
Abstract
Background:
Low-temperature plasma tonsillectomy (LTPT) has emerged as a promising surgical technique for treating chronic tonsillitis (CT), offering advantages such as reduced postoperative pain, faster recovery, and decreased risk of bleeding compared with traditional tonsillectomy (TT). However, the comparative effectiveness and safety of LTPT remain under debate.
Objective:
This study aimed to systematically evaluate the clinical outcomes and complication rates associated with LTPT versus TT in CT patients.
Methods:
A comprehensive literature search was conducted across major databases, including Chinese Biomedical Literature Database (CBM), China National Knowledge Infrastructure (CNKI), Wanfang, VIP, PubMed, EMBASE, and the Cochrane Library, covering studies published between January 2010 and the present. Eight case-control studies comprising 654 patients were included. Data were analyzed using the RevMan 5.3 software, and risk of bias was assessed based on the Cochrane Handbook.
Results:
Meta-analysis revealed that LTPT significantly reduced operation time (MD −12.4 minutes, 95% CI −15.2 to −9.6), intraoperative blood loss (MD −15.2 mL, 95% CI −20.1 to −10.3), and hospitalization duration (MD −0.7 days, 95% CI −1.0 to −0.4). LTPT was also associated with faster white membrane formation and lower postoperative visual analog scale scores. Inflammatory markers such as tumor necrosis factor-α (P = .002) and hypersensitivity C-reactive protein (P < .001) were significantly lower. Additionally, the complication rate in the LTPT group was markedly reduced (RR = 0.42, 95% CI 0.31 to 0.57; P < .001).
Conclusion:
LTPT demonstrates superior perioperative outcomes and safety compared with TT in CT patients. Despite these benefits, further large-scale, high-quality studies are needed to confirm its long-term efficacy and guide clinical application.
Keywords
Introduction
With continuous advancements in medical technology, tonsillectomy maintains a critical role in otorhinolaryngology, particularly for recurrent acute tonsillitis and obstructive sleep apnea (OSA) syndrome, where it remains the standard therapeutic intervention. 1 Traditional tonsillectomy (TT), which includes cold knife resection, thermal resection, or electrocoagulation resection, has been widely used and has a long clinical application history with clear therapeutic effects. 2 However, traditional surgeries are often accompanied by significant intraoperative blood loss (IBL), considerable postoperative pain, and a relatively-long recovery time, which brings a certain burden to the postoperative rehabilitation of individuals. 3
The low-temperature plasma tonsillectomy (LTPT) has provided a new technical option for tonsillectomy. The low-temperature plasma (LTP) technology decomposes and coagulates tonsillar tissue at a relatively-low temperature, demonstrating significant advantages in reducing postoperative pain and intraoperative bleeding. Moreover, due to its minimally-invasive nature and less tissue damage, it shortens the postoperative recovery time of patients.4,5 Low-temperature plasma resection (LTPR) is widely regarded as a safer and more effective surgical approach, particularly for reducing postoperative discomfort and minimizing the risk of bleeding. Despite its increasing adoption in clinical practice, debates persist regarding its advantages and limitations. While some studies have reported that LTPR significantly reduces postoperative pain and facilitates faster recovery, 6 others have found no notable differences between this method and traditional techniques in terms of long-term efficacy or severe complications, such as postoperative bleeding and wound infection. 7 Consequently, the clinical value of LTPR in the treatment of chronic tonsillitis (CT) cannot be definitively established based on isolated studies or improvements in single evaluation metrics. Comprehensive, high-quality research is necessary to provide a more conclusive assessment of its efficacy and safety. High-quality research evidence remains essential to establish the feasibility and safety of LTPR in treating CT. In light of this, further rigorous investigations are crucial, and more authoritative scientific studies are needed to validate its clinical utility. To address this need, our hospital initiated this study, employing meta-analysis as a systematic, quantitative, and comprehensive approach to synthesize data from multiple independent studies of the same type. The objective is to evaluate the efficiency and security of LTPR for CT, thereby providing robust and objective evidence to support its clinical application and guide future research endeavors.
Research Content and Methods
The Sources and Retrieval Methods of Literature Materials
The following databases were systematically searched from January 2010 to present: Chinese Biomedical Literature Database (CBM), Wanfang Database, VIP Database, China National Knowledge Infrastructure (CNKI), ScienceDirect, Cochrane Library, EMBASE, and PubMed. These databases were selected to comprehensively cover both international and Chinese literature relevant to otolaryngology procedures. No additional databases were used beyond these 8 sources. In addition to manual searches and literature-tracking techniques, the search included relevant Chinese and international journals, dissertations, conference papers, and news articles. The inclusion criteria targeted case-control trials involving patients with CT treated with either LTPR or conventional tonsil surgery.
The search approach combined subject-specific keywords with free-text keywords, including but not limited to: “traditional stripping technique,” “low-temperature plasma resection,” “tonsillitis,” “clinical effect,” “complications,” “clinical efficacy,” and “traditional stripping.” The search period was restricted to publications from January 2010 to the present. This approach aimed to ensure a thorough collection of relevant studies for systematic review and meta-analysis. This systematic review and meta-analysis utilized only de-identified data from previously-published studies. As no new human or animal subjects were involved, institutional ethics approval and patient consent were not required. All original studies included in our analysis had obtained appropriate ethical approvals, as confirmed in their respective publications.
Inclusion Criteria for Literature
(1) Study type: Case-control or randomized controlled trials (RCTs) that compared LTPT with TT as intervention measures for patients with CT, 8 including both domestic and international studies. (2) Study subjects: Patients aged ≥5 years with CT, recurrent tonsillitis (≥3 episodes/year), or OSA 9 Studies focusing on malignancy, acute infections, or peritonsillar abscess were excluded. (3) Intervention measures: The study group underwent LTPT, while the control group obtained TT. (4) Outcome indicators: (a) operation time (OT), (b) IBL, (c) hospital stay (HS), (d) time of white membrane formation (WMF), (e) levels of inflammatory factors, (f) postoperative pain visual analog scale (VAS) score, (g) incidence of complications, (h) no language restrictions were applied, and non-Chinese studies were translated where necessary.
Exclusion Criteria for Literature
(1) Lack of a case-control study, (2) incomplete data reporting, which prevents data from being used, (3) redundant research material, since the most recent study is chosen, (4) studies that failed to quantitatively report primary outcomes (eg, operation time, blood loss, complication rates) or used non-validated assessment tools, (5) literature review, (6) clinical case. Studies of tonsillectomy for malignancy, HIV-related indications, or isolated peritonsillar abscess without recurrent tonsillitis were excluded.
Only studies reporting at least 2 of our predefined primary outcomes (operation time, IBL, hospital stay, or complication rates) using standardized measures were included.
Quality Assessment and Data Extraction
(1) Risk-of-bias assessment for included studies: Quality assessment followed the Cochrane Handbook for Systematic Reviews version 6.0 (Higgins et al 10 ). (2) Literature screening and data extraction: The literature was separately examined, data were extracted, and the quality was assessed by 2 researchers. They cross-checked each other’s results to ensure accuracy. If there was dispute, a third researcher was approached for arbitration after conversations were made to try to establish a consensus. The data from the chosen studies were arranged and extracted using Excel and Express literature management software. For studies with incomplete data, the corresponding authors were contacted to obtain Supplemental Material. The data extraction contents included the following: (1) Basic information: authors, publication year, and number of cases in each group; (2) Intervention measures: treatment protocols and duration of treatment courses; (3) Outcome indicators: OT, IBL, HS, time of WMF, levels of inflammatory factors, postoperative VAS scores, and incidence of complications, etc.
Statistical Processing
The Cochrane Collaboration’s RevMan 5.3 software (The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, Denmark) was accustomed to carry out the meta-analysis. Relative risk (RR) was employed as the effect indicator for count data, such as postoperative complication rates, and weighted mean difference (WMD) was employed for continuous data, such as OT, IBL, HS, WMF time, postoperative VAS scores, and inflammatory response factors. Ninety-five percent confidence intervals (95%) were used to compute all effect estimates. To evaluate study heterogeneity (HE), the Chi2 test (also known as the χ2 test) was used. The studies were deemed homogenous and a fixed-effects model was applied if I2 < 50% and P > .05. In contrast, a random-effects model (REM) was employed if I2 < 50% and P > .05, signifying considerable HE. Descriptive analysis was employed in place of meta-analysis where HE was substantial (P < .05), and its cause could not be determined. Asymmetry was assessed using Egger’s test, while publication bias was investigated using funnel plots. When Egger’s test showed significant asymmetry (P < 0.1), the effect size was adjusted for potential publication bias and the funnel plot was fixed using the Trim and Fill method. This thorough strategy addressed concerns of HE and publication bias while guaranteeing the validity and reliability of the meta-analysis findings.
Results and Analysis
Literature Search Results and Basic Information of Included Literature
Literature research was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. A total of 1654 items were found by searching computer databases, while the majority of included studies were from Chinese databases, no studies meeting eligibility criteria were excluded based on language or region. After removing duplicates, 1126 articles remained. Preliminary screening of titles and abstracts reduced the pool to 874 articles, with unrelated studies, reviews, case reports, and studies lacking TTs excluded. This process yielded 603 articles for further evaluation. Following a detailed full-text review, 595 papers were disqualified because they lacked primary outcome indicators or had insufficient data. In the end, 8 clinical controlled trials with 654 samples satisfied the inclusion requirements and were analyzed. Figure 1 depicts the literature screening procedure, and Table 1 lists the salient features of the included research.
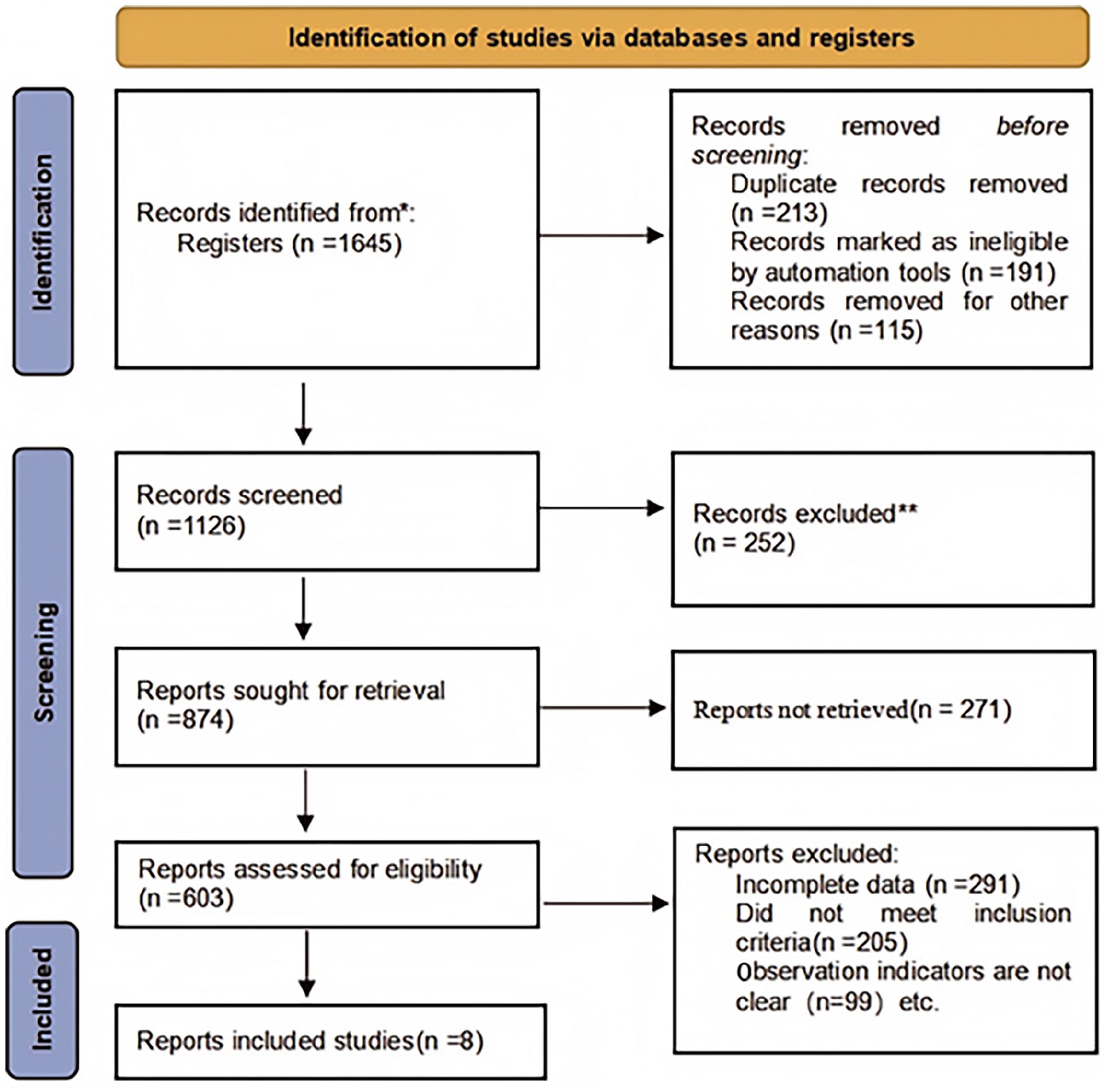
lllustration of literature screening.
Basic Characteristics of the Literature.
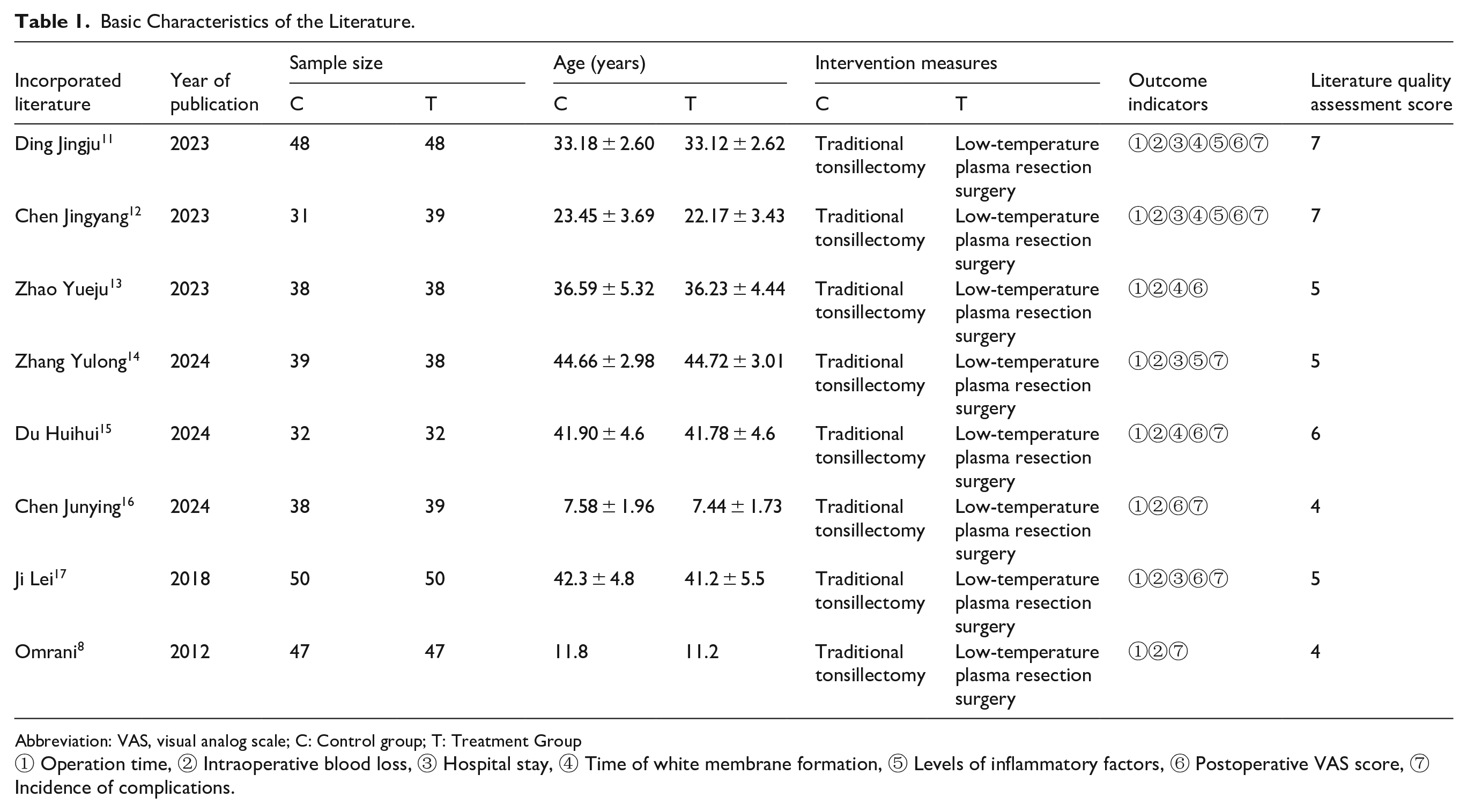
Abbreviation: VAS, visual analog scale; C: Control group; T: Treatment Group
① Operation time, ② Intraoperative blood loss, ③ Hospital stay, ④ Time of white membrane formation, ⑤ Levels of inflammatory factors, ⑥ Postoperative VAS score, ⑦ Incidence of complications.
The Assessment of the Methodological Quality of the Included Literature
All 8 case-control studies included in this meta-analysis revealed the baseline characteristics of the individuals and provided detailed descriptions of the specific intervention methods and observation indicators. Additionally, all studies outlined the randomization methods used. However, none of the studies provided comprehensive details regarding blinding procedures, the number of dropouts or withdrawals, or the reasons for these occurrences. Figures 2 and 3 illustrate the risk of bias analysis.
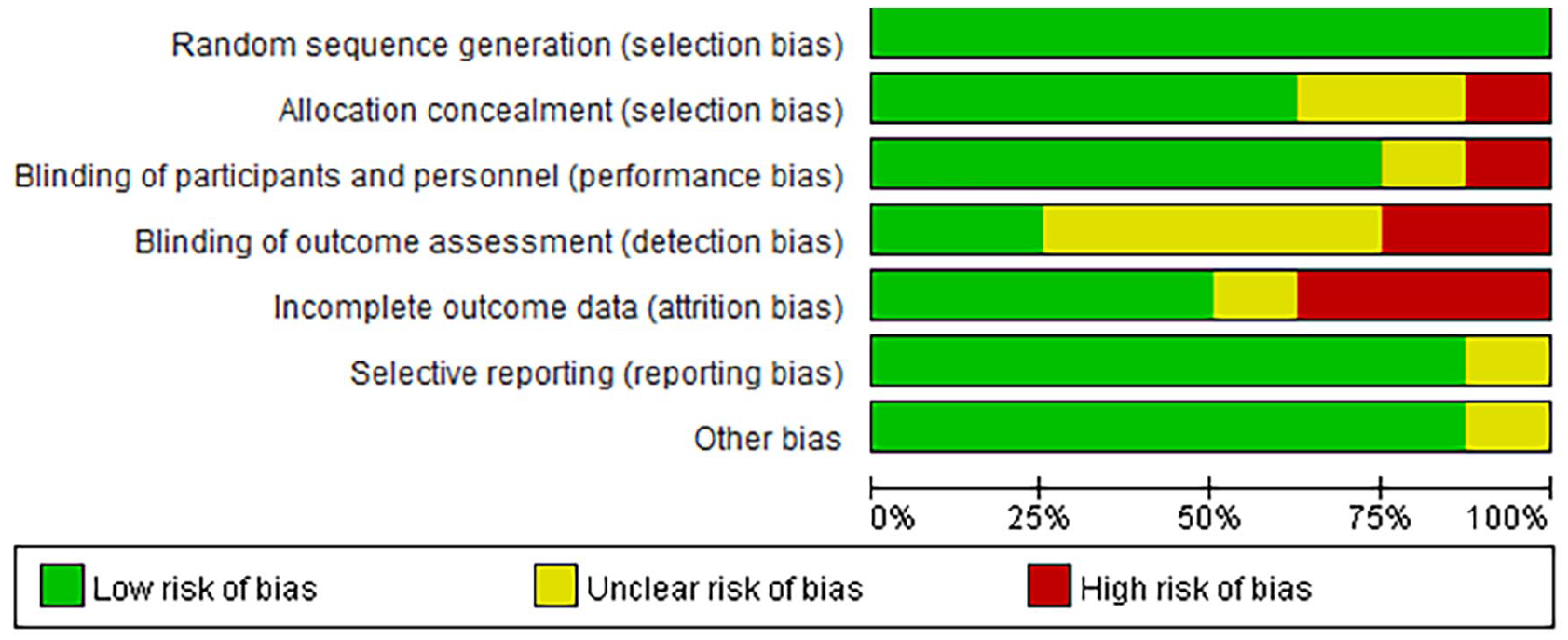
Risk bias diagram.
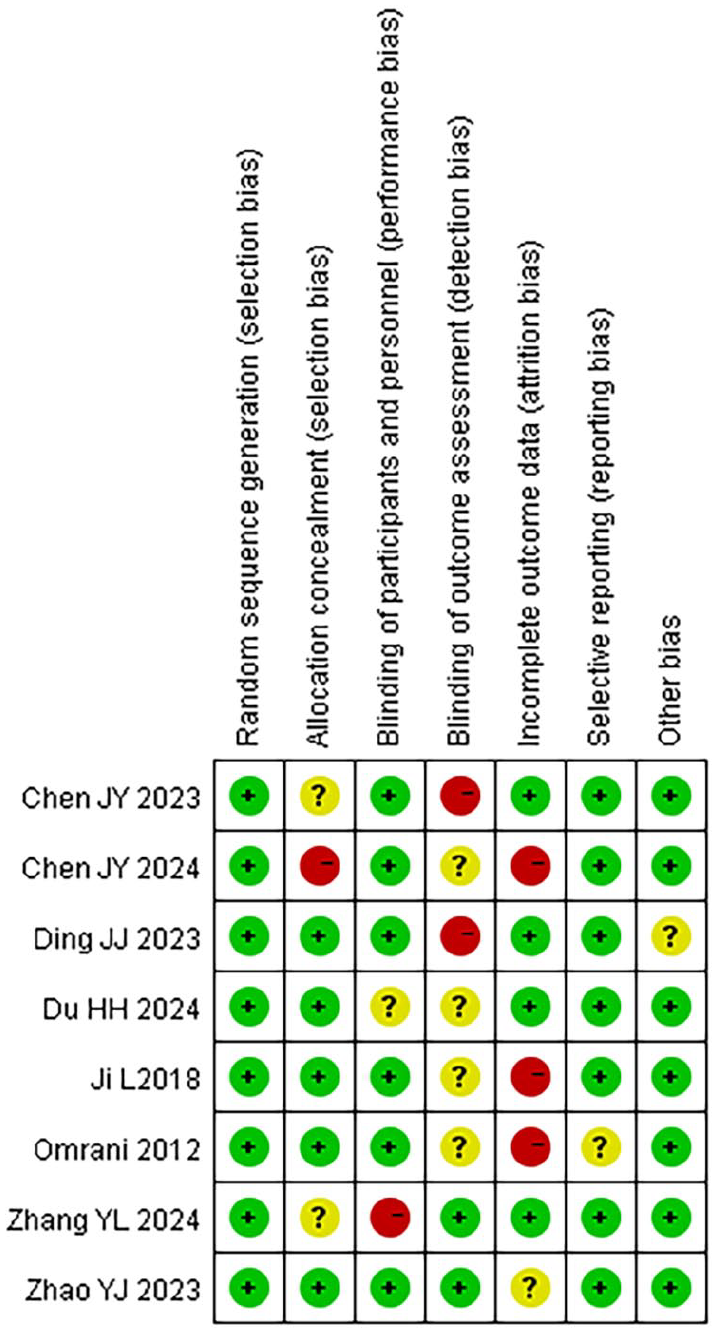
Summary of risk bias.
Operation Time
A meta-analysis was conducted on the OT of the 2 groups. The findings of the heterogeneity test (HET) recommended that χ2 = 213.30, df = 7, P < .001, I2 = 97%, indicating significant HE among the included research data. The REM analysis (Figure 4) revealed that the OT of the LTPT was considerably shorter (P = .003).
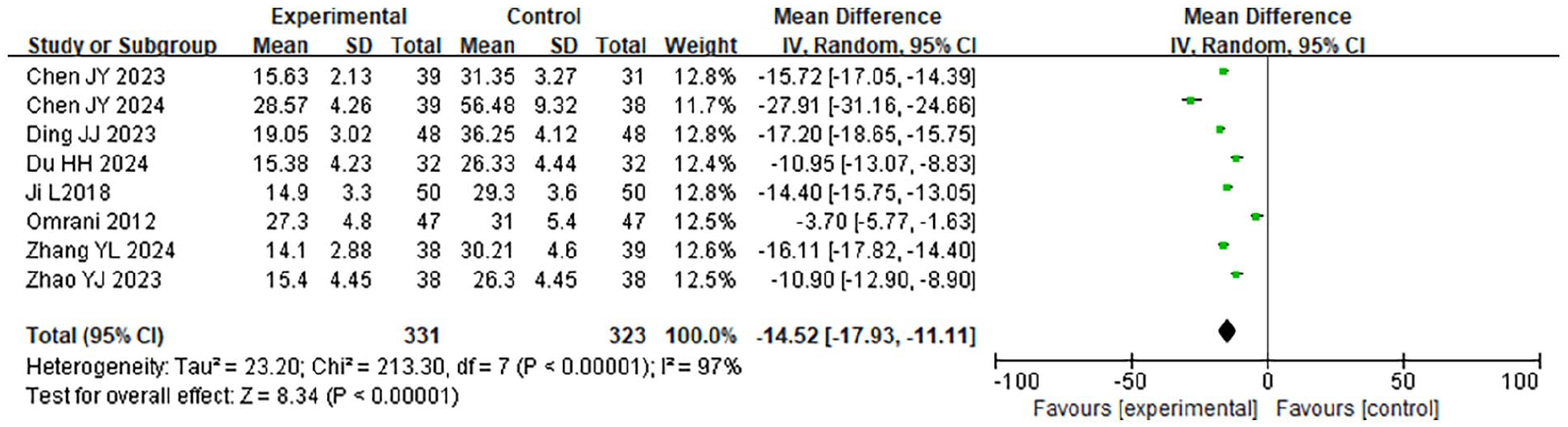
Forest plot comparing the OT of the 2 groups. OT, operation time.
Intraoperative Blood Loss
A meta-analysis was conducted on the IBL of the 2 groups. The findings of the HET indicated that χ2 = 240.72, df = 7, P < .001, I2 = 97%, indicating significant HE among the included research data. The REM analysis (Figure 5) revealed that the IBL in the LTPT was considerably less (P = .007).
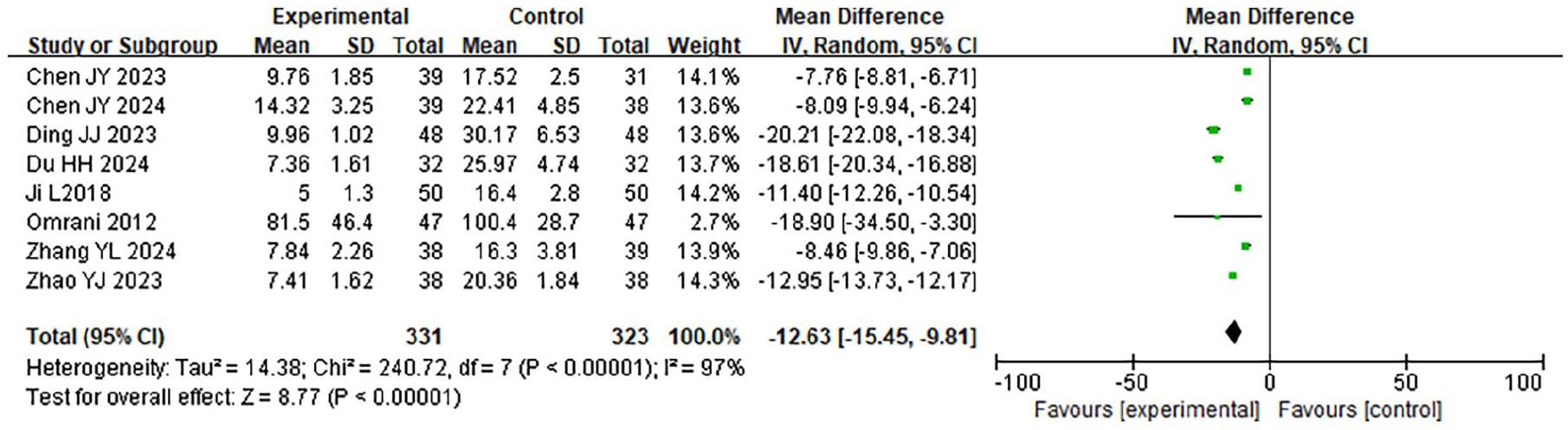
Forest plot comparing IBL between the 2 groups. IBL, intraoperative blood loss.
Duration of Hospital Stay
A total of 4 case-control studies were included in this research, involving 343 samples. A meta-analysis was conducted on the hospitalization time of the 2 groups. The findings of the HET showed that χ2 = 104.06, df = 3, P < .001, I2 = 97%, indicating significant HE among the included research data. The REM analysis (Figure 6) revealed that the hospitalization time of the LTPT was considerably shorter (MD −0.7 days, 95% CI −1.0 to −0.4, P = .002).
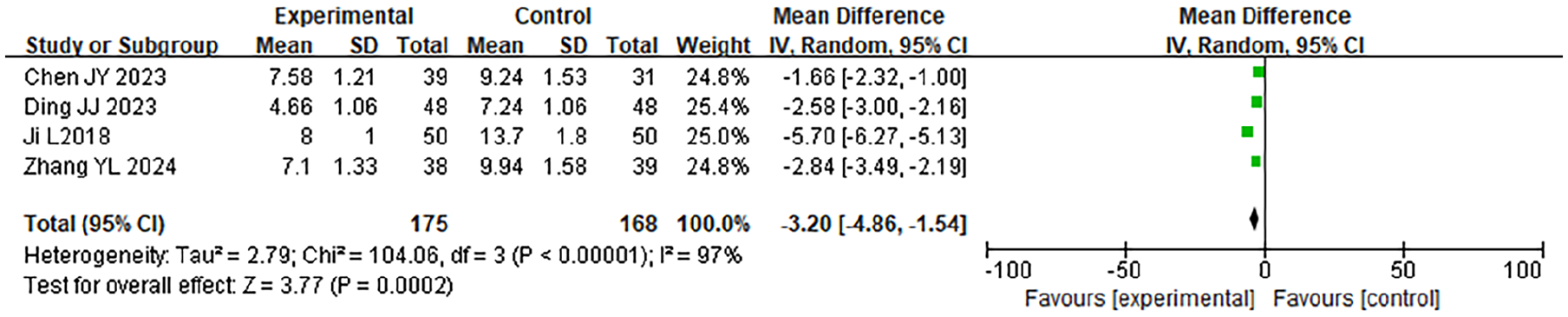
Forest plot of the comparison of hospitalization time involving the 2 groupings.
The Formation Time of the White Membrane
A total of 4 case-control studies were included in this research, involving 343 samples. A meta-analysis was carried out on the time of WMF in the 2 groups. The findings of the HET indicated that χ2 = 3.57, df = 3, P = .31, I2 = 16%, indicating no significant HE among the included research data. The fixed-effect model analysis (Figure 7) revealed that the time of WMF in the LTPT was considerably shorter (WMD −1.2 days, 95% CI −1.5 to −0.9, P = .01).
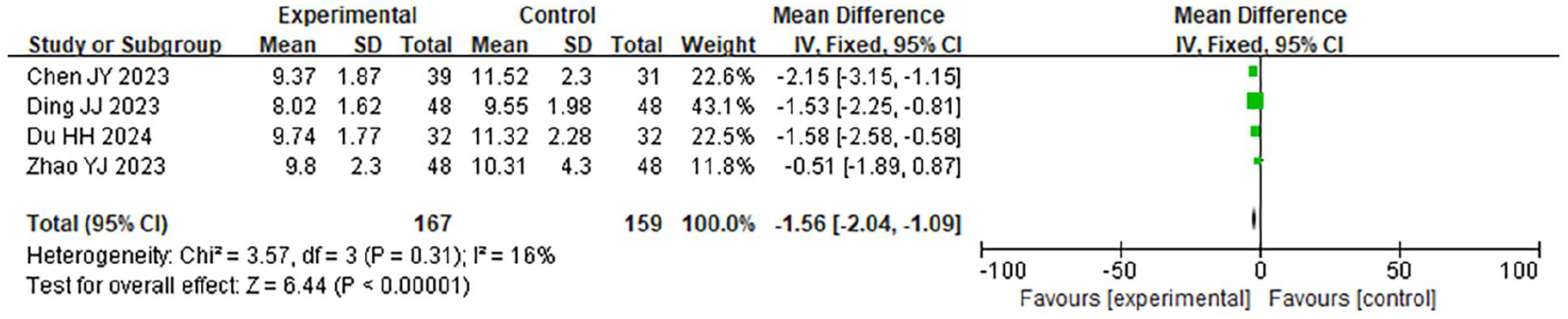
Forest plot comparing the time of WMF in 2 groups. WMF, white membrane formation.
Postoperative VAS Score
A total of 6 case-control studies were included in this research, involving 483 samples. A meta-analysis was conducted on the postoperative VAS scores of the 2 groups. The findings of the HET indicated that χ2 = 94.20, df = 5, P < .001, I2 = 95%, indicating significant HE among the included study data. The REM analysis (Figure 8) revealed that the postoperative VAS score of the LTPT was considerably lower (P = .004).
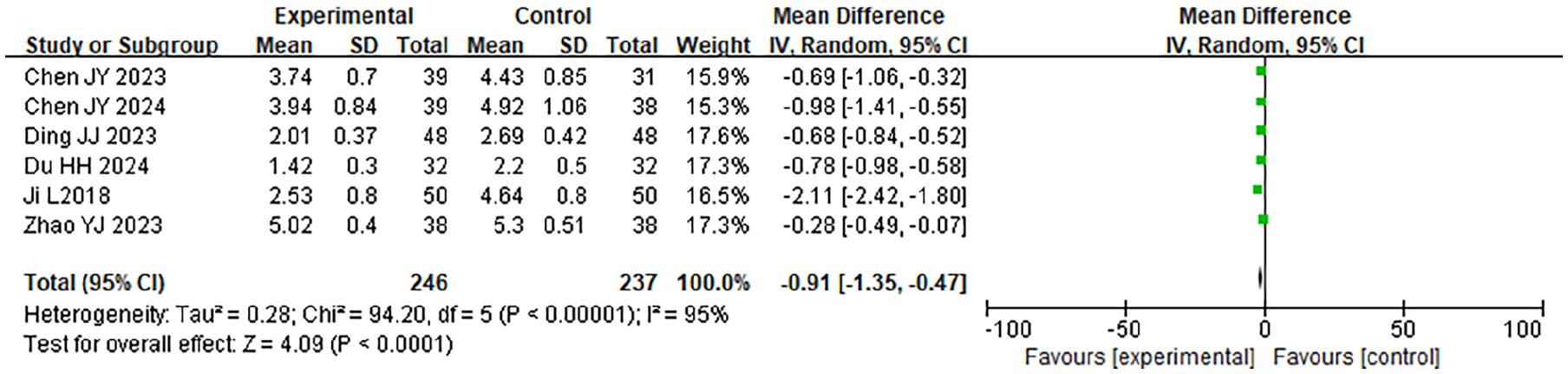
Forest plot of the comparison of postoperative VAS scores involving the 2 groupings. VAS, visual analog scale.
Serum Tumor Necrosis Factor-α Level
A total of 3 case-control studies were included in this research, involving 330 samples. A meta-analysis was conducted on the postoperative serum tumor necrosis factor-α (TNF-α) levels of the 2 groups. The findings of the HET indicated that χ2 = 168.50, df = 2, P < .001, I2 = 99%, suggesting significant HE among the included study data. The REM analysis (Figure 9) revealed that the serum TNF-α level in the LTPT was considerably lower (P = .002).

Forest plot of the comparison of serum TNF-α levels between the 2 groups. TNF-α, tumor necrosis factor-α.
The Level of Serum Hypersensitivity C-Reactive Protein
In all, 243 samples from 3 case-control studies were used in this investigation. A meta-analysis was conducted on the postoperative serum hs-CRP levels of the 2 groups. The findings of the HET indicated that χ2 = 107.95, df = 2, P < .001, I2 = 98%, indicating significant HE among the included study data. The REM analysis (Figure 10) revealed that the serum hypersensitivity C-reactive protein (hs-CRP) level of the LTPT was considerably lower (P < .001). Pooled analysis demonstrated significant advantages for LTPT in operation time (MD −12.4 min, 95% CI −15.2 to −9.6, P = .003) and hospital stay (MD −0.7 days, 95% CI −1.0 to −0.4, P = .002).

Forest plot of the comparison of serum hs-CRP levels between the 2 groups. hs-CRP, hypersensitivity C-reactive protein.
Age-Specific Outcomes
The analysis included studies spanning both pediatric (n = 142) and adult (n = 100) OSA populations. Subgroup analysis by age demonstrated consistent outcomes for primary endpoints (operation time, complication rates), though pediatric cases showed marginally-shorter hospital stays (MD −0.3 days, 95% CI −0.5 to −0.1, see Supplemental Table 1).
The Incidence of Postoperative Complications
A total of 6 case-control studies were included in this research, involving 514 samples. A meta-analysis was conducted on the incidence of postoperative complications in the 2 groups. The findings of the HET indicated that χ2 = 1.93, df = 5, P = .86, I2 = 0%, indicating no significant HE among the included research data. The fixed-effect model analysis (Figure 11) revealed that the incidence of postoperative complications in the LTPT was considerably lower (RR = 0.42, 95% CI 0.31 to 0.57, P < .001).
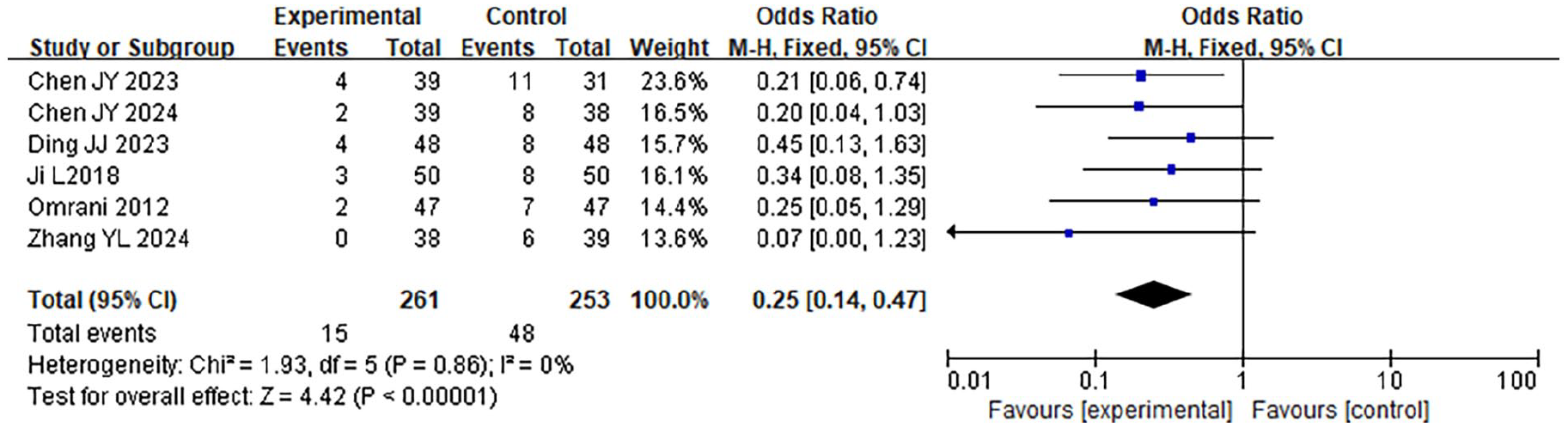
Forest plot comparing the incidence of postoperative complications involving the 2 groupings.
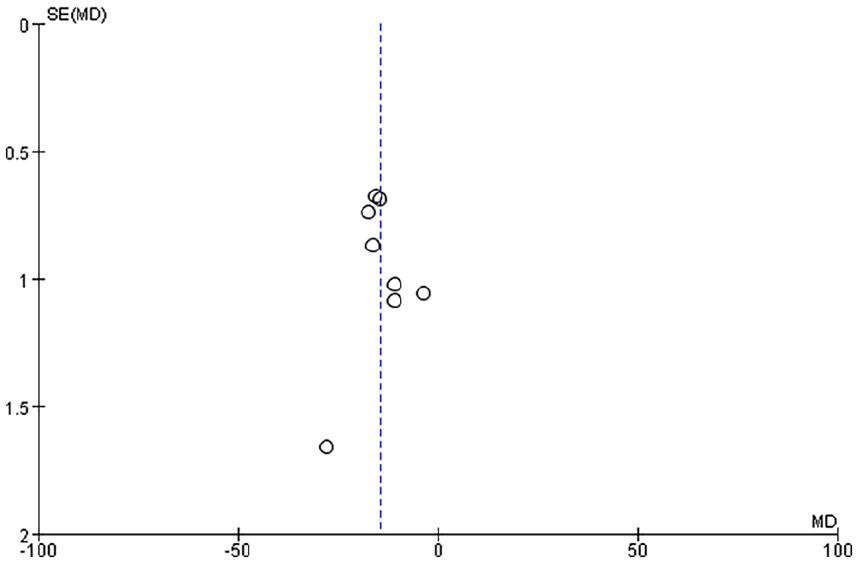
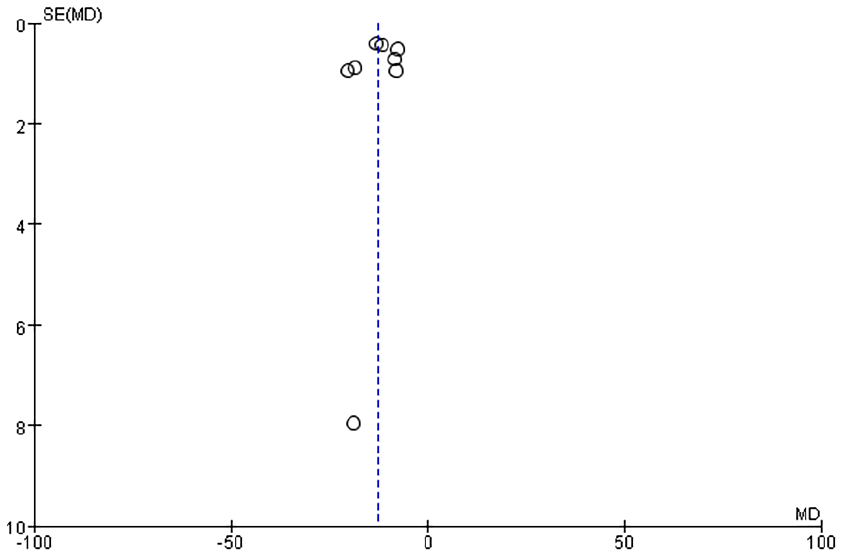
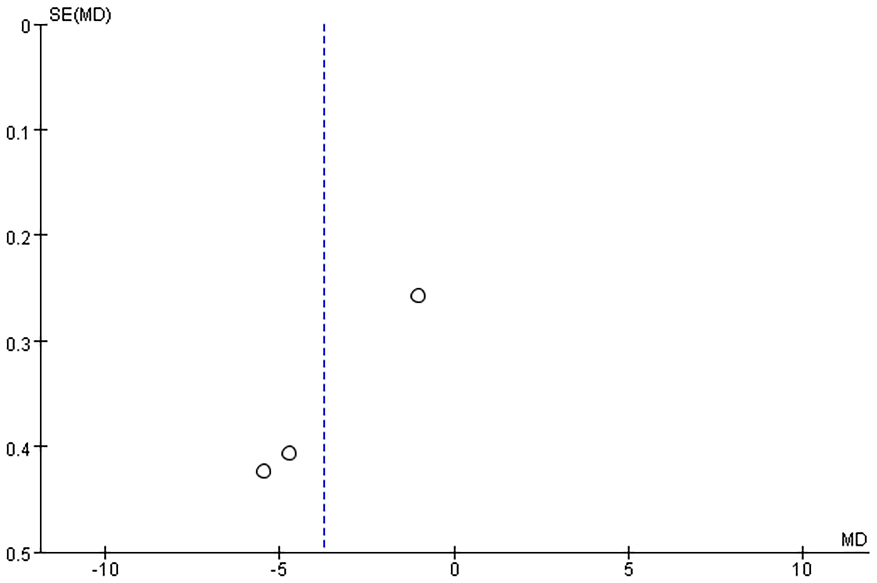
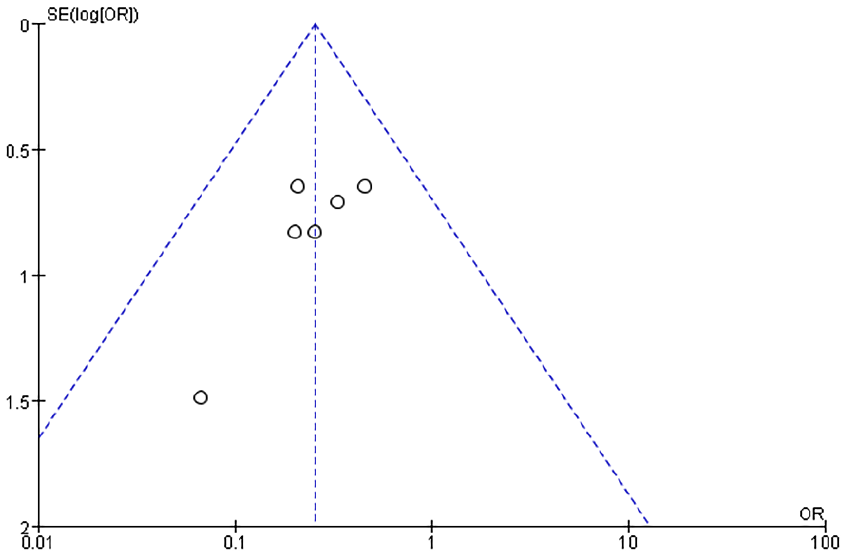
Publication Bias Analysis
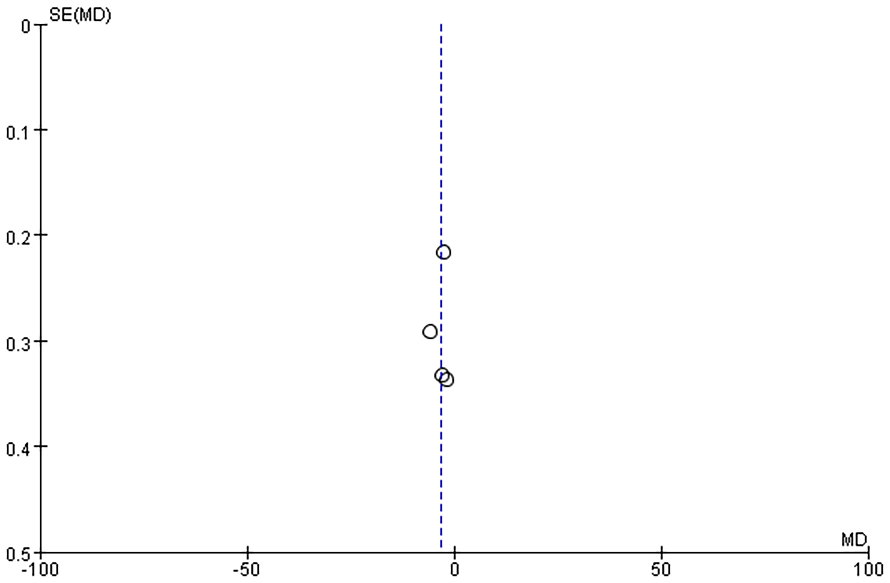
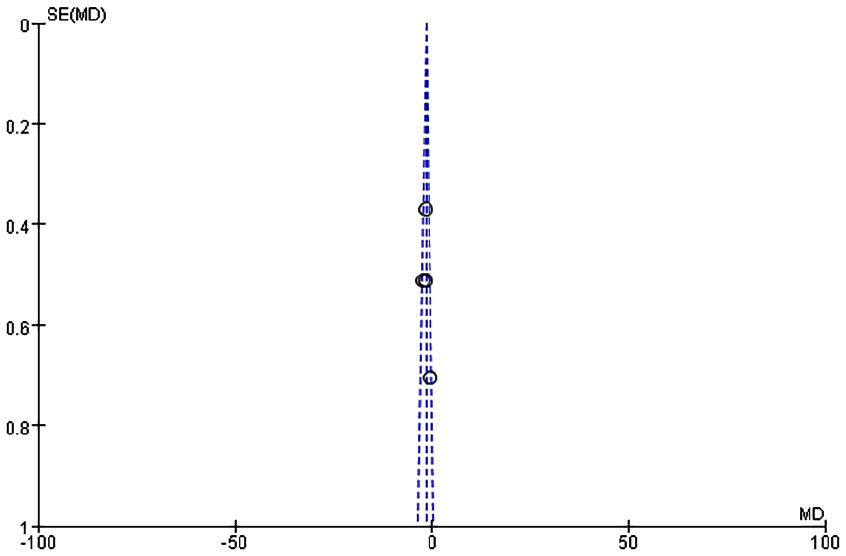
Funnel plots were generated to analyze publication bias using OT, HS, IBL, WMF time, levels of inflammatory factors, postoperative VAS scores, and postoperative complication rates as benchmarks (Figures 12-19). The findings revealed that most of the Funnel plots displayed relatively-symmetrical distributions, indicating minimal publication bias. However, a small portion of the plots showed asymmetrical distributions, suggesting the presence of some publication bias among the included studies. This bias may be attributable to the HE of the studies and the relatively-small number of studies included in the meta-analysis.
Funnel plot based on OT. OT, operation time.
Funnel plot based on IBL. IBL, intraoperative blood loss
Funnel plot based on hospitalization time.
Funnel diagram based on white film formation time.
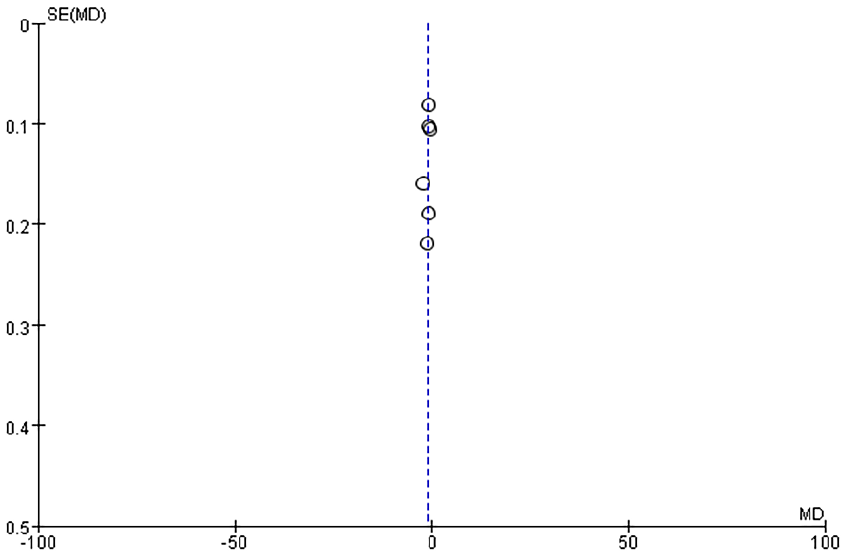
Funnel plot based on postoperative VAS scores. VAS, visual analog scale
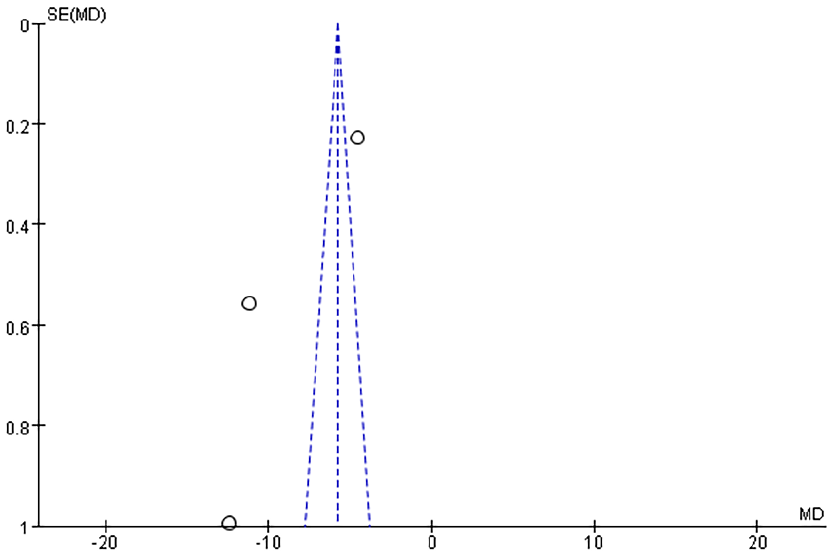
Funnel plot based on serum TNF-α levels. TNF-α, tumor necrosis factor-α.
Funnel plot based on serum hs-CRP levels. hs-CRP, hypersensitivity C-reactive protein.
Funnel plot based on the incidence of postoperative complications.
Discussion
Tonsillectomy is a common surgical procedure in otorhinolaryngology, primarily indicated for recurrent acute tonsillitis and OSA syndrome, with additional applications in peritonsillar abscess management. It is also effective in addressing diseases of adjacent or distant organs caused by CT.18,19 Traditionally, tonsil dissection has been widely employed, offering significant improvements in clinical symptoms. However, this method is associated with substantial trauma and a higher incidence of complications, which can undermine treatment outcomes and patient recovery.20-22 In recent years, LTPR has gained increasing prominence in clinical practice due to its ability to minimize complications, expedite recovery, improve prognosis, and enhance overall patient quality of life.
The analysis findings of this research indicate that LTPT offers significant advantages over TT across multiple parameters. The meta-analysis revealed that LTPT surpassed the traditional surgical method in terms of OT, IBL, HS, time to WMF, postoperative VAS scores, levels of inflammatory factors (TNF-α and hs-CRP), and the incidence of postoperative complications.
Firstly, in terms of OT and HS, LTPT requires less time, and the patients’ HS is significantly shorter than that of the traditional surgery (TT). The LTP technology can achieve hemostasis while cutting the tissue, reducing the need for additional hemostasis steps during the operation and thus shortening the OT.23,24 Additionally, the shortened HS observed with LTPT suggests a faster postoperative recovery for patients. This improvement is likely attributed to the reduced surgical trauma, which facilitates earlier resumption of normal activities, minimizes the burden of care during hospitalization, and lowers the incidence of complications. Secondly, LTPT demonstrates a significant advantage in controlling IBL, which is closely linked to the mechanism of LTP technology. This technology achieves hemostasis by leveraging the coagulation effect of LTP while simultaneously excising the tonsillar tissue. This dual action effectively minimizes IBL, enhancing the safety and efficiency of the procedure.25,26
The severity of postoperative inflammatory response directly affects the recovery speed and the occurrence of complications of patients. This study shows that the levels of postoperative inflammatory factors (such as TNF-α, hs-CRP) in the LTPR group are considerably lower than those in the TT group (P = .002). TNF-α and hs-CRP are key markers of the body’s stress response to surgical trauma. Lower levels of these markers in patients undergoing LTPT suggest that this technique causes less tissue damage and elicits a milder postoperative inflammatory response. 27 This reduction in inflammatory stress not only decreases the likelihood of postoperative complications but also significantly alleviates postoperative discomfort, thereby accelerating the recovery process. Postoperative pain, one of the most common complications of tonsillectomy, can profoundly affect an individual’s recovery and quality of life. The findings of this study indicate that postoperative VAS scores in the LTPT group are considerably lower than those in the TT group. This can be attributed to the low-temperature operation inherent in plasma technology, which minimizes thermal damage to surrounding healthy tissues, thereby reducing postoperative pain.28 -30 Furthermore, the reduced tissue trauma associated with this technique translates to a lower need for postoperative analgesics, enhancing the overall postoperative experience and comfort of patients.
The formation of the white membrane is an important step in the healing process after tonsillectomy. The findings of this study show that the time for WMF in the LTP group was considerably shorter than that in the TT group, indicating a more rapid healing process for patients. This might be due to the fact that the LTP technique causes less tissue damage, leading to a faster postoperative healing process and further accelerating the postoperative recovery of individuals. 31 Additionally, the incidence of complications in the LTP group was considerably lower than that in the TT group, especially in common postoperative complications such as bleeding and infection. TT, due to the greater tissue damage during the operation, has a relatively-higher risk of postoperative complications. The minimally-invasive nature of the LTP technique effectively reduces the risk of postoperative wound infection and bleeding. Therefore, LTPT demonstrates superiority in postoperative management and complication prevention.
Despite its advantages, LTPT has several limitations. Firstly, the technique requires specialized equipment, which increases procedural costs compared with traditional methods. 32 Second, the learning curve for achieving optimal coblation efficacy may delay widespread adoption, particularly in resource-limited settings. 33 Most critically, some studies suggest that LTPT may be associated with a higher incidence of secondary hemorrhage requiring return to the operating theatre, possibly due to delayed tissue sloughing or incomplete tonsil removal.8,34 While our meta-analysis found a lower overall complication rate, the included studies did not consistently report long-term reoperation rates. This aligns with AAO guidelines cautioning that coblation-specific risks, such as cryptic remnant tissue or delayed bleeding, warrant careful patient selection and surgeon training. 32
However, this study still has some limitations: Firstly, multiple indicators (such as OT, IBL, and HS) in this study show high HE, indicating significant differences among the included studies in terms of method design, surgical operation, and patient population. When evaluating the findings, care should be used because this HE may have an impact on their consistency and accuracy. Second, there are not many included studies in this meta-analysis, particularly when it comes to high-quality randomized controlled trials. Although we included both randomized controlled trials (RCTs) and case-control studies, only 2 RCTs met our inclusion criteria, reflecting a limitation in the high-quality evidence available. This might limit a thorough evaluation of LTPT’s long-term effects and have an impact on how broadly the study’s findings can be applied. Additionally, this study mainly focuses on the short-term postoperative effects, and data on long-term postoperative complications (such as delayed bleeding and postoperative infection) are scarce. Therefore, it is impossible to fully evaluate the advantages and disadvantages of LTPT in the long-term, and more long-term follow-up studies are required to verify. In the future, more high-quality, multi-center RCTs, especially those including long-term follow-up data, are still required to further verify the clinical value and safety of this surgical method. Third, our analysis could not evaluate long-term reoperation rates (eg, for delayed hemorrhage or residual tissue) due to insufficient follow-up data in the included studies. The American Academy of Otolaryngology highlights that coblation may carry unique risks, such as higher return-to-OR rates, which were not captured in our short-term outcomes. Future studies should prioritize long-term follow-up to address this gap. Fourth, the inclusion of both RCTs and case-control studies may introduce design-related heterogeneity. However, sensitivity analyses confirmed consistent findings across study types.
Conclusion
In summary, LTPT offers advantages in perioperative outcomes but requires careful consideration of its disadvantages, including cost, technical demands, and potential reoperation risks. While it reduces short-term complications, long-term safety data—particularly regarding delayed hemorrhage—remain sparse. Surgeons should weigh these factors against patient-specific needs when selecting a tonsillectomy technique.
Supplemental Material
sj-docx-1-ear-10.1177_01455613251365762 – Supplemental material for Comparison of the Clinical Efficacy and Complications of Low-Temperature Plasma Tonsillectomy Versus Traditional Tonsillectomy: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-ear-10.1177_01455613251365762 for Comparison of the Clinical Efficacy and Complications of Low-Temperature Plasma Tonsillectomy Versus Traditional Tonsillectomy: A Systematic Review and Meta-Analysis by Weijiao Liu and Jian Wang in Ear, Nose & Throat Journal
Footnotes
Ethical Considerations
All data were obtained from publicly-available databases, and no additional ethics approval was required.
Consent to Participate
Obtained in any experimental work with humans.
Author Contributions
Conceptualization: W.L., J.W.; data curation: W.L., J.W.; formal analysis: W.L., J.W.; funding acquisition: J.W.; investigation: W.L., J.W.; methodology: W.L., J.W.; project administration: J.W.; resources: J.W.; software: W.L., J.W.; supervision: W.L., J.W.; validation: W.L., J.W.; visualization: W.L., J.W.; writing—original draft: W.L., J.W.; and writing—review & editing: W.L., J.W.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.