
Abstract
Introduction:
In 2005, the National Prospective Tonsillectomy Audit was conducted by the Royal College of Surgeons England, reporting hot tonsillectomy techniques being associated with more postoperative pain and hemorrhage when compared with dissection. In 2006, the National Institute of Clinical Excellence declared its position on laser tonsillectomy reporting that bleeding may be less intraoperatively but is more postoperatively, that initial pain may be less but medium term is more and that healing is delayed.
Aim:
To revisit the literature surrounding laser tonsil surgery and assess the aforementioned factors for any trend changes.
Methodology:
A Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)-style systematic review conducted in July 2019 searched Embase, Medline, and Cochrane databases for randomized controlled trials comparing laser tonsil surgery with other techniques with the terms laser, tonsillectomy, and tonsillotomy for nonmalignant indications. A total of 14 articles were evaluated.
Results:
A total of 1133 patients received surgery accounting for a total of 2266 tonsil removals. A variety of laser techniques were used including CO2 (66%) potassium-titanyl-phosphate (19%) and contact diode (15%). Nonlaser techniques included dissection (62%), diathermy (20%), and coblation (18%). The summated conclusions suggest that laser techniques are superior regarding intraoperative bleeding and procedure duration. Laser techniques also provide equivocal or superior outcomes regarding postoperative hemorrhage, pain, and total healing time.
Conclusion:
Outcomes following laser surgery in recent years suggest an overall improvement. This could be due to enhanced familiarity with techniques and established centers performing laser procedures more routinely.
Introduction
The National Prospective Tonsillectomy Audit was conducted by the Royal College of Surgeons of England in 2005. 1 It is regarded as a benchmark of practice with regard to tonsillectomies in the United Kingdom. Of the 40 514 patients included in this audit, 0.9% required return to theater. The Executive summary states that the overall risk of hemorrhage related to the surgical technique—in general that hot techniques were found to have greater hemorrhage rates than cold techniques—although this was not found to be statistically significant, with the exception of coblation which was significantly associated with greater hemorrhage. The recommendations from this publication state that all hot techniques should be used with caution as a dissection tool and that all surgeons should receive training prior to adopting a new technique (such as coblation or laser).
Of the available hot techniques, laser tonsillectomy emerged as a new procedure that National Institute for Health and Care Excellence (NICE) published its position in 2006 on its application to UK practice. It reports that laser techniques are associated with the study by NICE.
2
Bleeding may be more common postoperatively but less severe intraoperatively.
Pain may be less in the first 24 hours, but long-term pain (2 weeks) may be worse.
Healing may be slower when compared with cold techniques. Aim
To review the literature for contemporary information about the associated complications of laser tonsillectomy when performed for nonmalignant indications.
Materials and Methodology
A Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)-style search was conducted using Embase, Medline, and Cochrane databases. Search terms included the terms “laser,” “tonsillectomy,” “tonsillotomy, “randomised-control trial.” Embase retuned 19 studies, Medline returned 22 studies and the Cochrane library returned 33 studies. After duplications were removed a total of 37 initial studies were identified.
Inclusion criterion is as follows: randomized controlled trials (RCTs) comparing laser tonsillectomy and tonsillotomy to other forms of tonsillectomy and tonsillotomy, in all age groups, for nonmalignant indications, after the year 2000, where outcome measures included any or all of the following parameters: validated postoperative visual analog scores (VAS) for pain, intraoperative bleeding volumes, intraoperative time for surgery, primary and secondary postoperative hemorrhage rates, and time taken to return to activities of daily living (ADLs).
Subsequent abstract review lead to 20 studies being identified as suitable when compared with inclusion criteria. Articles were excluded if text was of non-English language, resulting in a final count of 15 articles.
Results
A total of 1163 patients received bilateral tonsil surgery accounting for 2326 unilateral tonsil operations being performed—1102 by laser techniques and 1224 by nonlaser techniques. All studies commented that their groups were well matched for age, gender, and pathological indication.
Within the laser group, 665 were removed by carbon dioxide (CO2) laser (60.3%), 238 by potassium-titanyl-phosphate (KTP) laser (21.6%) and 199 by contact diode laser (18.1%), as shown in Figure 1. Within the nonlaser group, 792 were removed by dissection (64.7%), 238 by diathermy (19.4%), and 194 by coblation (15.8%) as shown in Figure 2.
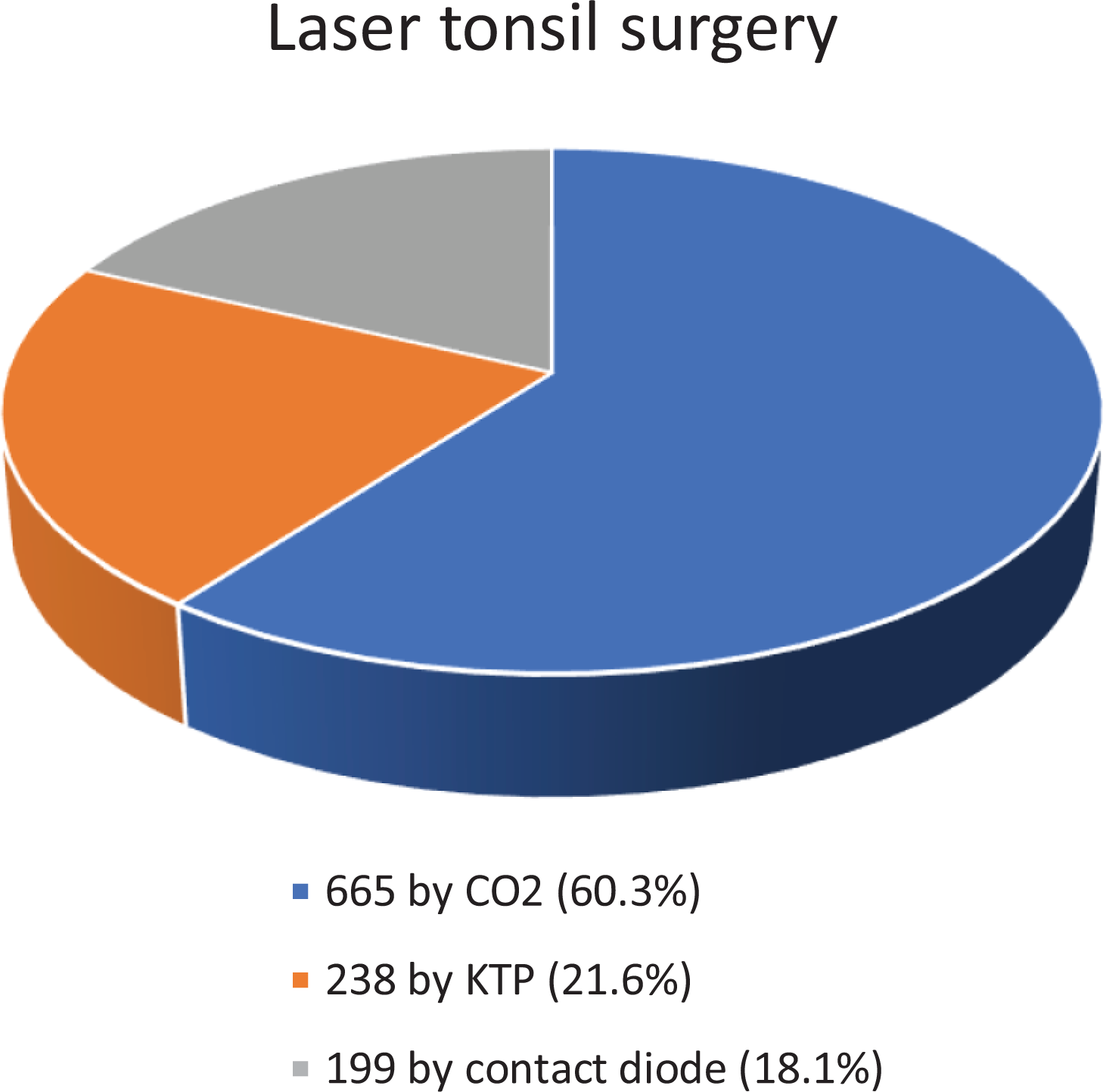
Graphical representation of the percentage each laser technique was utilized.
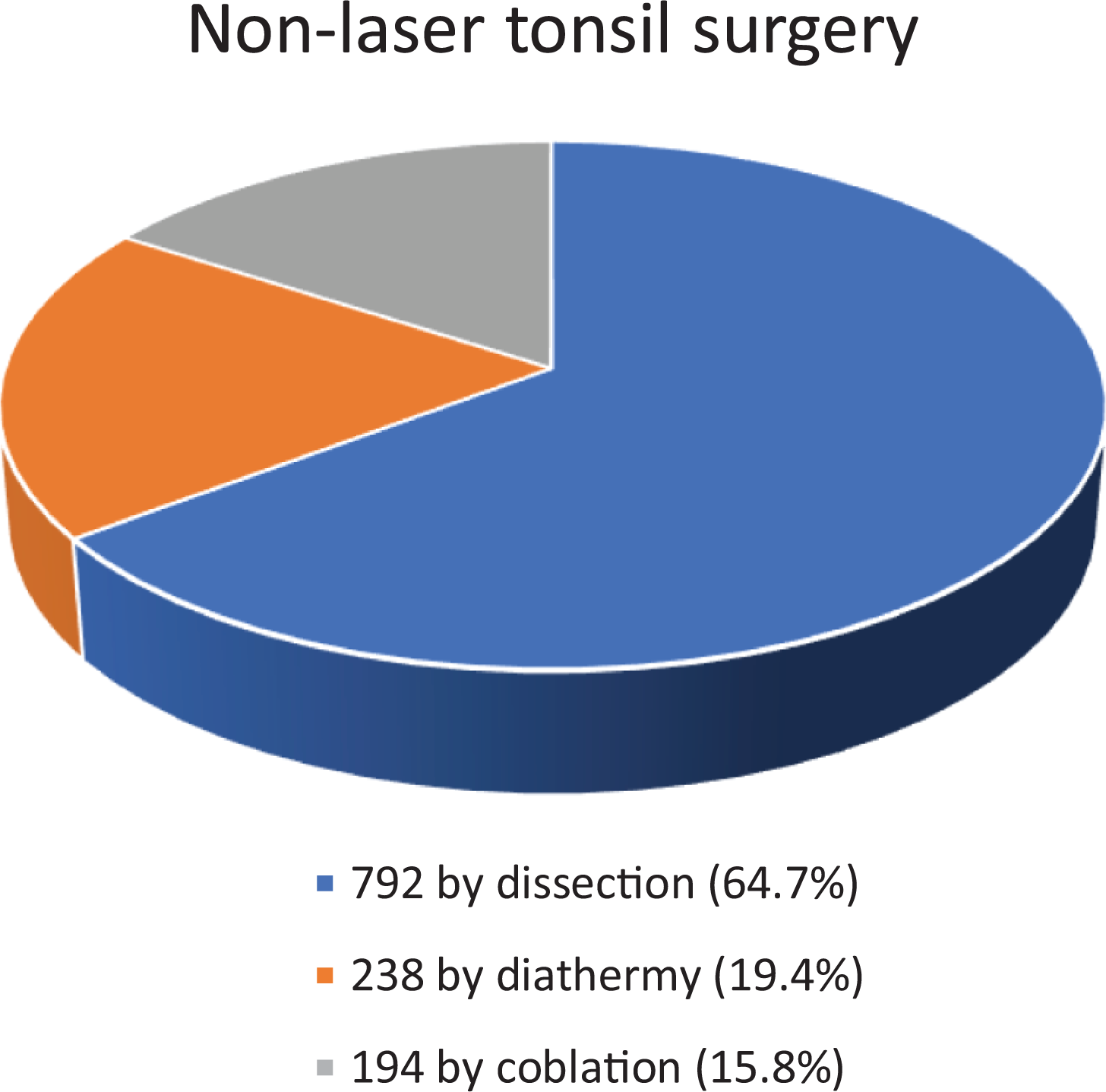
Graphical representation of the percentage that each nonlaser technique was utilized.
The main primary outcomes measured were intraoperative time, intraoperative blood loss, postoperative pain, and postoperative hemorrhage. A summary of these results is displayed in Table 1.
Summary Table Displaying the Individual Conclusions for Each Paper for Intraoperative Time, Intraoperative Bleeding, Postoperative Pain, and Postoperative Hemorrhage Rates With Graphical Representation Below of the Summated Outcomes.
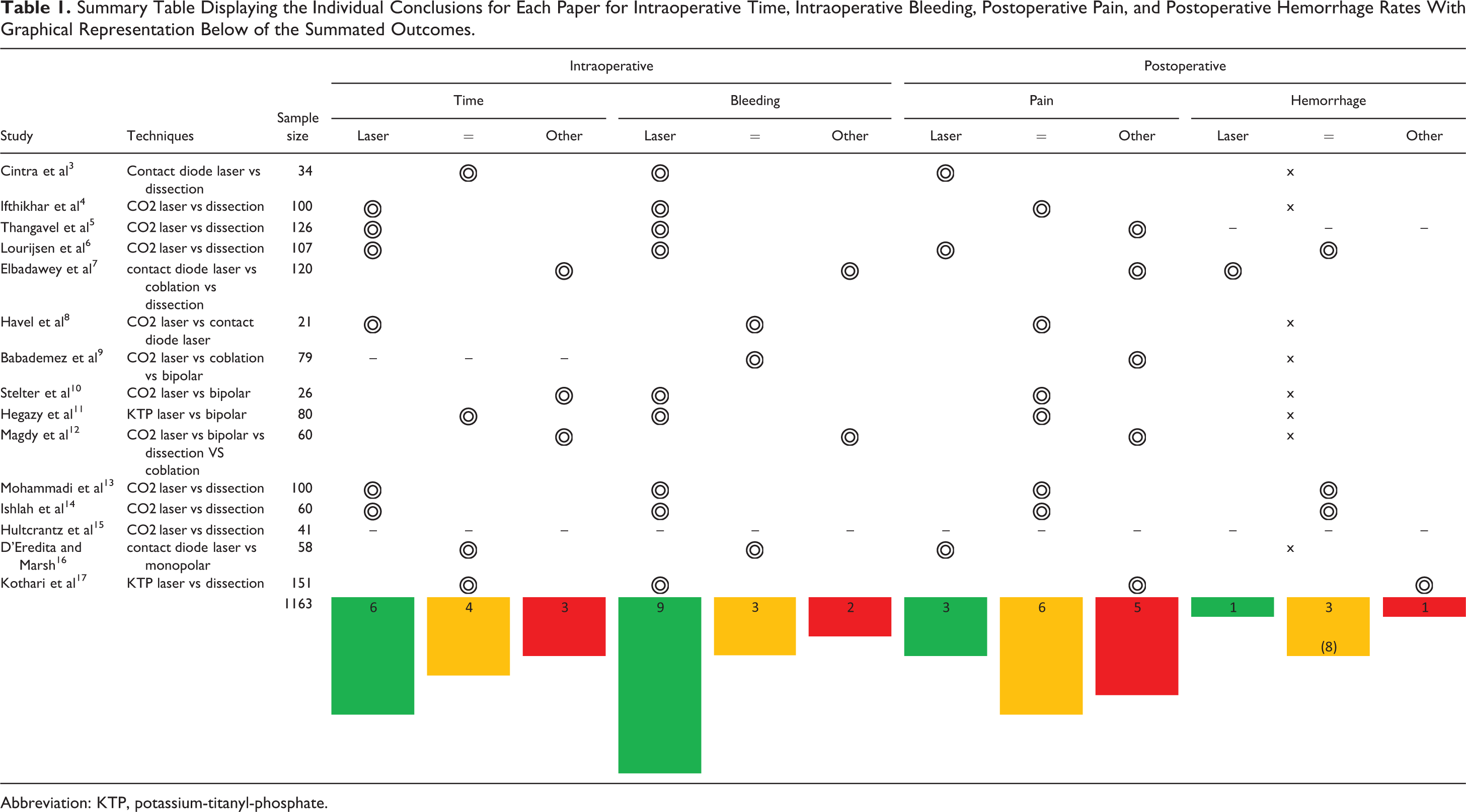
Abbreviation: KTP, potassium-titanyl-phosphate.
Intraoperative Time
Six of the 15 RCTs found laser techniques to be faster, these were all in comparison to dissection. Four of the RCTs found speed of laser surgery to be equivocal, 2 of which compared laser to dissection and 2 compared laser to diathermy. Three RCTs found laser to be slower, interestingly in comparison to coblation in 2 articles and bipolar diathermy in one article. No meta-analysis could be performed due to different start and end times being used.
Intraoperative Blood Loss
Nine of the 15 RCTs found laser techniques statistically significantly superior—7 articles in comparison to dissection and 2 articles in comparison to bipolar diathermy. Three RCTs found blood loss with laser equivocal, all of which were in comparison to other hot techniques. Two RCTs found coblation to be superior to laser, but in both articles laser still performed better than dissection. Meta-analysis could not be performed due to different techniques being used to record intraoperative blood loss.
Postoperative Pain
Three of the 15 RCTs found laser techniques superior at minimizing postoperative pain, 2 of which were compared to dissection and compared to monopolar diathermy. Six of the RCTs found postoperative pain associated with laser techniques to be equivocal, in comparison to dissection for 3 articles, bipolar diathermy in 2 articles, and compared to another laser technique in 1 article. Five of the RCTs found laser to be inferior at minimizing postoperative pain, 1 article compared to dissection, 3 with coblation, and 1 found early pain scores to be equivocal but pain at 30 days to be greater in the laser group. Meta-analysis could not be performed on this variable.
Postoperative Hemorrhage
One RCT found laser superior, this was in comparison to coblation. Three RCTs found laser to be equivocal, all of which were in comparison to dissection. All other RCTs did not report any bleeding with the exception of one which reported 11% bleeding with laser in comparison to 5.5% with dissection. Meta-analysis could not be performed on this variable due to insufficient numbers of reported bleeds.
Other Observations
No deaths or significant complications were reported in any of the RCTs. One study, by Lourijsen et al in 2016, reported that patients returned to normal activities more rapidly following laser tonsil surgery. One RCT by Hultcrantz et al in 2005 reported that long-term outcomes at one year were identical when comparing CO2 laser with dissection tonsillectomy.
Discussion
There is inconsistent methodology for collecting data on total intraoperative blood loss which prevented meta-analysis of the data. Methods included swab weights, suction chamber volumes, and combination of the 2, but there was a lack of consensus. If we assume the individual project conclusions are reliable for comparison within the study, then the overall message is that laser tonsil procedures lead to a near bloodless surgical field and in cases where there is bleeding it is significantly less when compared with dissection techniques. This is a unanimous observation with the exception of one study by D’Eredita et al in 2004 which compared contact diode laser with monopolar cautery which found equivocal intraoperative blood loss volumes. Additionally, nonsuperiority was the conclusion for Babademez et al in 2011, and studies which compared laser to coblation found coblation to be superior, as reported by Magdy et al in 2008, and Elbadawey et al in 2015.
Post-tonsillectomy hemorrhage was largely reported by the majority of studies as being not encountered. In those studies where post-tonsillectomy hemorrhage was observed, rate was identical or favorable for laser techniques. One exception is seen in the Kothari et al study from 2002 which compared day case KTP laser tonsillectomy with day case dissection tonsillectomy and found 11% reactionary hemorrhage in the laser group compared to 5.5% reactionary hemorrhage in the dissection group. These data precede the 2006 position paper from NICE.
There are limitations within the literature regarding time-taken to perform surgery, which on balance was less for laser procedures. This review could not perform meta-analysis of the data as some papers began timing immediately after insertion of the Boyle-Davis gag whereas others began timing at the first incision. Most papers seemed to stop timing after removal of the Boyle-Davis gag but the variation in the start time milestone complicated direct comparison. A general consensus of start and stop times, or a much larger study, would have to be conducted in order to reach a more reliable conclusion about the time required for laser surgery. This would have to take into consideration the time taken for equipment checks and laser safety protocols as these are clearly important factors with laser procedures.
A similar limitation exists for direct comparison of postoperative pain due to a number of VAS tools being utilized across studies. One could consider simply aligning VAS scales for data comparison where maximum and minimum pain responses aligned and the options in between were superimposed but this introduces error by assumption and is not necessarily robust enough to provide guidance on surgical practice. A general consensus to adopt one VAS tool for recording postoperative pain, or a larger study, would have to be conducted in order to reach a reliable conclusion. However, if we accept that VAS tools are reliable for comparison within a study then the summative outcome is that laser tonsil surgery is associated with an either equivocal or favorable pain experience 78% of the time. This figure has been arrived at my taking the number of cases within a project as a data value, the study conclusion as the variable (superior, equivocal, or inferior) and collating the outcomes.
Only one article, conducted by Lourijsen et al in 2016, reported duration of recovery as a primary outcome and found a faster return to normal ADLs with laser tonsillotomy compared to dissection tonsillectomy. When considered alongside the conclusions from a study by Hultcrantz et al in 2015, which compared outcomes from the same groups, the summative findings support the notion that laser tonsillotomy provides the same long-term disease control as dissection tonsillectomy but has a favorable morbidity profile.
Conclusions
Following systematic review of the RCTs comparing laser tonsillectomy and laser tonsillotomy with other established tonsillectomy and tonsillotomy techniques, the authors have established that laser techniques are equivocal or superior in 77% of trials at reducing intraoperative time, in 86% of trials at reducing intraoperative bleeding, in 64% of trials for reducing postoperative pain, and in 92% of trials for reducing postoperative bleeding.
Footnotes
Authors’ Note
J.A. and A.A. equally contributed.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.