quality or usefulness. This is important as patients may look toward the popularity of a video as pertaining to its accuracy, which is not the case based on findings in our study. We did note that VPI was higher from medical advertising/for-profit companies video sources, which may introduce certain commercial biases into the information presented. Additionally, we noted that videos from a university or professional organization had significantly higher scores on both DISCERN and JAMA criteria as compared to other video sources. This may reflect that the information used by universities or professional organizations were from more reputable sources and that information was presented in a more unbiased manner. However, we noted low FESS scores across video sources, which were not significantly different. This may imply that video content may not provide adequate amount of information to patients, regardless of the source. This finding highlights the need for otolaryngologists to provide credible high-quality sources of information regarding FESS to patients in the era of information explosion.
In evaluating YouTube videos, one of the themes that arose, but was not explicitly captured within this study, was on FESS educational videos geared toward medical trainees. Rapp et al identified through a cross-sectional study at a tertiary institution that YouTube was the most frequently used educational resource for surgical preparation and was used by 95% of medical students and residents. 19 Another study found that online videos were frequently used by medical trainees to prepare for surgical observerships. 20 Specific evaluation of YouTube videos as it pertained to laparoscopic surgery has revealed that videos were useful and appropriate educational tools. 21 However, other studies within the general surgery literature have shown low quality of the videos for surgical trainees, with poor or suboptimal techniques demonstrated. 8 In our study, we are unable to determine whether the videos can be used to teach FESS as this was not the aim of the study. With this uncertainty, studies in the future can aim to evaluate the accuracy and usefulness of YouTube videos on FESS in surgical training for medical trainees.
This study had potential limitations. As there was a lack of validated objective measurement tools for assessing FESS, a scoring checklist was developed for the study. This was our group’s attempt at objectively evaluating the quality of YouTube videos as it pertained to information surgeons would like to have presented to patients undergoing FESS. The checklist was developed with guidance from 2 staff rhinologists, for face and content validity, as it pertained to patient counseling. However, many of the videos on YouTube were made with regard to surgical education or promotional purposes and not purely from the perspective of patients. Moreover, although the checklist may reflect information that physicians would like to tell patients, it does not necessarily reflect the information that patients would like from YouTube videos. Noting that most patients supplement the discussions they had with their surgeons/physicians with additional sources of information such as YouTube videos, one way of identifying the subjective usefulness of the information from the patient’s perspective would be a survey of the patients who watch these videos as a future study, identifying gaps in knowledge from videos/information sources. Moreover, our cross-sectional study only evaluated videos on YouTube at one point in time. Given the enormous amount of content that is uploaded daily onto the website, there may exist more updated and useful videos in the near future. Moreover, we did not include search terms related to “balloon sinuplasty/dilation” as the procedure is currently not publicly funded within Canada. Additionally, we did not evaluate other websites aside from YouTube, as YouTube is considered the second most visited website in the world, after Google, containing 60% of all videos stored on the Internet.22,23 The majority of Google-based searches on FESS also linked to YouTube videos. Many academic institutions, including our own at the University of Toronto, have specific websites dedicated to providing patient information, often in video and interactive formats. These resources may be evaluated in the future as to determine its utility in providing patients with greater knowledge and understanding.
Conclusion
Although YouTube videos are frequently used as a source of information by patients, the overall quality and usefulness is poor as shown in the modified DISCERN, JAMA benchmark criteria, and FESS scoring checklists. Given YouTube is a frequently used resource for information by patients, otolaryngologists should aim to create and provide patients with more accurate, reliable, and useful sources of information.
Footnotes
Authors’ Note
Vincent Wu and Daniel Lee contributed to study design, data acquisition, data analysis, manuscript preparation, and revision. Allan Vescan and John Lee contributed to study design, data analysis, manuscript preparation, and revision.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.