
Abstract
Cricopharyngeal spasm and pharyngeal pouch can result in severe dysphagia symptoms that can have a significant impact on a patient’s quality of life. Several surgical interventions have been demonstrated including balloon dilatation, botox injection, and open and endoscopic cricopharyngeal myotomy. The aim of this case series is to describe our technique for endoscopic cricopharyngeal myotomy and compare pre- and postoperative swallowing outcomes using objective swallowing questionnaires in a small series of patients. Seven patients diagnosed with cricopharyngeal spasm or grade 1 pharyngeal pouch on barium swallow were prospectively observed. MD Anderson Dysphagia inventory (MDADI) and Dysphagia handicap index (DHI) were given to patients before and after their operation. All patients underwent the same surgical technique with the cricopharyngeal bar divided and the defect closed with dissolvable sutures. Mean inpatient stay was 7 days (range 1-8) and mean time to resumption of soft diet was 4 (range 1-7) days. All patients resumed oral diet before discharge. MDADI scores showed improvement across all domains, however only the emotional score achieved statistical significance (P = .04). Dysphagia handicap index scores showed a statistically significant improvement across functional, emotional, and total domains. Postoperative chest infection treated with oral antibiotics occurred in 3 patients (43%) and no other complications were documented. In conclusion, endoscopic cricopharyngeal myotomy with primary sutured endoscopic closure can result in a significant benefit to patient’s swallowing symptoms, emotional well-being, and quality of life.
Introduction
The cricopharyngeus muscle forms part of the inferior constrictor muscle of the pharynx, which along with the upper fibers of the esophagus creates the upper esophageal sphincter. 1 Through stimulation via the pharyngeal plexus of the vagus nerve, the muscle remains in a tonic state of contraction that protects against pharyngeal reflux and aerophagia. Cricopharyngeal spasm (CPS) occurs when there is uncoordinated or excessive muscle contraction in response to neuropathic, malignant, inflammatory, and idiopathic causes. 2 Typically, patients with CPS present with a spectrum of swallowing impairment, from mild swallowing difficulty and globus sensation to complete dysphagia with weight loss, aspiration, and a negative impact on quality of life. 2 Although there remains no clear consensus on etiology, a combination of CPS and anatomical weakness at Killian’s dehiscence can result in formation of pharyngeal pouch, 3 leading to worsening swallowing and aspiration symptoms in elderly patients.
Cricopharyngeal spasm can be managed with swallowing therapy, botulinum toxin injection, and bougie or balloon dilatation, with more permanent surgical intervention traditionally involving transcervical cricopharyngeal myotomy (CPM). Following Halvorson and Khun’s first description of endoscopic myotomy with a potassium-titanyl-phosphate laser, 4 the use of transoral approaches utilizing CO2 laser and monopolar diathermy have become popular. Despite this, there remains little unanimity on the optimal surgical technique for management of CPS, with some surgeons opting for myotomy with primary closure of the pharyngeal mucosa to minimize the risk of deep neck space and mediastinal complications.
The aim of this article is to discuss the surgical technique adopted in our Head and Neck Unit for endoscopic CPM with primary closure of the pharyngeal mucosa. In addition, we present postoperative outcomes in 7 patients who underwent endoscopic CPM and discuss the symptomatic, emotional, and functional effect this procedure can have on a patient’s quality of life through use of pre and postoperative swallowing questionnaires.
Case Series
Patient Cohort
Patient’s with symptoms suggestive of CPS or pharyngeal pouch including high dysphagia, globus pharyngeus, regurgitation, and choking episodes were prospectively identified from the outpatient clinic. Patients with suspected CPS or early pharyngeal pouch underwent flexible laryngoscopy to screen for obvious malignant or structural abnormalities contributing to dysphagia and routine barium swallow. Videofluoroscopy and esophageal manometry were not routinely performed. Patients with evidence of a prominent cricopharyngeal bar, upper esophageal dysmotility or early pharyngeal pouch on barium swallow who desired surgical intervention were consented for endoscopic CPM after discussion of risks and alternative management. All operations were performed by the same surgeon with a specialist interest in swallowing disorders at Charing Cross hospital, London.
Preoperatively, patients were asked to complete the MD Anderson Dysphagia inventory (MDADI) and Dysphagia handicap index (DHI) questionnaires. MD Anderson Dysphagia inventory contains 20 swallow-related questions scored from 1 to 5 on a Likert scale. Total points are calculated into a score out of 100 across 4 domains; global, physical, emotional and functional, with lower scores suggesting poorer swallowing outcomes. Dysphagia handicap index contains 25 questions split into 3 domains (physical, functional, and emotional) with patients ranking their symptoms from 1 (best) to 7 (worst). Scores are then totaled for each domain, with lower scores indicating a better swallow function. Patients were reviewed in the outpatient clinic at 3 months post-discharge, and were given the same swallow questionnaires. Statistical analysis comparing the median pre- and postoperative scores was performed with a Mann-Whitney U test with a result of P < .05 thought to be significant. No functional swallowing assessments were utilized in this study.
Our series contained 7 female patients with a median age of 72 years (range 52-88). Preoperative investigations diagnosed grade 1 pharyngeal pouch (3 patients), CPS (2 patients), and recurrent grade 1 pouch and CPS (1 patient each). Pharyngeal pouches were graded according to the Morton & Bailey classification system (grade 1, <2 cm; grade 2, 2-4 cm; grade 3, >4 cm). All patients described distressing dysphagia symptoms and tolerated a soft food diet only, although no patients required supportive enteral feeding. The cohort all underwent laryngo-pharyngo-esophagoscopy, injection of botox to cricopharyngeus and CPM with sutured primary closure. One patient underwent CO2 laser myotomy due to the presence of a cardiac pacemaker with the others undergoing division via monopolar diathermy. Two patients underwent concomitant balloon dilatation of the upper esophageal sphincter.
Surgical Technique
The patient is positioned supine under general anesthesia, with neck extension facilitated via a shoulder roll and the airway secured with a reinforced microlaryngoscopy endotracheal tube. A Dedo-Pilling Laryngoscope is used to identify the vocal cords and cricopharyngeus, to distinguish the posterior laryngeal commissure from the cricopharyngeal bar. The laryngoscope is put into suspension and 90 units (3 mL) of botulinum toxin type A is then injected into cricopharyngeus at 3 different points. Balloon dilatation can then be used to dilate from 15 to 18 mm.
A diverticuloscope is then put into suspension with blades either side of the cricopharyngeal bar. The microscope is deployed to more accurately visualize the cricopharyngeus and latterly aid placement of the endoscopic sutures. A 35-watt diathermy abbey needle with suction is then used to divide the cricopharyngeal mucosa. Underlying muscle fibers are subsequently identified and divided to the level of the prevertebral fascia. Haemostasis is then achieved with 1:1000 adrenaline soaked neuropatties.
A 5-0 polydioxanone suture on a cutting needle is then used to close the mucosa with interrupted sutures, without reapproximating muscle fibers. Sutures are placed with the aid of an endoscopic laryngeal needle holder and knots are secured with a Negus knot pusher. If using a pharyngoscope with a detachable inferior blade, this can be removed to allow for more space when placing sutures. Intraoperative photographs are shown in (Figure 1).
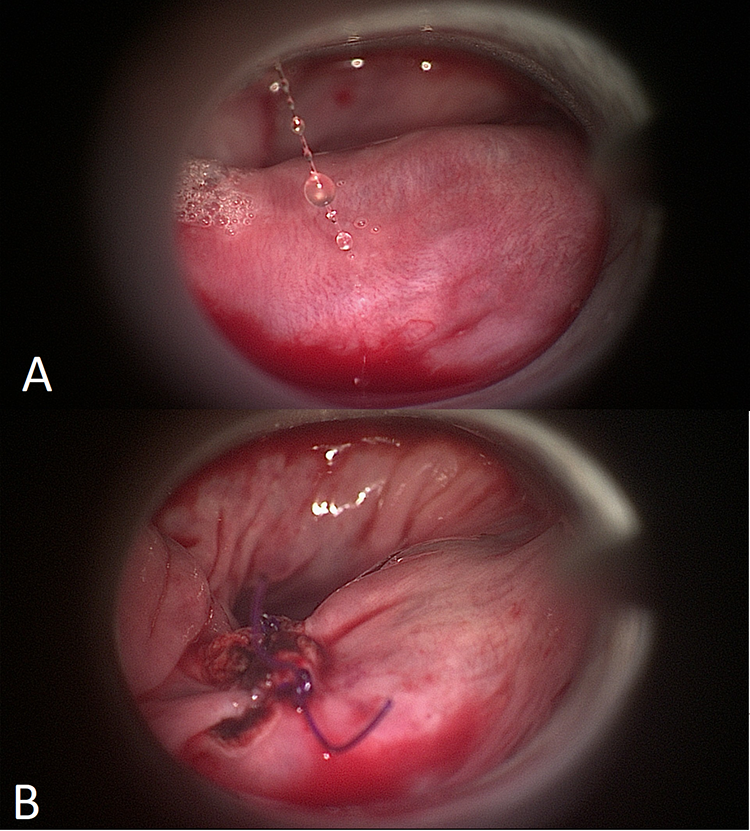
Clinical photographs showing endoscopic view of prominent cricopharyngeal bar. A, Shows the muscles fibers before division. B, Demonstrates the cricopharyngeal bar after division and reapproximation with endoscopic sutures.
A fine bore nasogastric (NG) tube is inserted at the end of the procedure under direct vision to supplement or replace oral feeding postoperatively. Postoperatively, the patient is kept nil by mouth for 2 hours and observed closely for signs or symptoms of mediastinitis. The patient is progressed onto clear fluids for the next 12 hours and oral intake can be built up onto solids the following day.
Results
Three patients resumed oral diet day 1 postoperatively (median age 72) with 4 patients requiring a period of NG feeding (median age 68). Median time to resumption of oral diet was 4 days (range 1-7 days). Median inpatient stay was 7 days (range 1-8 days) with all patients undergoing removal of NG tube and resumption of oral diet before discharge. Complications were not higher than grade II on the Clavien-Dindo classification: 3 patients (43%) had lower respiratory tract infections treated with first-line antibiotics. No other postoperative complications were reported. Median duration of follow-up is 5 months with no patients reporting symptom recurrence (Table 1).
Summary of Patient Demographic Data, Investigation Results, and Postoperative Outcomes.
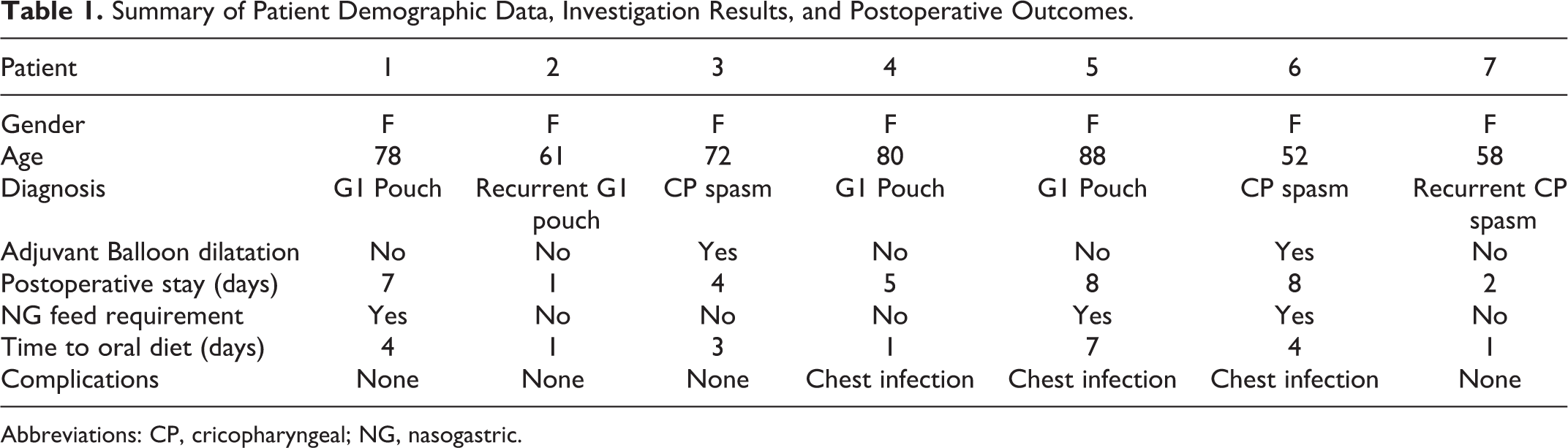
Abbreviations: CP, cricopharyngeal; NG, nasogastric.
MD Anderson Dysphagia inventory and DHI scores taken at 3 months post discharge revealed a global improvement across all facets of swallowing from patient baseline. Median MDADI scores increased across all domains, with global (40 vs 100, P < .2), physical (42.5 vs 65, P < .1), and functional issues (44.5 vs 76.7, P < .2) demonstrating a nonstatistically significant outcome, and changes to emotional symptoms (46.7 vs 76.7, P < .04) achieving statistical significance. Comparison of pre and postoperative median DHI scores revealed a statistically significant reduction in functional (44.5 vs 14, P < .05), emotional (37.5 vs 9, P < .04), and total (96.5 vs 29, P < .05) domains with a nonsignificant improvement in physical scores (19 vs 6, P < .08), in keeping with global improvement in swallowing function (Figures 2 and 3).
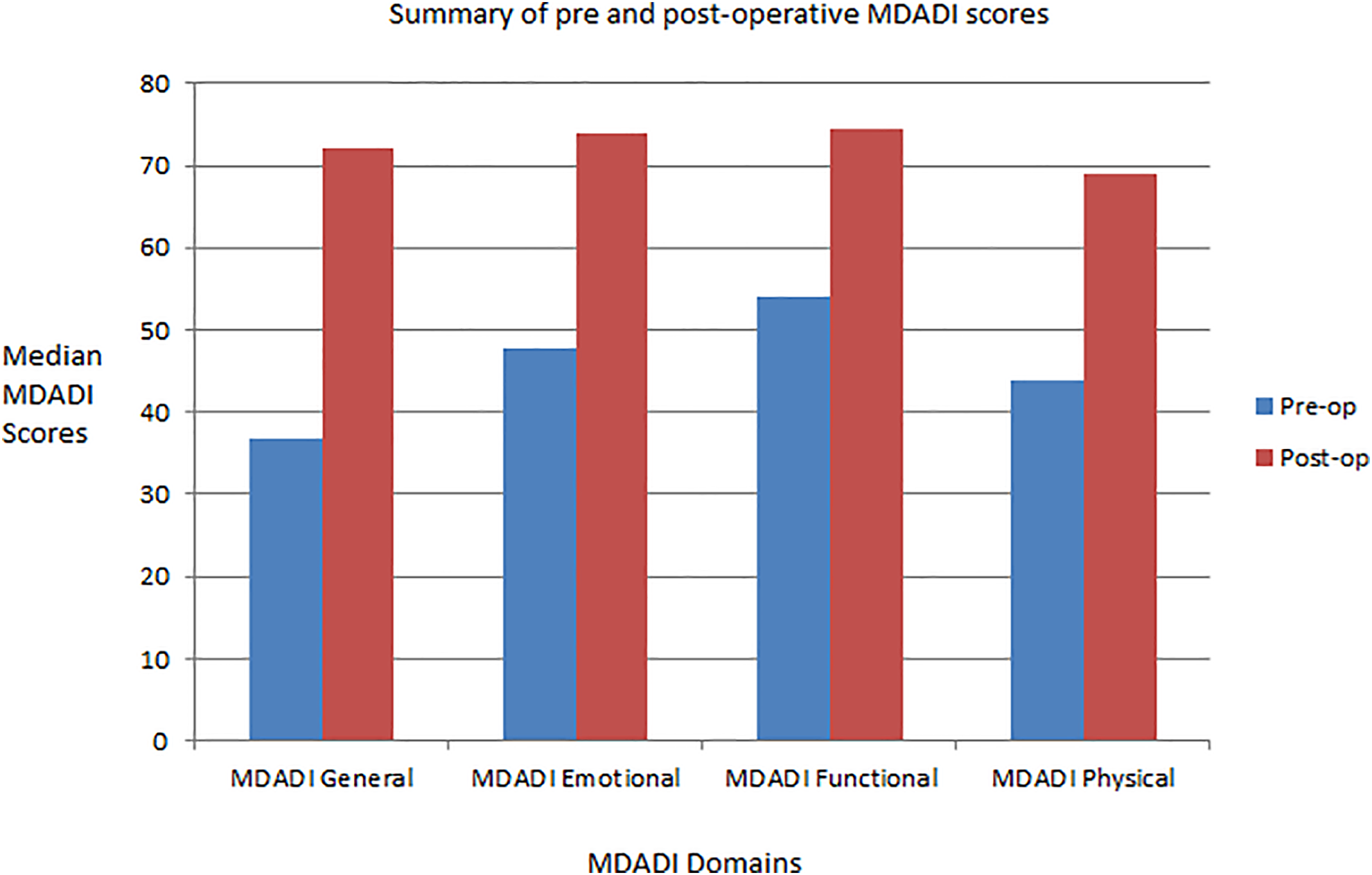
Chart summarizing the pre- and postoperative MD Anderson dysphagia inventory (MDADI) scores.
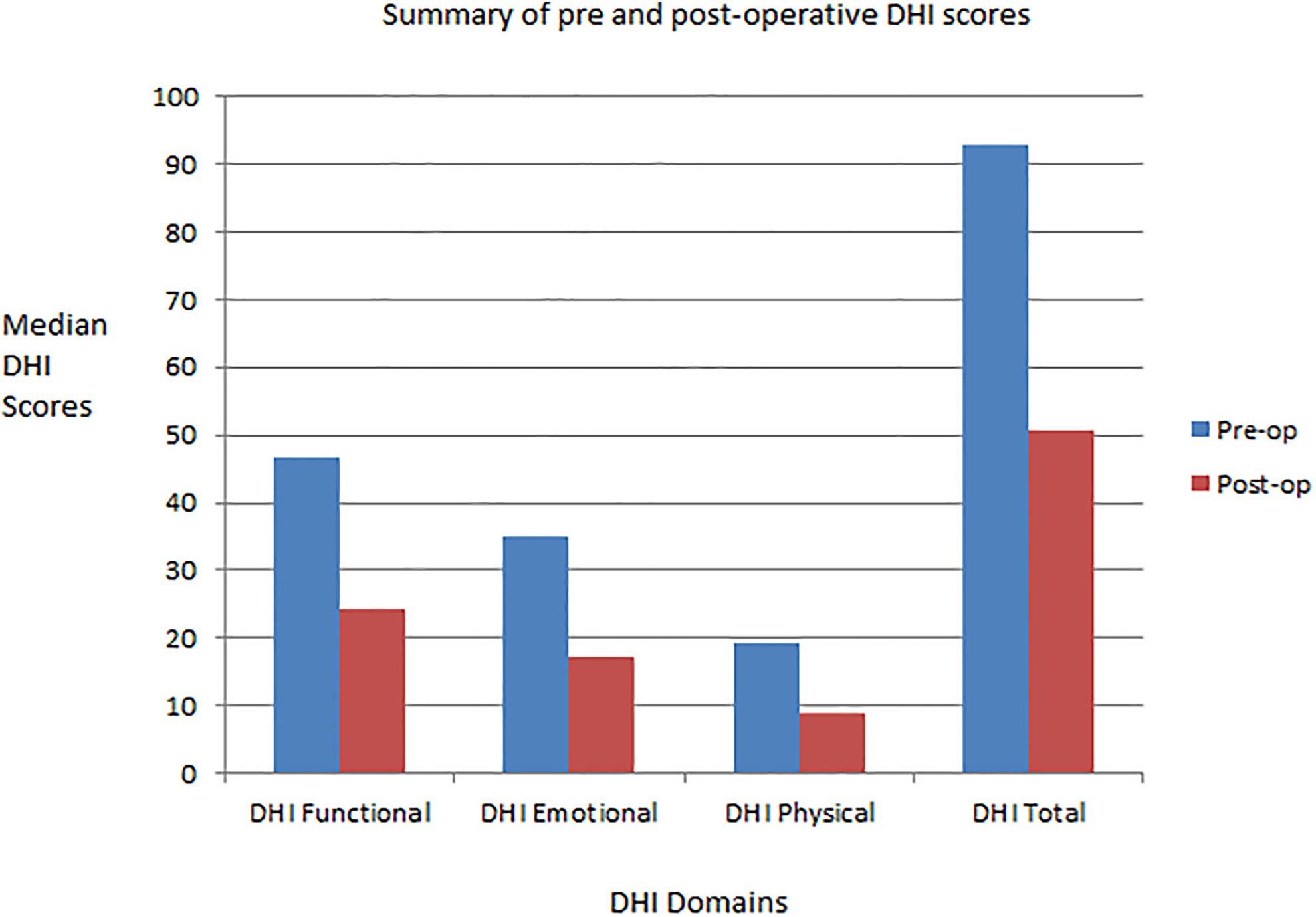
Chart summarizing the pre- and postoperative Dysphagia handicap index (DHI) scores.
Discussion
Cricopharyngeal Spasm and Myotomy
Cricopharyngeal spasm presents in elderly, comorbid patients with a spectrum of dysphagia severity. There is no agreed protocol for preoperative investigations and therefore the decision to operate is often determined by the impact quality of life, patient comorbidities, and surgeon and patient preference. Cricopharyngeal myotomy offers the only permanent improvement to dysphagia secondary to CPS and early pharyngeal pouch too small for endoscopic stapling, with video fluoroscopic studies demonstrating improved swallow through widening of the upper esophageal sphincter and reduction in the size of the pharyngeal diverticulum. 1
Certain series comparing CPM techniques have found the endoscopic approach to be at least as effective as open surgery, and may be the favored practice due to the reduced risk of complications such as pharyngocutaneous fistula, mediastinitis, and damage to the superior laryngeal nerve.2,5,6 However, an endoscopic approach does not entirely obviate these risks, as seen in a study of 38 open and 41 endoscopic CPM with primary closure which noted better functional outcomes in endoscopic patients, but found that significant complications including pharyngeal tear and fistula still occurred in both groups. 6 In a systematic review, Kocdor et al found a mean complication rate of 2% for endoscopic and 8% in open procedures across 15 studies. 2 Moreover, mean success rate was higher in the endoscopic group (83% vs 68%), implying it may be a safer and more effective treatment for CPS.
Dilatation and injection of botox confer a number of advantages over myotomy, as they can be repeated if effective, and can be performed under sedation or percutaneously for those unsuitable for general anesthetic. 2 However, both procedures only offer temporary improvements lasting between 0 and 24 months.2,7 Kocdor et al noted a success rate of 78% for CPM, which was statistically significant compared to botox injection (69%) but not against dilatation (73%). However, this review is hampered by combining open and endoscopic myotomy cohorts, heterogeneous outcome measures between studies, and containing few series on dilatation, making it difficult to draw satisfactory conclusions on the various treatment’s efficacy. Nevertheless, some authors advocate a 2 stage process; wherein frailer patients are offered a dilatation as a first-line therapy in order to avoid the morbidity of a myotomy, before offering definitive surgery in those who do not benefit from conservative measures. 8
Primary mucosal closure has been theorized to result in improved swallowing outcomes with reduced postoperative complications by sealing the retropharyngeal defect. This is evidenced by our cohort, which has shown an improvement across all swallowing domains with no major complications occurring. Ho et al reported a significant improvement in MDADI and functional outcome swallowing scales in 7 patients undergoing primary suture closure following endoscopic CPM, 9 however the authors performed a more limited myotomy compared to our technique, staying within buccopharyngeal fascia and not extending to the prevertebral space. Comparable improvements following primary mucosal closure were seen by Dale et al and Lawson et al, with no case series reporting any severe complications.10,11 This contrasts with Takes et al, who felt inflammation and scarring following CPM would close retropharyngeal defects, yet they reported free air on X-rays in 4/10 patients and surgical emphysema in 1 patient. 12 There are notable differences in the materials used for primary closure across studies with barbed knotless 6 and polyglactin sutures, 9 u-clips, 10 and fibrin glue 11 all being described with good functional outcomes and minimal complications.
There are a number of limitations to this series, with a small number of patients, short follow-up, variance in underlying pathology and surgical technique, and no comparison between patients with and without primary mucosal closure. A number of patients in this series were initially limited by pain necessitating NG feeding and several developed postoperative chest infections. Nevertheless, this may be reflective of an elderly and comorbid cohort, where a single definitive procedure may be preferable to a traumatic open operation or repeat anesthetics for temporary procedures. Finally, endoscopic placement of mucosal sutures presents a slight technical challenge, which may be heightened by anatomical issues that impede insertion of the pharyngoscope such as c-spine fixation and neck habitus.
Advantages of Surgical Technique
The modified technique described confers a significant advantage as it allows complete division of the cricopharyngeus muscle down to the level of the prevertebral fascia, without risking injury to the recurrent laryngeal nerve and inferior thyroid vessels necessary in transcervical dissections. Closure of the mucosa seals access to the retropharyngeal space, thus restoring the integrity of the pharyngeal wall and reducing the risk of surgical emphysema, deep neck space abscess, and mediastinal infections.
Although pain was a limiting factor in several of our patients, it has been hypothesized that primary closure can improve postoperative pain and therefore reduce hospital stay and reliance on NG feeding. 11 Additionally, an endoscopic approach may be better tolerated in frail and elderly patients, with reduced anesthetic time and a more rapid postoperative recovery significantly reducing the risk of perioperative complications.
Conclusions
This series has demonstrated CPM with primary mucosal closure is safe and can result in a significant functional improvement in patients with dysphagia secondary to CPS and early pharyngeal pouch. The technique described allows complete division of the cricopharyngeus while minimizing the risk of deep neck space complications which can carry significant morbidity in elderly patients. With careful postoperative monitoring, the procedure can therefore be employed as a first-line treatment for primary and recurrent CPS and pharyngeal pouch.
Footnotes
Author's note
Andrew Williamson and Zaid Awad, are also affilaited to Imperial College London, Exhibition Road, London SW7 2AZ.
Acknowledgments
The speech and language therapy team at NHS Imperial College healthcare for their advice and management of several patients in the case series.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.