
Abstract
Introduction:
One of the most common complications in the immediate and late postoperative period following total laryngectomy or pharyngolaryngectomy is pharyngocutaneous fistulae (PCF) formation and pharyngoesophageal stenosis (PES), causing significant mortality and morbidity. Since 1978, Montgomery salivary bypass tube (MSBT) has been used to reduce the incidence of PCF and PES. The aim of this retrospective study was to analyze the outcomes of using MSBT both as a tool to prevent PCF and PES and to treat these complications in the postoperative period.
Methods:
Between January 2013 and December 2019, we inserted 109 MSBT in 87 patients with laryngeal/hypopharyngeal cancer treated in the Unit of Otolaryngology of our University Hospital.
Results:
Sixty (86.9%) patients healed from complications with primary and secondary placement of MSBT. Seven patients presented a persistence of PCF and 2 presented a recurrence of PES. Secondary placement of MSBT allowed treating successfully 15 (83%) of 18 patients. Only 3 of them presented a PCF at the end of the follow-up period.
Conclusion:
According to our experience, the MSBT is an affordable, easy to apply and well-tolerated tool. Although it is generally used for PCF treatment, it can also be used intraoperatively for PCF and PES prevention.
Keywords
Introduction
A frequent complication in the immediate postoperative period following total laryngectomy and pharyngeal reconstruction is the formation of a pharyngocutaneous fistula (PCF), occurring between 3% and 65% of cases. 1 The etiology of PCF formation is multifactorial; according to Dedivitis et al, 2 risk factors of PCF include previous radiotherapy or chemoradiotherapy, hemoglobin <12.5 g/dL, hypopharyngeal tumor site, supraglottic tumor subsite, advanced-stage primary tumor, performance of neck dissection, positive surgical margins, infections, and chronic obstructive pulmonary disease.3-5 Another common complication is pharyngoesophageal stenosis (PES) 6 that, according to Rosales Solis et al, 7 occurs in nearly 25% of cases. The rate increases when chemoradiotherapy is administered before surgery, developing in 14% to 61% of patients. 8
In 1955, Montgomery 9 described the salivary bypass, a silicone tube placed during laryngo-esophagectomy. This device directs the saliva into the distal esophagus and can be used to allow tissue repair using pedicled skin flap tissue preventing PCF and to treat stenosis of the cervical esophagus after extensive surgery or radiotherapy. 10 A feeding tube may be inserted through the salivary bypass tube.
In this retrospective study, we retrospectively reviewed the experience of our Otolaryngology Unit using the Montgomery Salivary Bypass Tube (MSBT) to prevent or treat PCF and PES in patients affected by laryngeal/hypopharyngeal cancer.
Materials and Methods
Eighty-seven patients with laryngeal/hypopharyngeal cancer treated with MSBT (Boston Medical Products Inc, USA) between January 2013 and December 2019 at the Unit of Otolaryngology of our University Hospital were included in this study. Some of these patients underwent multiple insertions of MSBT for a total of 109 MSBT. The length of the stents was standard (191 mm), while the diameter varied from 8 to 20 mm, depending on the surgery performed and on patient’s physical characteristics.
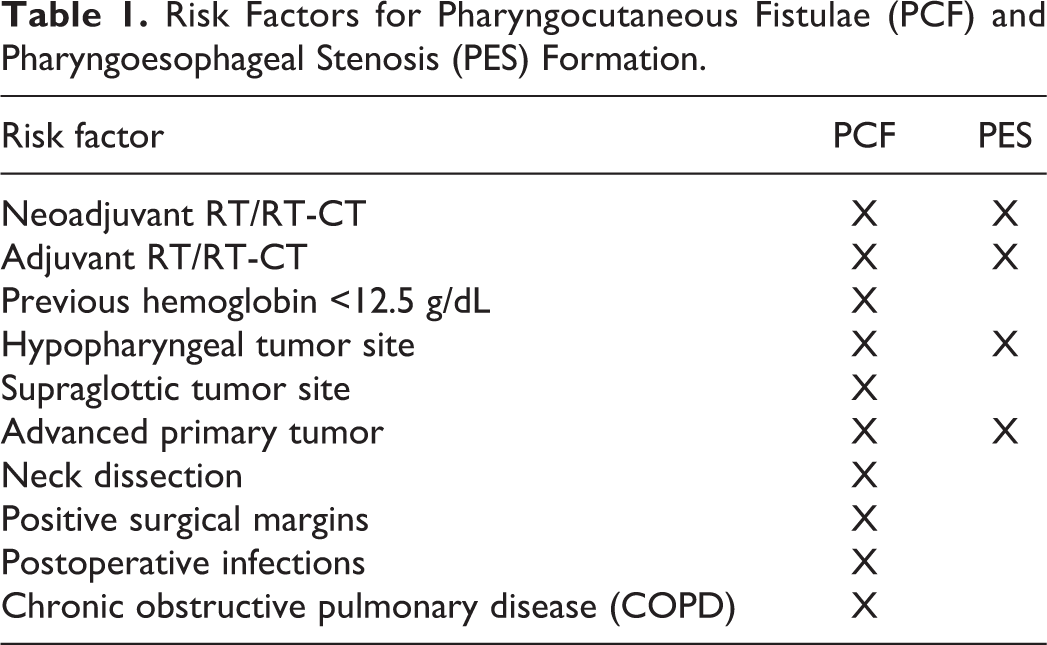
Patients were divided in 2 groups according to primary or secondary MSBT placement. Outcomes were studied in terms of oral feeding and incidence of PCF and PES complications. Risk factors for PCF and PES complications are shown in Table 1.
Risk Factors for Pharyngocutaneous Fistulae (PCF) and Pharyngoesophageal Stenosis (PES) Formation.
The criteria for primary MSBT placement included total laryngectomy extended to the base of the tongue, hypopharynx, cervical esophagus or cervical skin, neoadjuvant radiotherapy, or chemoradiotherapy. Secondary MSBT placement was performed in patients that failed or did not undergo primary MSBT placement. No anchoring systems were used.
Intraoperative placement of a nasogastric tube (NGT) in all patients ensured patient feeding for an average time of 30 days in the postoperative period (with a range of 20-42 days); swallowing rehabilitation was initiated after NGT removal with semi-liquid bolus and after about 20 (range of 15-30) days with full oral diet, as recommended by Samlan and Webster. 11
MSBT was removed using an endoscopic approach under general anesthesia 10 days after removal of NGT; oral feeding in presence of MSBT usually lasted 50 days (range 39-60 days). All patients signed a written informed consent and the study respected the principles of the declaration of Helsinki.
Results
Primary MSBT Placement
Sixty-nine MSBT were placed in patients undergoing total laryngectomy with or without partial pharyngectomy. Of these, 29 (42%) were patients undergoing total laryngectomy associated with partial pharyngectomy and bilateral neck dissection and reconstruction with pectoralis major myocutaneous flap (PMMF), 27 (39.1%) were patients undergoing total laryngectomy and bilateral neck dissection and reconstruction with PMMF; 13 (18.8%) were patients undergoing total laryngectomy and bilateral neck dissection without reconstruction with PMMF (Figure 1).
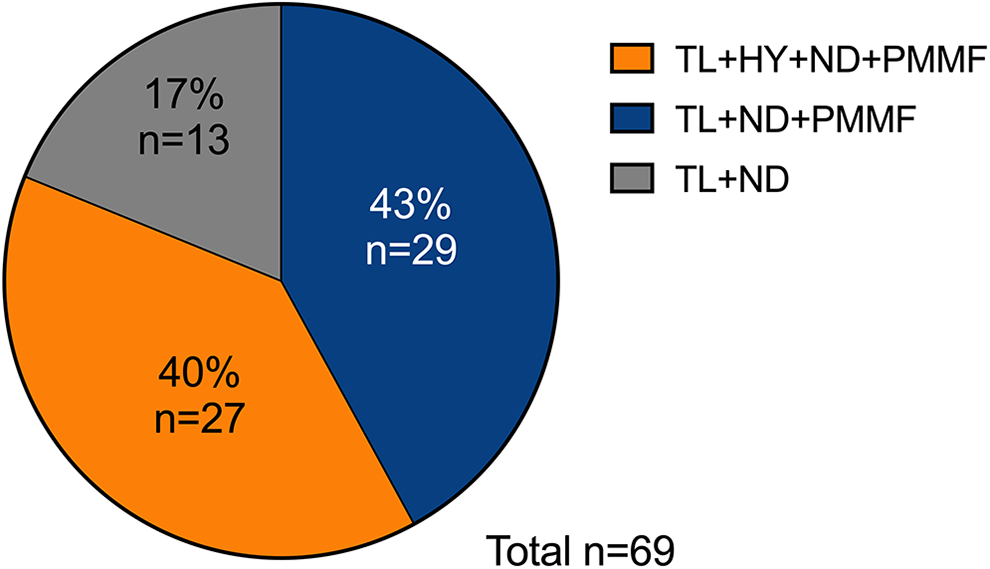
Different types of surgical treatment performed in patients with primary MSBT placement. HY indicates partial pharyngectomy; ND, neck dissection; PMMF, pectoralis major myocutaneous flap; TL, total laryngectomy.
Montgomery salivary bypass tube displacement occurred in 3 cases in which we observed dislocation of the stent in the distal esophagus or stomach. These patients were treated endoscopically with MSBT removal without further complications.
Forty-three patients underwent neoadjuvant radiotherapy or chemoradiotherapy (35 and 8, respectively). Twenty patients were treated with adjuvant radiotherapy or chemoradiotherapy. Six patients performed only surgery (Figure 2).
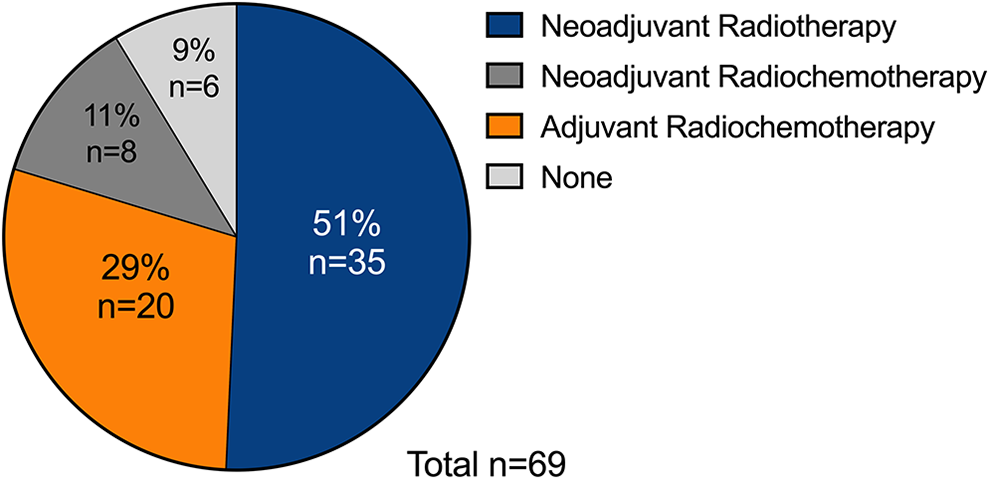
Adjuvant and neoadjuvant treatment performed in patients undergoing primary Montgomery salivary bypass tube (MSBT) placement.
An indwelling voice prosthesis (VP; Provox Vega 22.5Fr) was implanted in 16 patients with primary tracheoesophageal puncture (TEP) 12 in addition to MSBT placement. Four (25%) patients developed complications; 1 patient had PCF (6.2%), while 3 patients developed tracheoesophageal fistula (18.7%).
Among the 69 patients treated with primary MSBT placement, in 47 (68.1%) there were no complications after removing MSBT. Conversely, 22 (31.9%) patients presented sequelae after the removal of MSBT: 14 (20.3%) developed a PCF and 8 (11.6%) a PES. These patients were further treated with placement of secondary MSBT.
Secondary MSBT Placement
Forty patients underwent secondary MSBT placement, 15 for PES formation (Figure 3A) and 25 for PCF formation (Figure 3B). They included the 22 cases that failed with primary MSBT placement and 18 patients that underwent total laryngectomy without primary MSBT positioning.
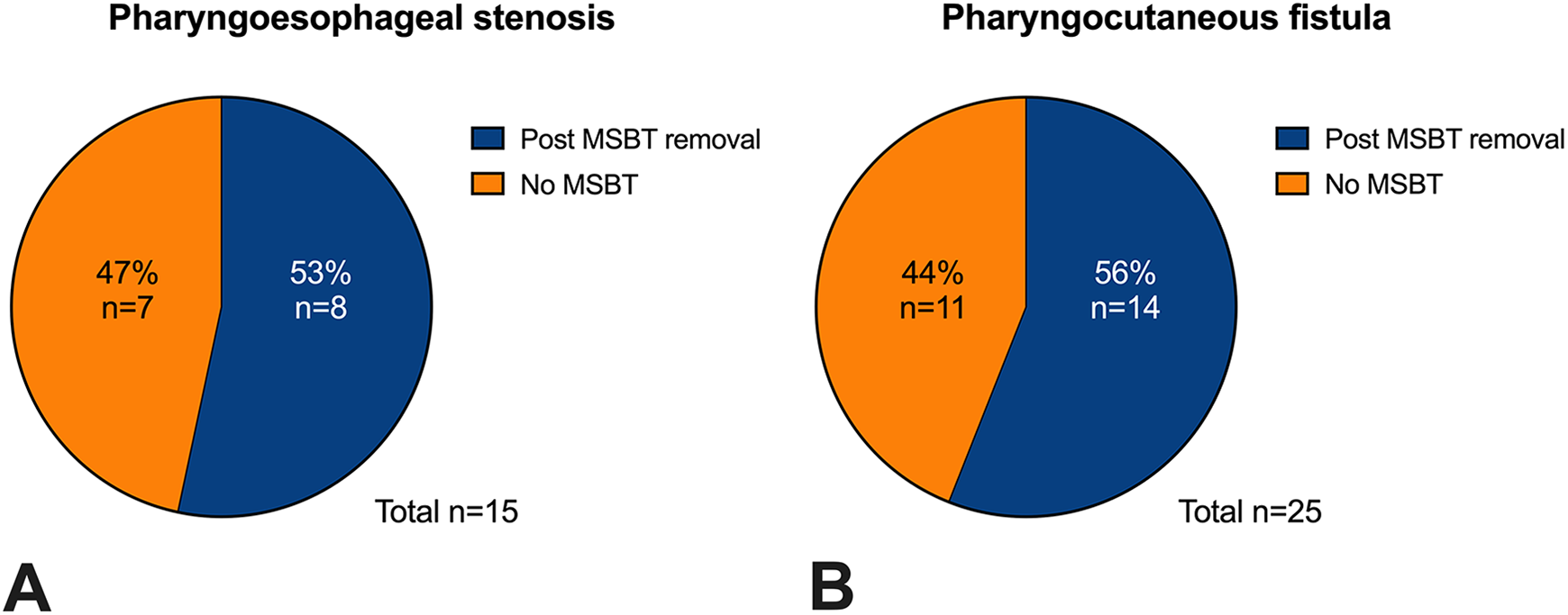
Patients undergoing secondary Montgomery salivary bypass tube (MSBT) placement; 15 for pharyngoesophageal stenosis (PES) formation (A) And 25 for pharyngocutaneous fistula (PCF) formation (B).
In patients that developed PCF requiring secondary MSBT placement, 9 needed surgical revision with primary closure or surgical repair using the PMMF due to failure of conservative treatment. Enteral feeding was guaranteed using NGT. To restore oral feeding, esophagus dilation was performed using increasing diameter sized stents placed entirely within the esophagus using a “push-through” technique. Montgomery salivary bypass tube was then inserted to maintain the calibre. During the 6-month follow-up after MSBT removal, 2 patients had a PES recurrence (13.3%).
Discussion
The use of MSBT in the management of advanced laryngeal or hypopharyngeal cancer and their complications such as PCF, PES, and tracheoesophageal fistula has been widely discussed in the literature.10,13,14
In this study, we retrospectively analyzed the outcomes of MSBT placement in patients treated in our clinic, with special attention to: (a) surgical outcomes and comparison with the literature; (b) possibility of oral feeding in patient with MSBT and PCF; (c) reduction of frequency of pharyngoesophageal restenosis after endoscopic dilation and simultaneous placement of MSBT compared to only endoscopic dilation; and (d) placement of MSBT and VP by primary TEP in 1 step.
Pharyngocutaneous Fistulae Data Analysis
Pharyngocutaneous fistulae is the most common complication after laryngeal and hypopharyngeal surgery, occurring between 3% and 65% of cases.1,15,16 The reconstruction of the surgical defect with the use of pedunculated or free flaps and the application of MSBT can significantly decrease the incidence of PCF.1,15,17-20 A recent multicenter retrospective review from the Microvascular Committee of the American Academy of Otolaryngology-Head & Neck Surgery in 486 patients with a history of laryngeal or hypopharyngeal carcinoma treated with primary chemoradiotherapy who required salvage surgery showed that primary closure of the hypopharynx was associated with a higher rate of PCF formation compared to reconstruction with vascularized tissue augmentation, concluding that vascularized tissue augmentation can reduce the fistula rate. 21
Our group placed MSBT in all cases of laryngectomy with partial or total resection of hypopharynx during surgery (primary placement). Contrarily, when performing total laryngectomy alone, MSBT was primary placed only in patients with preoperative risk factors. In our experience, the incidence of PCF after surgery and primary placement of MSBT was 20.3%, reduced to 10.1% after secondary placement.
In patients undergoing total laryngectomy without primary MSBT placement, we found a PCF in 9.2% of the patients; this percentage is in accordance with the available scientific literature. 22 Among these patients, PCF disappeared in 72.2% after secondary MSBT placement. The different complication rate may be explained by the selection of the patient and the presence of risk factors in these undergoing MSBT placement.
Our data suggest that pharyngeal resection may be an important risk factor for the development of PCF; in our opinion, we recommend primary placing of MSBT when performing pharyngeal surgery.
Oral feeding in patients with MSBT who developed PCF is still debated for the possible occurrence of complications. The presence of PCF reduces quality of life and prolongs hospitalization time; in these cases, MSBT may help nourishment initially with semiliquid bolus and gradually until a full oral diet.
Pharyngoesophageal Stenosis Data Analysis
In our case series, 15 patients with strictures of cervical esophagus were treated with secondary placement of MSBT: 8 after failure of primary MSBT placement and 7 after surgery without MSBT positioning.
A recent randomized controlled survey showed that patients that developed a PES after laryngeal/pharyngeal cancer treatment were successfully treated with endoscopic dilations in 76% of cases. 23 The study also indicated that 25% of these subjects developed a recurrence within 6 months and 50% after an average of 9.6 months. 23 Differently, we placed the MSBT immediately after the endoscopic dilation and removed it after 50 days. During a 6-month follow-up after MSBT removal, 2 patients had a PES recurrence (13.3%). These encouraging results could support the placement of MSBT immediately after endoscopic dilation.
Tracheoesophageal Puncture and VP Data Analysis
Our study also investigated the feasibility of simultaneous placement of primary MSBT and VP. Sixteen patients underwent total laryngectomy and received primary MSBT with VP placement through TEP. Four patients showed secondary complications and only 1 case developed a PCF; tracheoesophageal fistula was found in 3 (18.7%) patients due to a widening of the TEP. No correlation between PCF formation and primary TEP for VP placement was found. These data are in accordance with Divi et al 24 and with Hutcheson et al. 25 Our data show no increased morbidity or incidence of complications after laryngectomy when performing a primary TEP, also in case of reconstruction with a myocutaneous flap.
In addition, the salivary device placed with simultaneous VP had no different characteristics in length and diameter compared to those placed without VP. Also, no contrasts were found in the simultaneous positioning of both devices. In our opinion, even a possible secondary placement of VP would not decrease the risk of PCF development since PCF is not attributable to the positioning of the VP.
Conclusions
In this retrospective study, we showed the importance of the application of MSBT to reduce the incidence of fistula in high-risk patients undergoing laryngopharyngeal surgery. This approach may also represent an effective solution in hypopharyngeal and oesophageal strictures caused by treatments for advanced malignancies.
The use of MSBT should be considered a valid tool for the prevention of fistula formation and the treatment of hypopharyngeal and oesophageal strictures in high-risk patients. Montgomery salivary bypass tube is an affordable, easy to apply and well-tolerated tool, and may reduce postoperative morbidity and hospitalization time.
Footnotes
Authors’ Note
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.