
Abstract
We describe the first case of ethmoid metastasis from an oropharyngeal human papillomavirus–induced squamous cell carcinoma using the anti-P16 immunohistochemistry. The p16 overexpression can be a valuable aid in the differential diagnosis.
Case Report
We report the case of a 67-year-old woman who has been followed in our department for dysphagia and oropharyngeal pain 2 years ago. An oropharyngeal human papillomavirus–induced squamous cell carcinoma (OSCC-HPV+) classified cT4bN2cM0 was diagnosed and managed by concomitant radio-chemotherapy by our oncology department. The extension assessment including a positron emission tomography computed tomography (PET-CT) did not show metastatic extension or sinus filling.
Two years later, the patient presented with recurrent left sinusitis in the form of nasal obstruction and purulent rhinorrhea. After medical treatment with antibiotic therapy failed, an imaging assessment CT scan and MRI demonstrated an ethmoidal mass (Figures 1 and 2).

Axial contrast CT scan of the head shows a heterogeneous mass in the anterior and posterior ethmoid sinus eroding through the basal lamella of the middle turbinate and involving the sphenoid sinus posteriorly. CT indicates computed tomography.
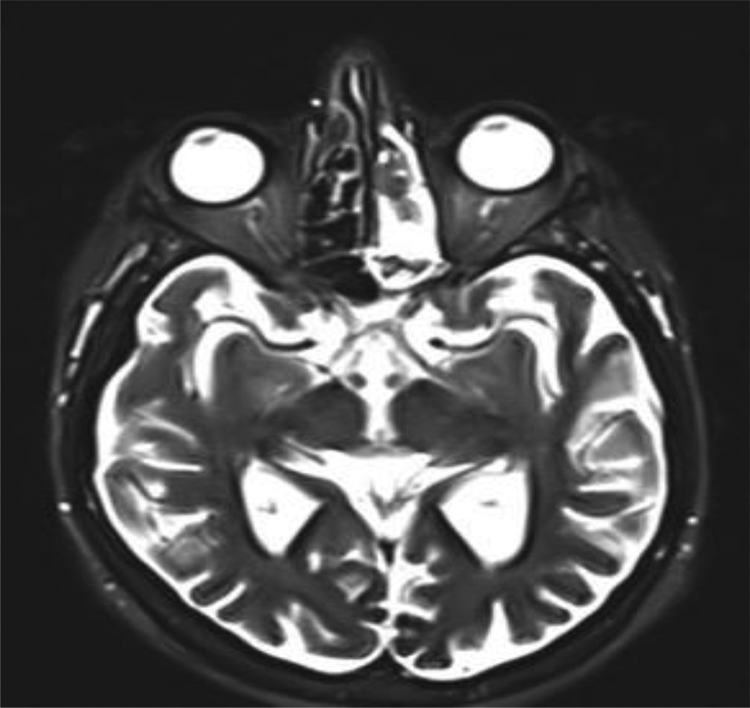
Axial T2-weighted brain MRI showing a large, heterogeneous mass involving the left ethmoid air cells and left sphenoid sinus.
We decided to perform a left middle meatotomy and a left ethmoidectomy was scheduled. During the intervention, a left ethmoidal mass was quickly identified and biopsied. Histological analysis demonstrated the presence of a squamous cell carcinoma (SCC) positive for anti-p16 immunohistochemical labeling with one hundred percent of the cells labeled (Figure 3).
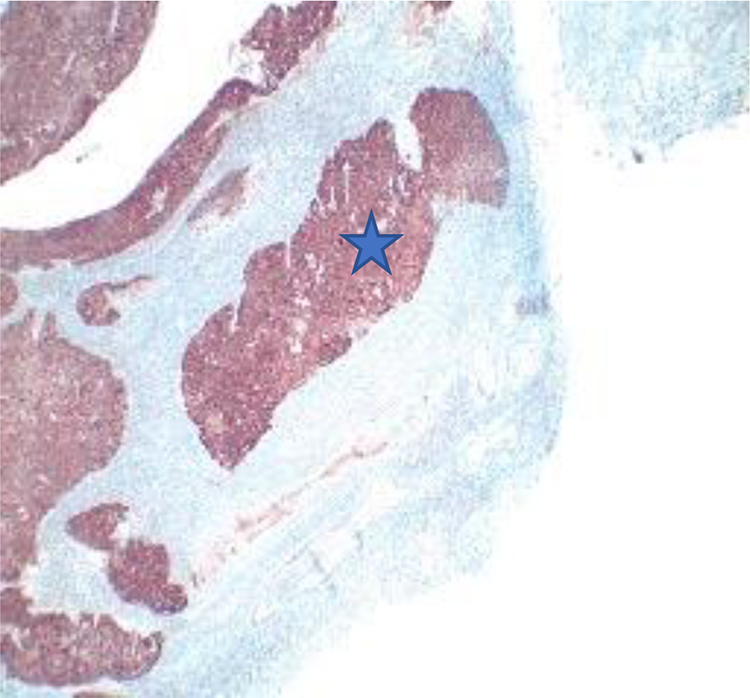
Histological section showing 100% of the squamous cell carcinoma marked by P16 immunohistochemistry.
After discussion at a multidisciplinary oncological meeting, the diagnosis of metachronous metastasis of OSCC-HPV+ was made and a complete endoscopic resection associated with adjuvant radiotherapy was carried out. A new extension assessment by PET-CT did not demonstrate any other metastatic location. After the treatment and until this day, the patient did not present any recurrence of her cancer.
Discussion
Although neoplasia is a differential diagnosis for paranasal sinus and orbit occupying lesion, it remains extremely rare sites for distant metastasis. The most common primary tumor metastasizing by hematogenous spread to paranasal sinuses and orbit is renal carcinoma, followed by lung, thyroid, ductal breast, and prostate carcinoma.1,2
The most common site for distant metastasis of OSCC is the lungs. Extra-thoracic distant metastases, for example, to metastases to bone, liver, or brain remaining rare. 3
However, some studies have highlighted a different mechanism of metastatic dissemination for OSCC-HPV+. They especially suggest that this cancer has a predilection toward active invasion of the vasculature and other atypical metastatic sites, 4 including a preference for bone. 5
In our case, different diagnoses could be evoked and particularly the inverted papilloma and the primitive SCC of the ethmoid sinus, which can also be p16 positive. What allowed us to differentiate a metastasis of OSCC HPV+ from a primitive SCC of the ethmoid or from an inverted papilloma is the percentage of p16 labeling of the tumor.
Although some studies have indeed shown that inverted papilloma can also have p16 immunostaining, the difference lies in the percentage of p16 labeling. According to the latest oropharyngeal SCC literature, p16 is considered positive when its overexpression is above 70%.6-8 In inverted papilloma, p16 overexpression is significantly lower than 70%, as shown in the last study where average fixation of p16 was 11.3% for normal inverted papilloma and 14% for inverted papilloma with carcinoma. 9 Another argument to reject this diagnosis is that at the first imaging assessment there was no tumor in the ethmoid.
Conclusion
We have described the first case of ethmoid metastasis from an OSCC HPV+ using the anti-P16 immunohistochemistry. This marker can be a valuable aid in the differential diagnosis.
Footnotes
Authors’ Note
This article should have been presented during the spring meeting of royal Belgian society of oto-rhino-laryngology, head and neck surgery (March 21, 2020); because of the coronavirus pandemic, this meeting will take place at a later date. We received the patient’s consent as well as the agreement of the ethics committee for the publication of this case report.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.