
Abstract
Objectives:
First-line treatment of chronic rhinosinusitis includes topical corticosteroids aimed at decreasing inflammation of sinonasal mucosa. No guidelines exist regarding the effect of head position during administration of corticosteroids. We hypothesize certain positions enhance delivery to the paranasal sinuses, with further improvement in delivery after sinus surgery.
Methods:
A systematic review of the literature was conducted using Medline Ovid, Embase, Scopus, and Cochrane databases. All studies evaluating intranasal medications administered in 2 or more head positions were included. Study population, head position(s), method/volume of delivery, and outcome metrics were recorded.
Results:
Twenty-four studies compared head positions and their role in distribution of intranasal medication. Of 12 papers studying surgically naive subjects, 6 found improvement in delivery to specific sinonasal regions (middle meatus; lateral, superior, or posterior nasal cavity) and/or symptomatic improvement, in the lying head back (LHB) or head down and forward (HDF) positions, but only 3 reached statistical significance. Of 12 papers studying surgically altered patients, 10 found delivery improved in the HDF, LHB, and head forward 45° or 90° positions. Of 5 studies of extended frontal sinus procedures (Draf IIb/III), a majority found distribution to the frontal sinus improved with the head forward 90° position. Patients found the HDF position most uncomfortable.
Conclusions:
Studies found no statistically significant difference in distribution to unoperated sinuses among different head positions. A minority of studies supported the use of the LHB and HDF positions. This suggests that in surgically naive patients, intranasal corticosteroid delivery to sinonasal regions and/or symptomatic improvement may be best achieved with the sinuses positioned inferior to the delivery device. Surgery improved distribution to the paranasal sinuses regardless of head position, although tilting the head forward 90° was particularly effective in delivery to the frontal sinus after extended frontal sinus procedures.
Introduction
Chronic rhinosinusitis (CRS) is a prevalent condition 1 -4 characterized by chronic inflammation, not explained by infection alone, in combination with 2 or more nasal symptoms (nasal blockage, nasal discharge, reduced sense of smell, facial pain) for greater than 12 weeks. 5 In the United States, estimated direct and indirect costs of CRS run at $12.8 billion with 260 000 sinus surgeries performed per year. 6,7 Corticosteroids, applied as drops, sprays, or irrigations, are a first-line treatment for CRS. Direct application of steroids enhances their local anti-inflammatory activity while avoiding undesirable systemic side effects. 8
The efficacy of intranasal corticosteroid administration is dependent upon contact of the drug with sinonasal mucosa. Surgical status of the sinuses, volume delivered, method of delivery, and head position during administration may affect delivery and efficacy. Although various head positions for administration of intranasal medications have been studied, we lack consensus on an optimal head position. 9,10 The International Consensus Statement on Allergy and Rhinology: Rhinosinusitis (ICAR: RS) reports improved delivery of intranasal medications postoperatively and with high-volume devices regardless of patient position, but the impact of head position in low-volume devices remains unknown. 11 Head position may influence delivery in both the surgery-naive and the postoperative patient and have varying effects as a result of volume delivered (low volume such as spray or drops, or high volume such as irrigations).
The goal of this review is to examine the role of head position in the installation of intranasal corticosteroids. We also aim to elucidate the interaction between surgery and head position. We hypothesize that certain head positions can improve delivery of medication to the paranasal sinuses, increasing their efficacy in CRS treatment, with sinus surgery further improving delivery.
Methods
A medical librarian conducted a literature search on June 11, 2020, in the Medline Ovid, Embase, Scopus, and Cochrane databases. The strategy was initially developed in Medline Ovid (see Supplement 1) using Medical Subject Heading (MeSH) headings and/or keyword equivalents for Adrenal Cortex Hormones; Glucocorticoids; Administration, Intranasal; Nose; Nasal Cavity; Paranasal Sinuses; Posture; and Head-down Tilt. This strategy was translated to the other databases, yielding 1921 results after de-duplication. Articles with irrelevant subject matter, case reports, abstracts or incomplete papers, letters to the editor, reviews, and animal studies were excluded. Only studies assessing 2 or more head positions were included in the review. Two authors (E.L.C. and S.N.F.) reviewed the full text of the remaining articles for inclusion.
Data extracted and recorded using a REDCap survey instrument included: (1) study population, (2) head position(s) studied, (3) method of delivery, (4) distribution of the medication, (5) grading criteria applied, (6) outcomes measured. 12,13
Results
Twenty-four articles met the inclusion criteria; see Figure 1 for full PRISMA diagram. All trials used intranasal corticosteroids or dyed fluids. Studies included healthy patients, patients with sinonasal disease, cadavers, 3D models, and computational fluid dynamics (CFD) studies.
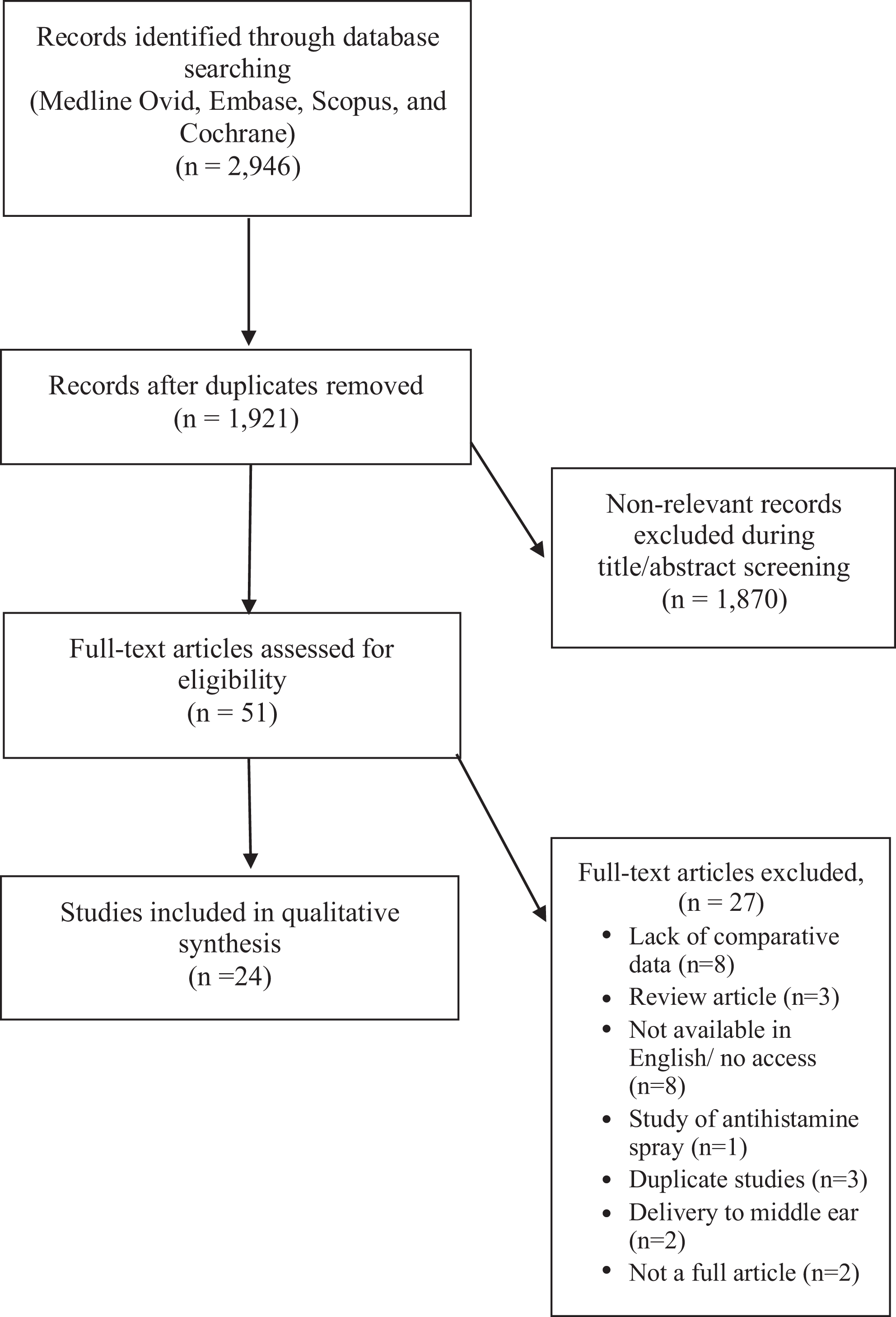
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) diagram adapted from Moher et al. 14
Commonly Studied Head Positions
Head down and forward (HDF) or vertex-to-floor or Mecca position involves kneeling on the floor, with the top of the head on the ground and nostrils facing upward. Lateral head low or Ragan position involves lying on the side with chin pointed up toward the opposite shoulder. Intranasal medication is instilled in the lower nostril. Lying head back (LHB) or Mygind’s position involves lying supine with head hanging in hyperextension, with the chin raised. Vertex or head-forward or head tilted 90° forward involves sitting or standing with the head tilted 90° forward with the crown of the head in a plane perpendicular to the wall (Figure 2).
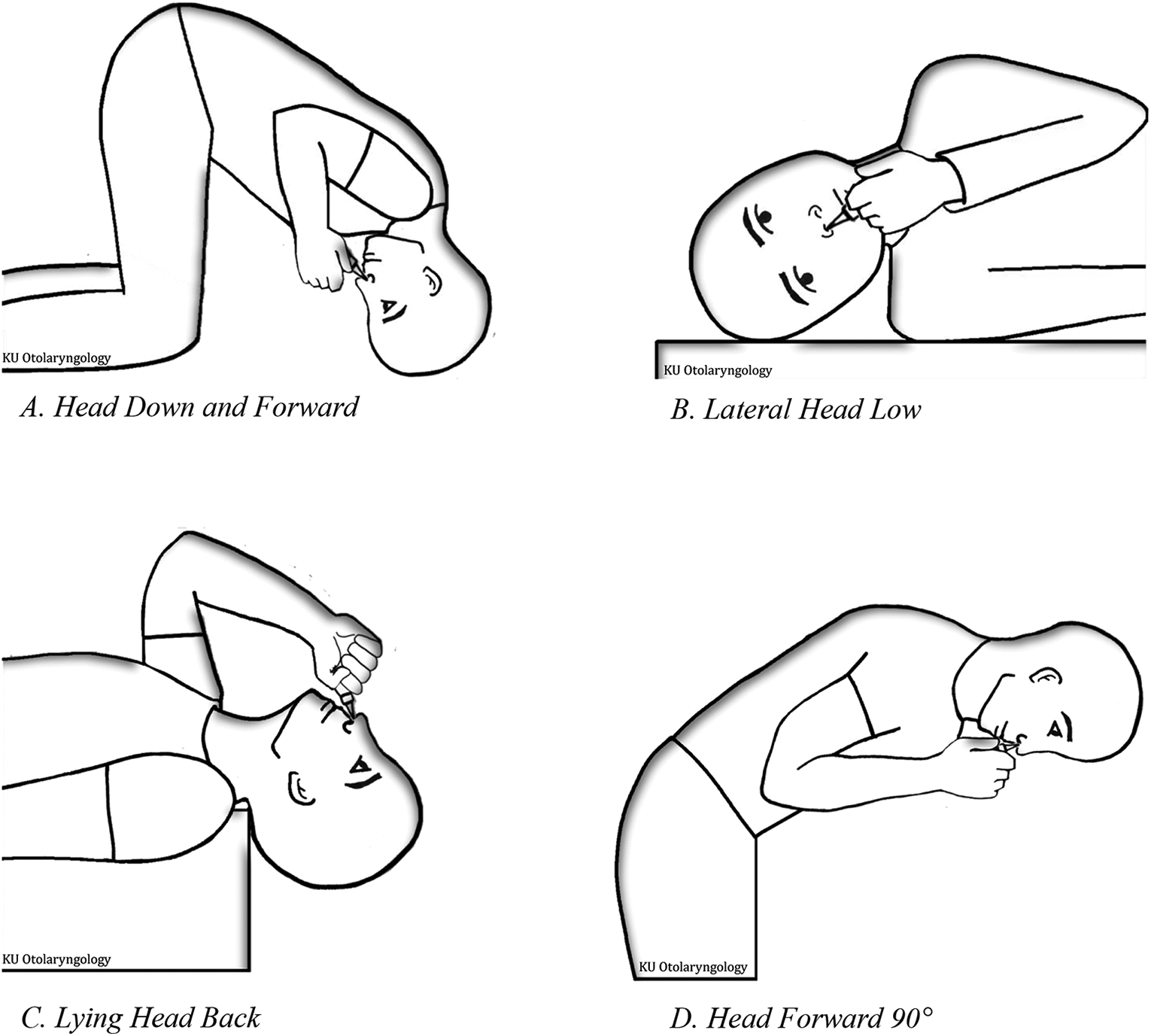
Illustration of head positions. 1. Head down and forward or vertex-to-floor or Mecca position (HDF): kneeling on the floor, with the top of the head on the ground and nostrils facing upward. 2. Lateral head low or Ragan position (LHL): lying on the side with chin pointed up toward the opposite shoulder. Intranasal medication is instilled in the lower nostril. 3. Lying head back or Mygind’s position (LHB): lying supine with head hanging in hyperextension, with the chin raised. 4. Vertex or head-forward or head tilted 90° forward: sitting or standing with the head tilted 90° forward with the crown of the head in a plane perpendicular to the wall.
Outcome Metrics
Twenty-two of 24 studies evaluated visual, endoscopic, or computer-simulated delivery of fluid, with or without dye, to specific sinonasal regions, or improvement in appearance of nasal polyps on examination. Two studies assessed symptomatic improvement, SNOT-22 and Lund-Kennedy scores. 15,16
Surgery Naive Patients and Head Position
Twelve studies assessed the effect of head position on delivery of intranasal medications in surgery naive patients; these included 6 studies of healthy patients, 2 of patients with sinonasal disease, 3 CFD studies, and 1 cadaver study (Table 1). 16 -27 Six studies found improved delivery to various sinonasal regions and/or symptomatic improvement based on head position, 16,20,21,23,24,26 but only 3 reached statistical significance. 16,20,26 Patients with sinonasal disease reported improvement in nasal discharge, blockage, and facial pain with drops instilled in the HDF position, held for 2 minutes. 16 One study of healthy patients found both the HDF and LHB position, held for 30 seconds, to improve delivery of drops to the middle meatus. 20 One CFD study found the LHB position improved delivery of spray to the posterior nasal cavity with no inspiratory airflow. 26 Four studies found no significant improvement in distribution between head positions. 17,18,22,27 No studies included in this review compared high-volume to low-volume delivery in surgically naive patients, and there was no significant difference in the distribution of drops versus sprays. 18
Effect of Head Position in Surgery Naive Patients.
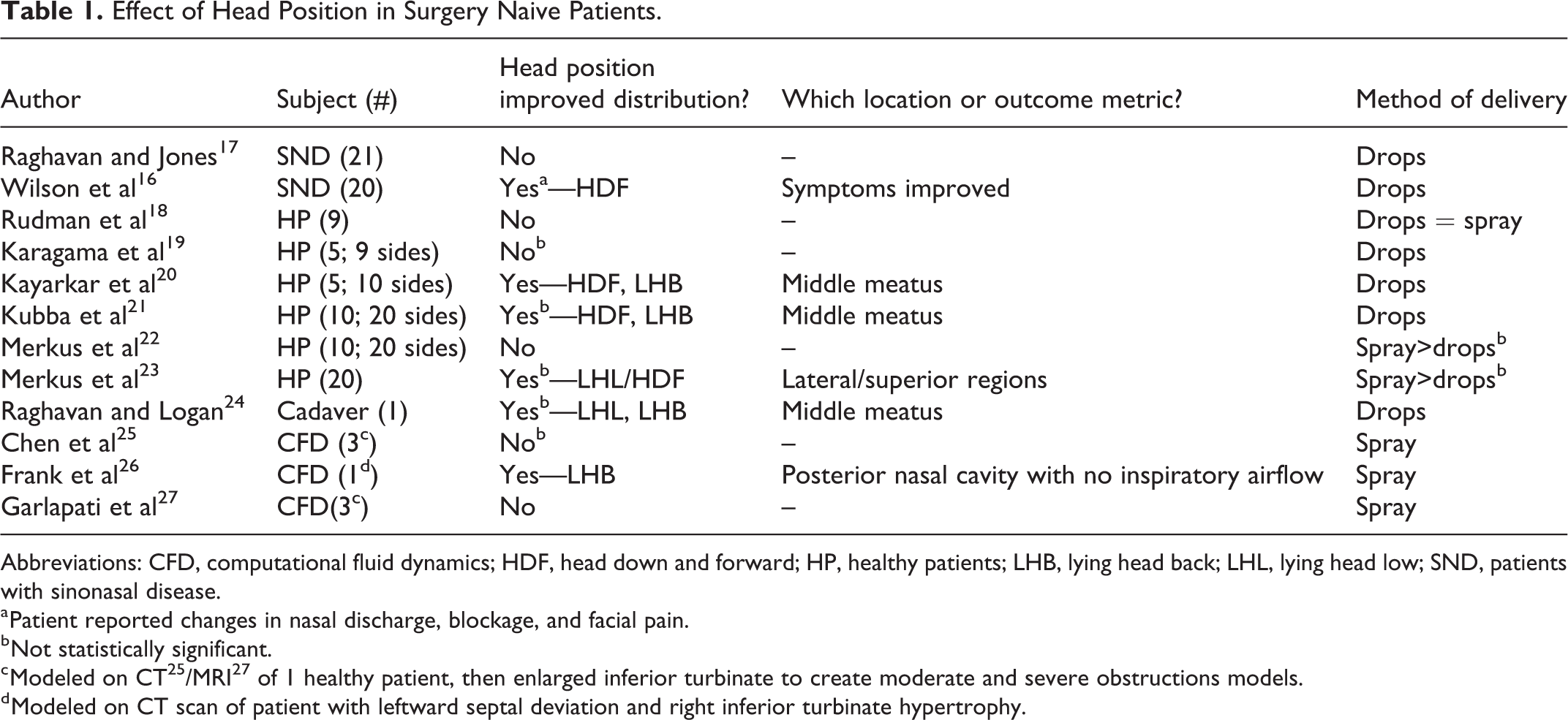
Abbreviations: CFD, computational fluid dynamics; HDF, head down and forward; HP, healthy patients; LHB, lying head back; LHL, lying head low; SND, patients with sinonasal disease.
a Patient reported changes in nasal discharge, blockage, and facial pain.
b Not statistically significant.
c Modeled on CT 25 /MRI 27 of 1 healthy patient, then enlarged inferior turbinate to create moderate and severe obstructions models.
d Modeled on CT scan of patient with leftward septal deviation and right inferior turbinate hypertrophy.
Surgery and Head Position
Twelve studies assessed the effect of surgery and head position on delivery of medication; these included 4 studies of patients with sinonasal disease, 6 cadaver studies, 2 CFD studies, and 1 study of a 3D-printed model (Table 2). 15,28 -38 Six studies addressed standard functional endoscopic sinus surgery (FESS) including maxillary antrostomy, total ethmoidectomy, sphenoidotomy, and frontal sinusotomy. 15,33 -35,37,38 Two studies addressed extended maxillary sinus surgery, including mega and extended modified mega-antrostomy 36 or creating the widest possible opening, 30 while 5 examined extended surgery of the frontal sinus. 28 -32 Extended frontal sinus surgery was defined as Draf IIb and Draf III procedures.
Effect of Head Position and Surgery.
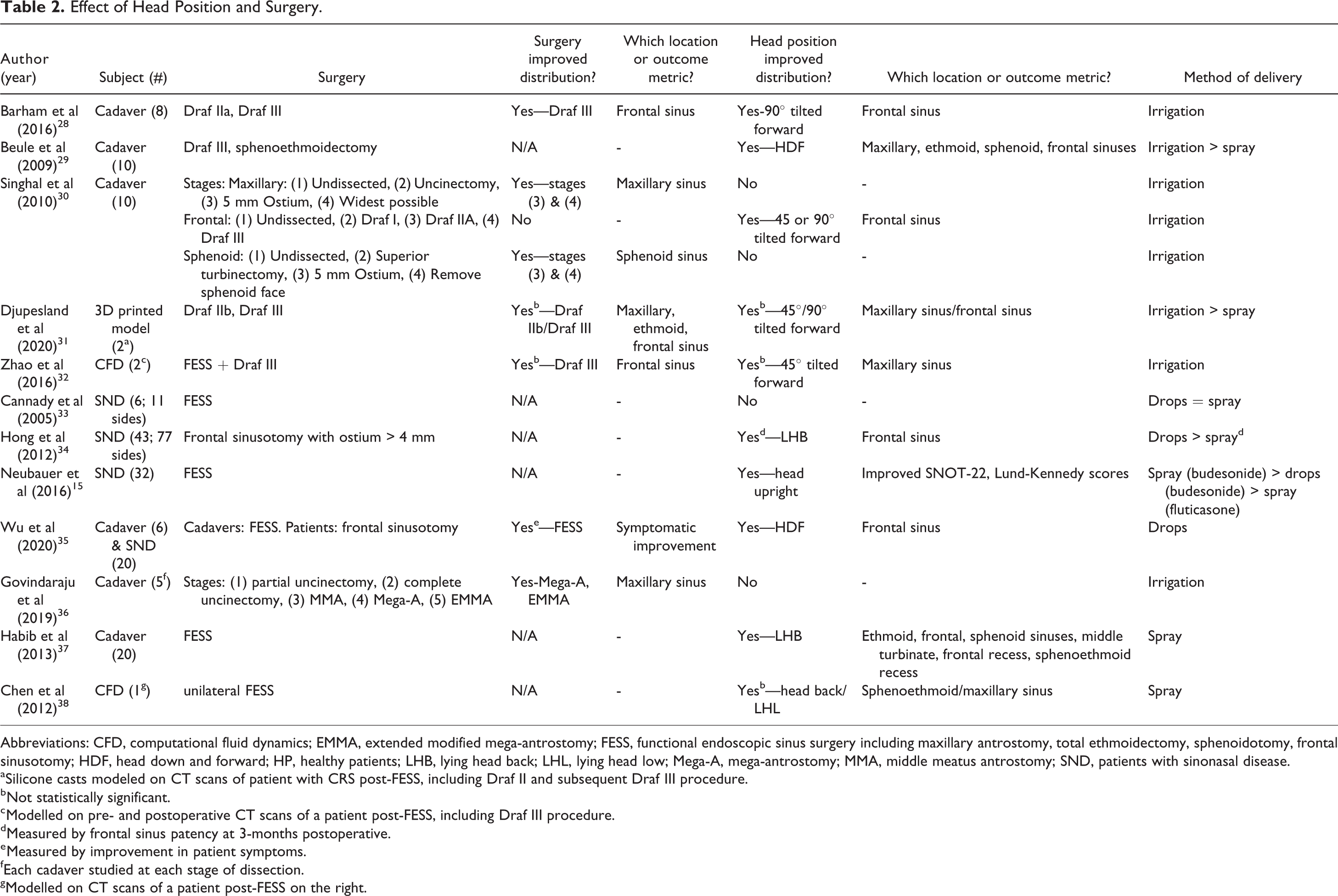
Abbreviations: CFD, computational fluid dynamics; EMMA, extended modified mega-antrostomy; FESS, functional endoscopic sinus surgery including maxillary antrostomy, total ethmoidectomy, sphenoidotomy, frontal sinusotomy; HDF, head down and forward; HP, healthy patients; LHB, lying head back; LHL, lying head low; Mega-A, mega-antrostomy; MMA, middle meatus antrostomy; SND, patients with sinonasal disease.
a Silicone casts modeled on CT scans of patient with CRS post-FESS, including Draf II and subsequent Draf III procedure.
b Not statistically significant.
c Modelled on pre- and postoperative CT scans of a patient post-FESS, including Draf III procedure.
d Measured by frontal sinus patency at 3-months postoperative.
e Measured by improvement in patient symptoms.
f Each cadaver studied at each stage of dissection.
g Modelled on CT scans of a patient post-FESS on the right.
Six papers compared outcomes between unoperated and postsurgical patients, or between 2 or more types of surgeries. 28,30 -32,35,36 Three found significant improvement in delivery with increased level of dissection and high-volume delivery, 28,30,36 while one found improvement with increased dissection and use of drops in the HDF position for 1 minute. 35 The remaining 2 found delivery positively correlated with level of dissection using irrigation, although this difference did not reach statistical significance. 31,32
Five studies evaluated the effect of extended frontal sinus procedures. Distribution to the frontal sinus improved with the head forward 90° position using irrigations. 28,30,31 Two studies included extended maxillary procedures and neither found any impact of head position on distribution, both using irrigations. 30,36 Two studies compared high-volume delivery to low-volume sprays and found significantly improved distribution in the high-volume groups. 29,31 Three studies of surgical patients compared delivery of sprays to drops, with one study finding no difference between the 2, with spray delivered in the Head Upright (HUR) position, compared to drops in the HDF position, held for 1 or 5 minutes, 33 one finding improved frontal sinus patency at 3 months postop with the use of drops in the LHB position for 5 minutes, 34 and one finding budesonide spray significantly improved patient SNOT-22 and Lund-Kennedy scores compared to fluticasone spray, both delivered in the HUR position. 15 Budesonide drops, delivered in the HDF position held for 1 minute fell in between these 2 sprays in terms of symptomatic improvement.
Discussion
The ICAR: RS position statement recommends the use of intranasal corticosteroids for CRS with and without nasal polyposis in the standard formulation (spray). 11 Their review shows very limited delivery of intranasal medications to unoperated sinuses regardless of head position, but the HDF position improves distribution in postoperative patients. Our review had similar findings.
Surgery Naive Patients and Head Position
This review revealed more studies (4) finding no significant difference in outcomes between head positions in surgically naive patients than those that did (3), corresponding with the ICAR: RS recommendations. Of the 3 papers that reached statistical significance, one found that the HDF and LHB back positions held for 30 seconds improved distribution of nasal drops to the middle meatus, 20 while another found the LHB position improved distribution to the posterior nasal cavity with no airflow in a computer simulated trial. 26 The third paper found drops instilled in the HDF position held for 2 minutes significantly improved patient-reported changes in nasal discharge, blockage, and facial pain, but did not result in change appearance of nasal mucosa on examination. 16 These findings suggest that in the unoperated sinuses, instilling medication with the sinuses inferior to the delivery device may allow gravity to improve penetration, but this requires further investigation. None of the surgically naive patients received high-volume delivery methods, although prior studies have shown that corticosteroid irrigations are effective for such patients. 39,40
Surgery and Head Position
The literature largely supports that increased dissection results in improved delivery of intranasal medications, 41 -43 although a few studies show equivalence in delivery with slightly less dissection. 44 A study by Harvey et al found FESS improved delivery, particularly to the frontal and sphenoid sinuses, 41 while a study by Bhalla et al found irrigation distribution to the frontal sinus after Draf IIb with superior septectomy equivalent to the Draf III procedure. 44 Our review is concordant with increased surgery resulting in improved delivery; 4 of 6 papers comparing either pre- and postoperative distribution or varying levels of dissection showed significantly improved penetration to both frontal and maxillary sinuses with greater levels of dissection. Draf III improved delivery to the frontal sinus and was most synergistic with the head tilted forward 90°. No head position improved delivery after extended maxillary surgery or FESS. High-volume delivery in surgical patients outperformed low volume in all comparisons, although drops were also shown to be effective. 34,35
Patient Comfort
Two papers identified the HDF position as the most uncomfortable position for patients. 19,20 These findings mirror a study evaluating head positions based on patient discomfort. This study argued against using the HDF position due to discomfort and lack of strong evidence supporting its clinical effectiveness. 45 Although many of the papers reviewed reported increased distribution in the HDF position, especially to the frontal sinuses, discomfort may limit patient adherence.
Limitations
Although many studies discuss the effect of volume delivered, method of delivery, and surgery on the distribution of intranasal medication, our review found only 24 studies that compared 2 or more head positions and their effect on delivery of medications to the sinonasal cavity. The heterogeneity of data regarding method of delivery, surgery/dissections, head positions studied, and outcome metrics allows for limited comparison among studies. A majority of the studies utilized visual evaluation of intranasal distribution as a primary outcome; however, this may not correspond to the source of clinical symptoms and disease.
Conclusion
Many factors play a role in the delivery of intranasal medications, some of which are easily modified such as method or volume of delivery and head position. In surgery naive patients refractory to treatment, one can consider instillation of medication in the LHB position, which is more comfortable and may be as effective as the HDF position in improvement of symptoms. Further investigation of delivery to the paranasal sinuses in surgery-naive patients with CRS is warranted. For patients undergoing extended frontal sinus surgery, application of high-volume medication with head tilted 90° forward may be beneficial. Future studies should consider evaluation of delivery to anatomic regions and symptom control as metrics.
Supplemental Material
Supplemental Material, EAR_961004_supplement_1 - Positional Installation of Intranasal Corticosteroids in the Treatment of Chronic Rhinosinusitis: A Systematic Review of the Literature
Supplemental Material, EAR_961004_supplement_1 for Positional Installation of Intranasal Corticosteroids in the Treatment of Chronic Rhinosinusitis: A Systematic Review of the Literature by Emily L. Cummings, Scott N. Fassas, Kevin J. Sykes, Amy Sisson, Alexander G. Chiu and Meha G. Fox in Ear, Nose & Throat Journal
Footnotes
Acknowledgments
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.