
Abstract
This report outlines the treatment of an 82-year-old man with squamous cell carcinoma of the left cheek. The wide excision and simultaneous superficial parotidectomy were planned. Various incision methods have been widely introduced such as retroauricular hairline incision, modified Blair incision, or face-lift incision. For coverage of preauricular skin defect and parotidectomy, we modified retroauricular hairline incision that the end of the incision was bent to make transposition flap. The operation has been successfully finished using this extension of a retroauricular hairline incision.
Introduction
Partial superficial parotidectomy (PSP) is a widely used surgical technique that can lower parotid tumor recurrence rates and preserve facial nerves without complications. 1 With the popularization of this technique, various incision methods have been widely introduced and researched. The appropriate incision is chosen based on tumor location, the surgeon, or patient’s preference, sex, and age. A retroauricular hairline incision (RAHI), modified Blair incision (MBI), or face-lift incision (FLI) is used.2,3
These incision techniques were developed for effective access to the parotid area and minimal scarring. In the past 2 decades, MBI was the most common incision for parotidectomies. However, due to a significantly long scar, FLI and RAHI have recently become more common.4,5 Despite these recent surgical techniques allowing adequate excess to the parotid area with minimal scarring, there could be unique cases with an accompanying preauricular skin defect that should be covered with a flap. If the preauricular skin defect is covered with a skin graft, there could be a permanent and intolerable postoperative scar on the patient’s cheek.
Therefore, we need a modified incision technique that makes PSP simple and safe and covers the preauricular skin defect. Several patients underwent PSP with a retroauricular transposition flap and healed well. Here, we report this modified PSP incision method.
Case Report
An 82-year-old man visited our clinic due to a mass in the left cheek. The mass was a 4.5 cm × 5.5 cm black crusted papule (Figure 1). The mass occurred 2 years prior and was diagnosed as squamous cell carcinoma by incisional biopsy. Whole-body screening did not indicate any distant metastases. A wide excision with PSP was planned for the malignancy because preoperative computed tomography showed a deeper invasion of the parotid fascia. The procedure was performed with general anesthesia and the operative field included exposing a wide retroauricular area. After planning a wide surgical margin of the skin malignancy, an additional retroauricular incision was planned for the PSP and coverage of the anticipated defect. In the retroauricular area, the incision line was designed similarly to RAHI. The end of the incision was a bent line designed for a transposition flap (Figure 2). After a wide excision of the malignancy and PSP, the designed transposition flap was elevated for coverage and the donor site was covered with a skin graft (Figure 3A and B). The patient healed without complications after he was discharged from the hospital.

Wide excision of the black-crusted papule in the left cheek was planned.
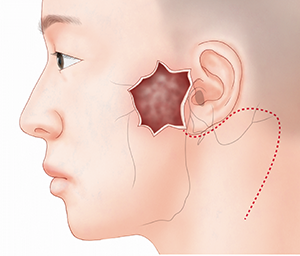
Extension of a retroauricular hairline incision was designed for coverage of preauricular skin defect and parotidectomy.
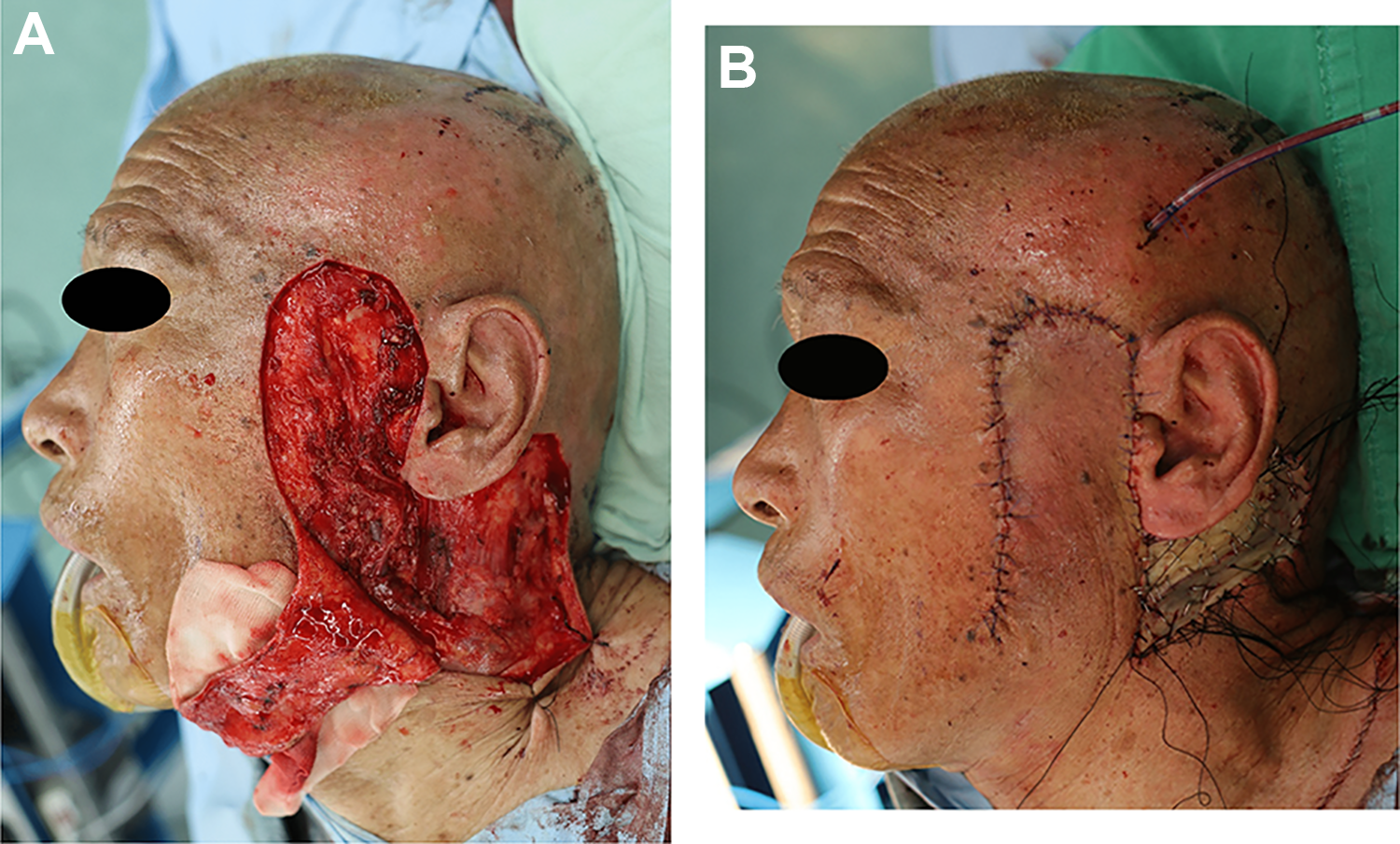
Wide retroauricular flap using extension of the retroauricular hairline incision was elevated (A) and the donor site was covered with full-thickness skin graft (B).
Discussion
Preauricular skin defects are sometimes a challenging problem because there are no definite surgical techniques for their treatment. If the defect is larger, a simple local flap is not possible due to high tension in the area. A full- or partial-thickness skin graft can be used; however, these grafts could lead to color mismatch as well as an undesirable scar contracture. 6 Even if the defect is caused by a parotidectomy, a skin graft may cause facial nerve irritability or Frey syndrome.
Of course, there are some recommended flaps for preauricular skin defects. An island flap or V-Y advancement flap using the inferior flap of the defect can be used; however, these flaps require adequate free movement to reduce tension. This could lead to extensive dissection and may cause flap necrosis. For large defects, a face-lift flap or cervicofacial rotation flap can be used; however, these flaps are invasive and require a large incision line.7,8
We recommend the increased use of the retroauricular transposition flap using the resulting incision line from the parotidectomy. The retroauricular area has a clear advantage as the donor site because it is a nonexposed area and there is low chance of necrosis due to the flap having a wide base at the neck. Our patient has no complaints about a wide scar at the donor site. However, if the patient was younger or sensitive to scar formation, a bilobed or trilobed flap using the posterolateral neck area could be possible. In addition to that, if the burrow triangle for transposition flap is large enough, the excised skin can be good donor skin for skin graft. Although this flap has a large incision, it can make easy coverage without tension compared with FLI.
If the defect occurs in the preauricular area and additional parotidectomy is needed, using a retroauricular transposition flap using an extension of the RAHI could be feasible for stable and easy coverage of the defect. Here, we reported a patient with skin cancer of the preauricular area who is in remission following a retroauricular transposition flap after wide excision and PSP.
Footnotes
Authors’ Note
This is the first submission on this topic and this research has not been presented at a scientific meeting.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.